CONTACT TRACING
FOR AIR TRAVEL
CDC’s Data System
Needs Substantial
Improvement
Report to Congressional Addressees
July 2022
GAO-22-105018
United States Government Accountability Office

United States Government Accountability Office
Highlights of GAO-22-105018, a report to
congressional addressees
July 2022
CONTACT TRACING FOR AIR TRAVEL
CDC’
s Data System Needs Substantial Improvement
What GAO Found
The Centers for Disease Control and Prevention (CDC) plays a key role in
contact tracing for air travel—the process of identifying and notifying passengers
who may have come into contact with a person infected with a communicable
disease during a flight. However, several factors affect CDC’s ability to collect
timely, accurate, and complete air passenger information to support contact
tracing by local public health authorities. For example, airlines may not have
accurate and complete information about passengers to share with CDC
because the contact information provided to book a ticket may be for a third
party, like a travel agent, not for passengers. Further, because no single,
complete, and reliable source of passenger information exists, CDC often
conducts research to fill in gaps, extending the time it takes to share information
with local public health authorities.
Overview of Process for Collecting Air Passengers’ Contact Information
Since the start of the COVID-19 pandemic, CDC has taken some actions to
improve the quality of information it collects. For example, since November 2021,
CDC has required airlines to collect certain information—including name, phone
number, email, and physical address—no more than 72 hours before departure
from passengers traveling on flights into the United States and to transmit the
information to CDC in a defined format.
However, limitations in how CDC collects and manages air passengers’ contact
information—including CDC’s use of an outdated data management system—
hinder the agency’s ability to monitor public health risks and facilitate contact
tracing. The data management system—developed in the mid-2000s—was not
designed for rapid assessment or aggregation of public health data across
individual cases. For example, CDC is unable to quickly and accurately identify
the number of passengers exposed to a specific infected passenger on a flight.
Nor does the system contain the necessary data fields to assess the quality of air
passenger information CDC receives, such as a field to determine the timeliness
of airlines’ responses to CDC’s request. Consequently, CDC is not positioned to
efficiently analyze and disseminate data to inform public health policies and
respond to disease threats. Nor is it positioned to evaluate its performance in
collecting and sharing quality passenger information.
View GAO-22-105018. For more information,
contact
Heather Krause at (202) 512-2834 or
.
Why GAO Did This Study
The COVID
-19 pandemic has
underscored the importance of public
health measures
aimed at controlling
the transmission of communica
ble
disease
s. Air travel can play a role in
quickly spreading communicable
diseases across the world and
throughout communities. Given this
potential, c
ontact tracing for air
passengers
is an important measure
for protecting
public health.
GAO was asked to examine CDC’s
process for collecting and managing air
passenger
s’ contact information to
facilitate contact tracing.
This report
addresses
: (1) the factors that affect
CDC
’s ability to collect this information
,
(
2) recent actions CDC has taken to
improve the quality of the information it
collects
, and (3) how effectively it
collects and
manages this information.
GAO reviewed
relevant federal
documentation
, including regulations,
orders, technical gu
idance, and public
comments
, as well as available CDC
data
. GAO also interviewed officials
from CDC,
U.S. Customs and Border
Protection
, and the Federal Aviation
Administration,
and selected
representatives from
the aviation,
travel, and public health
industries.
What GAO Recommends
GAO is making
three
recommendations, including that
CDC
redesign
its data management system
for air passenger information
or deploy
a new one
. CDC concurred with the
recommendations.
Page i GAO-22-105018 Contact Tracing for Air Travel
Letter 1
Background 4
Multiple Factors Impede CDC’s Collection of Timely, Accurate,
and Complete Passenger Information 11
CDC Has Made Some Improvements to the Quality of Air
Passenger Information It Collects for Inbound International
Travel 15
Unaddressed Limitations in How CDC Collects and Manages Air
Passengers’ Information Hinder Contact Tracing 19
Conclusions 29
Recommendations for Executive Action 30
Agency Comments 30
Appendix I Objectives, Scope, and Methodology 34
Appendix II Comments from the Department of Health & Human Services 41
Appendix III GAO Contact and Staff Acknowledgments 44
Figures
Figure 1: Overview of Process for Collecting Air Passengers’
Contact Information to Support Contact Tracing 8
Figure 2: Examples of Air Passengers Seated in Proximity to an
Infected Passenger, Potentially Warranting a Contact
Investigation, according to CDC Protocols 9
Figure 3: Illustration of CDC’s Reliance on Manual Entry to
Process Air Passenger Contact Information into Its
Quarantine Activity Reporting System 21
Contents

Page ii GAO-22-105018 Contact Tracing for Air Travel
Abbreviations
APIS Advance Passenger Information System
ATS Automated Targeting System
CBP U.S. Customs and Border Protection
CDC Centers for Disease Control and Prevention
DHS Department of Homeland Security
DOT Department of Transportation
FAA Federal Aviation Administration
HHS Department of Health and Human Services
ICAO International Civil Aviation Organization
MERS Middle East Respiratory Syndrome
MOU memorandum of understanding
NNDSS National Notifiable Diseases Surveillance System
OMB Office of Management and Budget
QARS Quarantine Activity Reporting System
SARS severe acute respiratory syndrome
USCIS U.S. Citizenship and Immigration Services
WHO World Health Organization
This is a work of the U.S. government and is not subject to copyright protection in the
United States. The published product may be reproduced and distributed in its entirety
without further permission from GAO. However, because this work may contain
copyrighted images or other material, permission from the copyright holder may be
necessary if you wish to reproduce this material separately.

Page 1 GAO-22-105018 Contact Tracing for Air Travel
441 G St. N.W.
Washington, DC 20548
July 11, 2022
Congressional Addressees
The introduction and spread of COVID-19 throughout the United States
has underscored the importance of public health measures aimed at
controlling the transmission of communicable diseases. Responsibility for
protecting the health of the public from communicable diseases rests
heavily with state and local public health authorities. With regard to air
travel into the United States and between states, however, federal
agencies and the Centers for Disease Control and Prevention (CDC), in
particular, play a unique role in helping prevent or mitigate disease
transmission. Contact tracing for air passengers is the process of
identifying and notifying persons who may have come into contact with a
person infected with a communicable disease during a flight. It is one
public health measure that is particularly important because of air travel’s
known potential to quickly spread communicable diseases across the
world and throughout communities. For example, several studies have
reported that the introduction and initial spread of COVID-19 throughout
the United States was tied to air travel.
1
However, CDC has faced long-standing challenges to collecting and
sharing timely, accurate, and complete contact information for air
passengers with local public health authorities to facilitate contact
1
See for example: Jeffrey Prince and Daniel H. Simon, The Effect of International Travel
on the Spread of COVID-19 in the U.S. (Dec. 21, 2020), Kelley School of Business
Research Paper No. 2021-02, available at SSRN: https://ssrn.com/abstract=3753069 or
http://dx.doi.org/10.2139/ssrn.3753069;Christopher A. Mouton et al., COVID-19 Air Traffic
Visualization: By January 31, 2020, at Least 1.5 Daily Infected Passengers Were
Originating in China. Santa Monica, CA: RAND Corporation, 2020,
https://www.rand.org/pubs/research_reports/RRA248-2.html; and Michel Bielecki et al.,
“Air travel and COVID-19 prevention in the pandemic and peri-pandemic period: A
narrative review,” Travel medicine and infectious disease, vol. 39 (2021): 101915.
doi:10.1016/j.tmaid.2020.101915.
Letter

Page 2 GAO-22-105018 Contact Tracing for Air Travel
tracing.
2
The ability of public health authorities to quickly contact
potentially exposed passengers to advise them on post-exposure actions,
such as testing or quarantining, is critical to stopping the chain of disease
transmission. Inaccurate or incomplete contact information may delay or
even preclude notifying an exposed passenger, potentially leading to
broader community spread of a disease.
These challenges have been exacerbated by the ongoing COVID-19
global pandemic. For example, CDC officials estimated that the number
of flights warranting a contact investigation in 2020 increased more than
10,000 percent from 2019—taxing the aviation and public health sectors’
systems and resources.
The CARES Act includes a provision for us to report on our ongoing
monitoring and oversight efforts related to the COVID-19 pandemic.
3
This
report is a part of that body of work.
4
We also were asked to examine
CDC’s process for collecting and managing air passenger contact
information to facilitate contact tracing. This report addresses:
• the factors that affect CDC’s ability to collect timely, accurate, and
complete air passenger contact information from airlines and other
sources;
2
For example, in 2004, we reported on CDC’s challenges in collecting timely and complete
passenger information during the 2003 severe acute respiratory syndrome (SARS)
outbreak. Following that report, CDC proposed—though never finalized—a rule to expand
requirements that airlines collect designated pieces of information for passengers traveling
on both international inbound and domestic interstate flights and transmit that information
to CDC within 12 hours of request. See GAO, Emerging Infectious Diseases: Asian SARS
Outbreak Challenged International and National Responses, GAO-04-564 (Washington,
D.C.: Apr. 28, 2004). Also, as discussed later in this report, CDC issued, in February
2020, an Interim Final Rule requiring airlines to, in response to a CDC order, collect and
provide CDC with five designated pieces of information for passengers traveling on
inbound international flights. Control of Communicable Diseases; Foreign Quarantine, 85
Fed. Reg. 7874 (Feb. 12, 2020) (codified at 42 C.F.R. § 71.4(d)–(e)).
3
Pub. L. No. 116-136, § 19010, 134 Stat. 281, 579-81 (2020).
4
We regularly issued government-wide reports on the federal response to COVID-19. For
the latest report, see GAO, COVID-19: Current and Future Federal Preparedness
Requires Fixes to Improve Health Data and Address Improper Payments,
GAO-22-105397 (Washington, D.C.: Apr. 27, 2022). Other government-wide reports on
this topic are available on GAO’s website at https://www.gao.gov/coronavirus.

Page 3 GAO-22-105018 Contact Tracing for Air Travel
• the actions CDC has taken since the onset of the COVID-19
pandemic to improve the quality of air passenger contact information it
collects; and
• how effectively CDC collects and manages air passenger contact
information to facilitate contact tracing.
To conduct this work, we reviewed relevant statutes and regulations
pertaining to contact tracing for air travel. We also assessed the activities
of the three key federal departments with roles in facilitating contact
tracing for potentially exposed air passengers—the Department of Health
and Human Services (HHS); Department of Homeland Security (DHS);
and Department of Transportation (DOT)—as well as their relevant
components, including HHS’s CDC, DHS’s U.S. Customs and Border
Protection (CBP), and DOT’s Federal Aviation Administration (FAA). And,
we interviewed officials from four of the 20 CDC regional quarantine
stations: Atlanta (Hartsfield-Jackson Atlanta International Airport);
Chicago (O’Hare International Airport); Los Angeles (Los Angeles
International Airport); and San Francisco (San Francisco International
Airport).
5
We selected these quarantine stations based on the volume of
international and domestic passengers at the airport co-located with the
quarantine station, among other factors.
To identify and obtain perspectives on factors affecting CDC’s ability to
collect timely, accurate, and complete passenger contact information, in
addition to speaking with officials from identified agencies, we interviewed
or received written responses from six selected U.S. commercial
passenger airlines: American Airlines, Delta Air Lines, JetBlue Airways,
Southwest Airlines, Spirit Airlines, and United Airlines. We selected these
airlines based on passenger volumes and seating practices, among other
characteristics. We also interviewed representatives from four industry
groups representing the aviation sector, two associations representing
local public health authorities, and three travel industry organizations to
obtain broader stakeholder perspectives on contact tracing for aviation.
To describe CDC’s actions since the onset of the COVID-19 pandemic to
improve the quality of air passenger contact information it collects and
manages, we reviewed regulatory documents including CDC’s 2020
Interim Final Rule for the Control of Communicable Diseases, as well as
associated implementing orders, technical instructions, and submitted
5
CDC quarantine stations are located at 20 ports of entry and land-border crossings
where most international travelers arrive. Eighteen of the 20 stations are located at
international airports.

Page 4 GAO-22-105018 Contact Tracing for Air Travel
public comments. In addition, we reviewed applicable CBP documents
describing the expansion of coordination efforts between CDC and CBP
in collecting information for passengers traveling on flights to the United
States.
We assessed CDC’s ability to effectively collect and manage air
passenger contact information against 1) CDC guidance for maintaining
and using public health data to inform agency activities and respond to
disease events; 2) the Office of Management and Budget’s (OMB)
Federal Data Strategy; 3) federal internal control standards related to
data entry, information processing and information system design, and
program monitoring; and 4) leading practices GAO has previously
identified for program evaluation and performance measurement and
evaluation. As part of our assessment, we reviewed a sample of data
from and available documentation on CDC’s Quarantine Activity
Reporting System (QARS) and interviewed CDC officials. Additional detail
on the scope and methodology of our review is contained in appendix I.
We conducted this performance audit from February 2021 to July 2022 in
accordance with generally accepted government auditing standards.
Those standards require that we plan and perform the audit to obtain
sufficient, appropriate evidence to provide a reasonable basis for our
findings and conclusions based on our audit objectives. We believe that
the evidence obtained provides a reasonable basis for our findings and
conclusions based on our audit objectives.
The COVID-19 global pandemic has renewed concerns about the spread
of communicable diseases through air travel, as well as about the U.S.
aviation system’s preparedness to respond to such threats.
6
As of June
2022, more than 86 million cases of COVID-19 had been reported in the
6
In 2015, we reported on the preparedness of the U.S. aviation system to respond to
pandemics and other health crises. We recommended that the Secretary of Transportation
work with relevant stakeholders, including HHS, to develop a national aviation-
preparedness plan for communicable diseases. In June 2020, we urged Congress to take
legislative action to require DOT to develop a national aviation-preparedness plan. As of
March 2022, according to agency officials, DOT plans to take the lead, working closely
with HHS and DHS, in developing such a plan building upon the Runway to Recovery and
guidance materials from the International Civil Aviation Organization. According to
officials, DOT intends to complete and implement the preparedness plan in 2023. See
GAO, Air Travel and Communicable Diseases: Comprehensive Federal Plan Needed for
U.S. Aviation System’s Preparedness, GAO-16-127 (Washington, D.C.: Dec. 16, 2015)
and GAO, COVID-19: Opportunities to Improve Federal Response and Recovery Efforts,
GAO-20-625 (Washington, D.C.: June 25, 2020).
Background

Page 5 GAO-22-105018 Contact Tracing for Air Travel
United States, resulting in more than 1 million deaths.
7
More than any
other mode of transportation, air travel creates the potential for infectious
diseases to move quickly from one part of the world to another. Beginning
with the 2003 severe acute respiratory syndrome (SARS) epidemic, a
number of communicable disease threats—such as the 2009 H1N1
influenza pandemic, the 2012 Middle East Respiratory Syndrome (MERS)
outbreak, and the 2014 Ebola Virus Disease outbreak—have raised
concerns regarding international transmission of diseases from travel.
The SARS epidemic was the first major new disease of the 21st century,
according to the World Health Organization (WHO) of the United Nations.
WHO described that 2003 epidemic as a watershed event because it
revealed how much impact communicable diseases can have in a highly
mobile and interconnected world.
8
Contact tracing is a key public health measure to help control the
transmission and spread of communicable diseases. When implemented
effectively, contact tracing separates the people who have, or may have,
a communicable disease from those who do not by identifying infected
individuals, notifying their “contacts”—all the people they may have
transmitted the disease to—and communicating information on measures,
such as getting tested or quarantining, that potentially exposed contacts
should take.
In the United States, contact tracing investigations and notifications are
primarily carried out by state and local public health authorities. Yet in the
case of contact tracing for passengers potentially exposed while flying
into the country or between states, several federal agencies, the airline
industry, and international organizations also play a role in supporting
state and local public health authorities. Specifically:
7
Data on COVID-19 cases in the U.S. are based on aggregate case reporting to CDC and
include probable and confirmed cases as reported by states and jurisdictions. CDC
COVID-19 counts are subject to change due to delays or updates in reported data from
states and jurisdictions. According to CDC, the actual number of COVID-19 cases is
unknown for a variety of reasons, including that people who have been infected may have
not been tested or may have not sought medical care. See CDC, “COVID Data Tracker:
Trends in Number of COVID-19 Cases and Deaths in the US reported to CDC, by
State/Territory,” accessed June 22, 2022, https://covid.cdc.gov/covid-data-
tracker/#datatracker-home.
8
World Health Organization, Outbreak Communication: Best practices for communicating
with the public during an outbreak. (Singapore: Sept. 21–23, 2004). Report of the WHO
Expert Consultation on Outbreak Communications.
Contact Tracing Roles and
Responsibilities
Page 6 GAO-22-105018 Contact Tracing for Air Travel
• HHS has statutory authority to make and enforce regulations to
prevent the introduction, transmission, and spread of communicable
diseases into the United States and between states.
9
Within HHS,
CDC is responsible for public health surveillance, which is the
ongoing, systematic collection, analysis, interpretation, and
dissemination of data regarding health-related events to inform public
health policies and respond to disease threats. As part of this
surveillance, staff and contractors within CDC’s Division of Global
Migration and Quarantine in its headquarters and 20 regional
quarantine stations spearhead the collection of air passenger contact
information from airlines and other sources. Subsequently, CDC
provides this information to state and local public health authorities to
carry out their contact tracing investigations.
• CBP—through a memorandum of understanding between HHS and
DHS
10
—supports CDC by sharing information on passengers
traveling into the United States that the agency already collects from
airlines and other federal agencies for the purpose of CBP’s mission
at ports of entry.
11
Of the information that CBP collects, it provides
CDC with those elements that are relevant to responding to a public
health threat.
• FAA, while not directly involved with collecting or sharing passenger
contact information, regulates aviation safety, including safety of
airlines, which provide CDC with passenger information. In addition,
given FAA’s knowledge of the aviation sector, it has played a key role
in coordinating with relevant stakeholders, including CDC, CBP, and
airlines, in responding to public health threats in areas that relate to
air travel.
9
42 U.S.C. § 264(a).
10
In 2005, HHS and DHS signed a memorandum of understanding (MOU) that
documented CBP’s support of CDC in providing information for travelers arriving by air
into the United States. Under this MOU, CBP provides CDC with selected passenger
information that it collects for the purpose of CBP’s mission at the border and that is also
deemed useful to CDC, under the MOU, in preventing the introduction, transmission, and
spread of communicable diseases into and within the United States.
11
In the United States, a port of entry is an officially designated location (airport, seaport,
or land-border location) where DHS officers or employees are assigned to clear
merchandise, collect duties, and enforce customs laws; and where DHS officers inspect
persons seeking to enter or depart, or applying for admission into, the United States
pursuant to U.S. immigration and travel controls. CBP collects passenger information in
order to fulfill its mission of securing the U.S. border while facilitating lawful travel and
trade. See 19 C.F.R. § 122.49a(b).

Page 7 GAO-22-105018 Contact Tracing for Air Travel
• International organizations, such as WHO and the International Civil
Aviation Organization (ICAO), issue international public health
regulations and guidance.
12
WHO implements and oversees these
regulations and—together with its partners, such as ICAO—helps
member states, like the United States, build response capacities.
ICAO plays a key role in coordinating the international aviation
response to public health risks. This coordination includes providing to
member states recommended protocols for contact tracing for various
diseases and standards for information relevant to public health
threats collected by border protection agencies. For example, in the
case of an infected passenger identified during a flight, ICAO’s
recommended practice is to collect specific elements of passenger
contact information using a standard paper form, known as the Public
Health Passenger Locator Form.
13
Countries may also rely on this
form when collecting contact information from passengers on a flight
arriving from locations with an identified communicable disease
outbreak.
After an individual infected with a communicable disease is identified as
having recently traveled by air into the country or between states, CDC is
notified—most often by a local public health authority—to help identify
other passengers on the flight who were potentially exposed
(“contacts”).
14
To facilitate the contact tracing investigation, CDC seeks to
collect contact and other relevant information about the exposed
passengers from multiple sources—particularly airlines and in some
instances CBP. Finally, CDC shares this information with the state or
local public health authority with jurisdiction for the locality in which the
exposed passenger is residing, whether permanently or temporarily (see
fig. 1).
12
The International Health Regulations were originally adopted by the World Health
Assembly, the governing body of WHO, in 1969 to address certain disease threats.
13
This form solicits specific elements of contact information and is to be distributed to
passengers who may have been exposed to an individual infected with a communicable
disease during flight in case they need to be contacted at a future date.
http://www.icao.int/safety/aviation-medicine/Pages/guidelines.aspx.
14
According to representatives from an organization representing state and local public
health authorities, CDC is generally not involved in providing contact information for
contact tracing investigations for passengers exposed to an infectious disease traveling
within one state (i.e., intrastate flight).
CDC’s General Process
for Collecting Air
Passenger Information

Page 8 GAO-22-105018 Contact Tracing for Air Travel
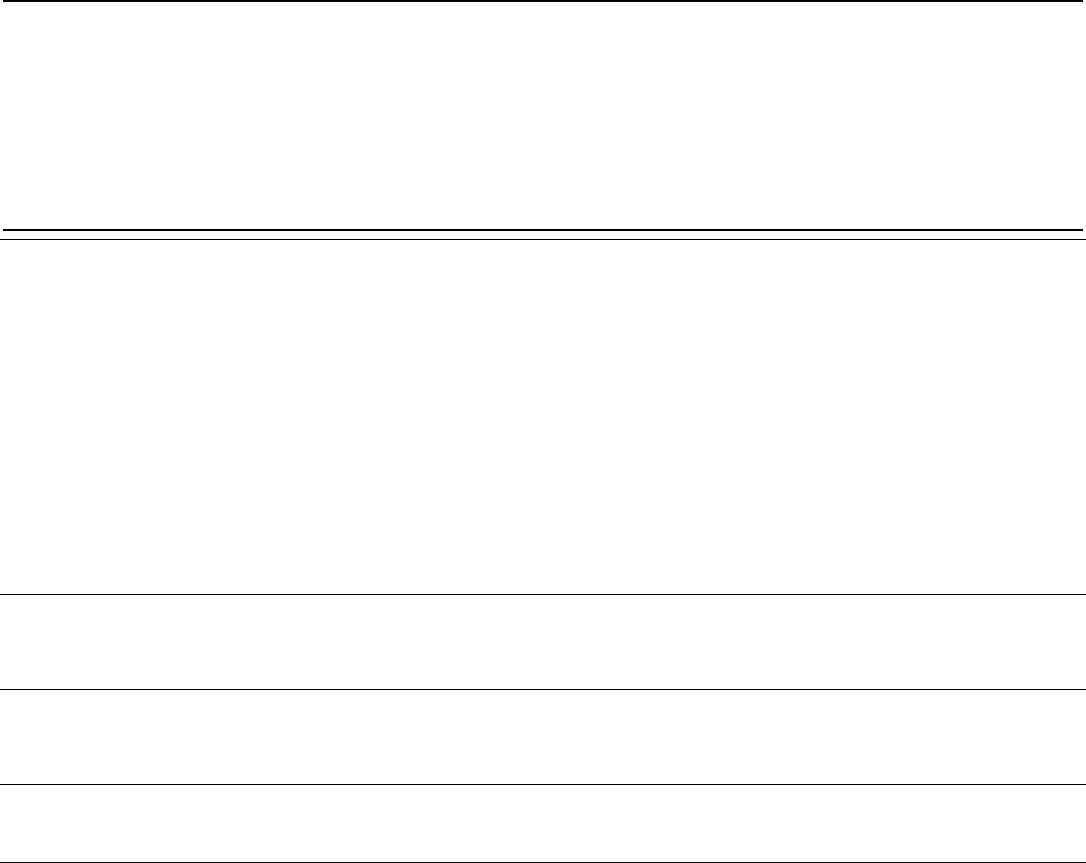
Figure 1: Overview of Process for Collecting Air Passengers’ Contact Information to Support Contact Tracing
To conduct effective contact tracing investigations for passengers
potentially exposed on a flight, CDC has identified five essential elements
of data for passenger contact information: name, U.S. address, email,
and primary and secondary phone number. CDC also seeks to collect
other information—such as seat number, initial and connecting flight
numbers, and final travel destination—that helps both identify passengers
who may have been exposed and facilitate the sharing of information with
appropriate state and local public health authorities.
CDC seeks to collect this information when it deems a contact
investigation for the infected passenger is warranted based on CDC-
established protocols, which are informed by international guidance.
15
CDC develops these protocols based on several factors, including the
proximity of that individual to the infected passenger on the aircraft. For
example, protocols for COVID-19, as well as for measles and
tuberculosis—the diseases most often identified in air travel prior to
COVID-19—specify that passengers in the same row and two rows in
front and behind (with some exceptions, such as for bulkheads) are in the
“contact-zone” and warrant a contact investigation. For twin-aisle aircraft,
this process may require contacting close to 50 passengers, as shown in
15
See, for example, World Health Organization, Tuberculosis and air travel: guidelines for
prevention and control, 3rd ed. (World Health Organization: 2008).

Page 9 GAO-22-105018 Contact Tracing for Air Travel
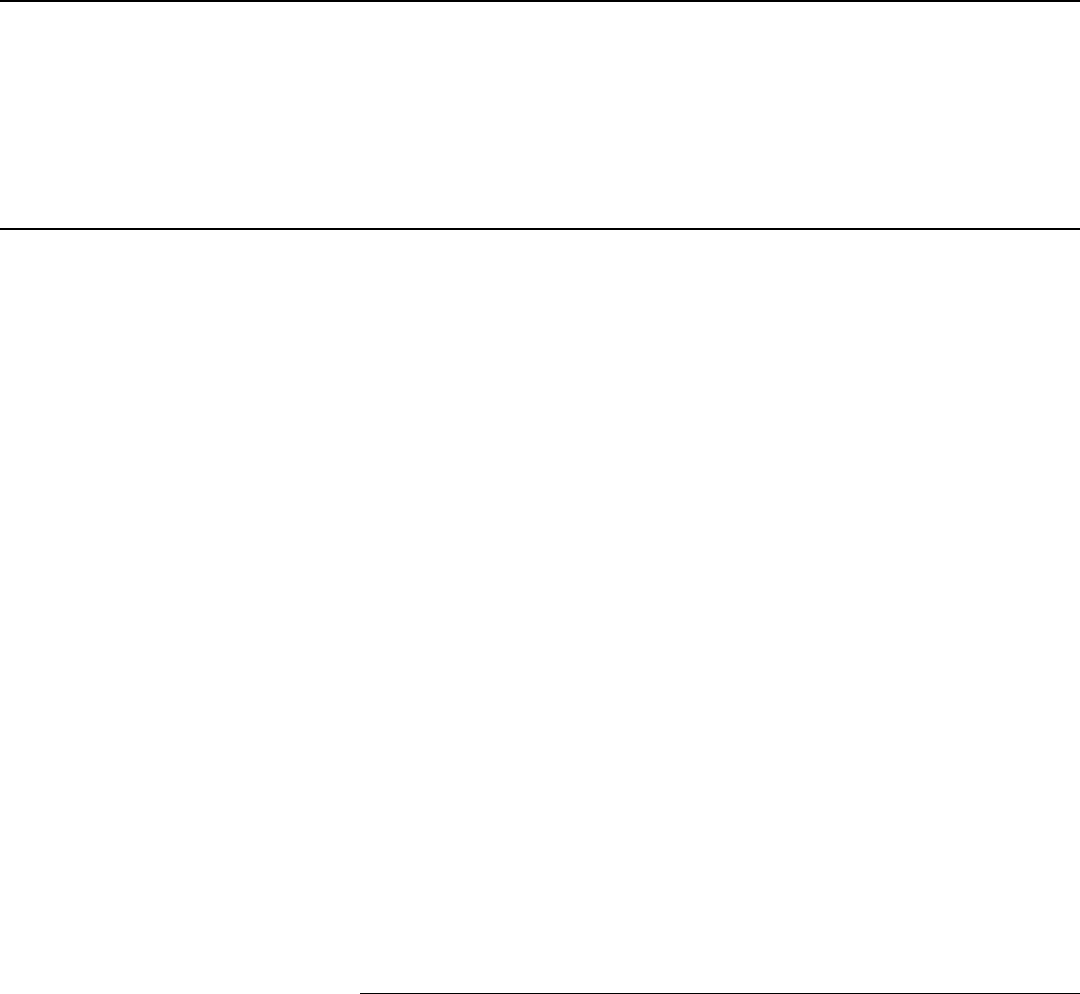
figure 2. Factors other than proximity include the disease characteristics
(e.g., method of transmission or incubation time) and other characteristics
of the specific case, such as the flight time (i.e., exposure duration) and
time between flight arrival and notification of CDC.
16
Figure 2: Examples of Air Passengers Seated in Proximity to an Infected Passenger,
Potentially Warranting a Contact Investigation, according to CDC Protocols
To obtain contact information for these passengers, CDC requires that
airlines provide passenger information that is available and already
maintained by the airline, such as information in its reservation system or
frequent flyer datasets. In doing so, CDC traditionally issues a flight
manifest request (i.e., manifest order) to airlines.
17
An airline manifest
would include additional information necessary to identify potentially
exposed passengers, such as seat assignments.
For passengers traveling on inbound international flights, CDC seeks to
supplement the information provided by airlines with passenger
information that CBP has already collected to enforce customs,
16
Thresholds for exposure duration and time to notification are disease dependent. For
example, according to CDC protocols for tuberculosis, a contact investigation is warranted
if the flight is 8 hours or longer gate-to-gate, the travel occurred within 3 months of
diagnosis, and CDC was notified within 3 months of travel, among other factors.
17
A flight manifest is a document maintained by airlines that includes a list of passengers
of an aircraft compiled before departure based on flight check-in information.

Page 10 GAO-22-105018 Contact Tracing for Air Travel
immigration, and agriculture laws at the border and ports of entry.
Specifically, CDC submits a request to CBP seeking additional
information for exposed passengers. In response to CDC’s request, CBP
uses its Automated Targeting System (ATS)—which is a decision support
tool that aggregates data from various data systems—to search and
extract contact information that is relevant to responding to public health
threats—such as a passenger’s address or passport number.
18
CBP has
traditionally provided these data to CDC in a standard Excel file format
through a secure federal data network. Some of the data that CBP
maintains is collected from airlines through the agency’s existing data
transmission feeds prior to departure, while some data are from other
CBP and non-CBP datasets and systems.
19
Throughout this process, CDC officials record the five essential elements
of contact information for the infected passenger and potentially exposed
passengers, as well as other information about each case (e.g., flight
number, date, arrival location, passport number), as they are received
into its Quarantine Activity Reporting System (QARS). According to CDC,
QARS is a web-based and secure electronic data system first developed
as a legacy case-management system in the mid-2000s that supports
collection of data for ill persons on inbound international or interstate
flights. CDC has described QARS as a system that enables the
quantification and analysis of the information collected to support disease
surveillance. For contact tracing, CDC officials use QARS to integrate the
passenger contact information and case records, and then to transmit
18
Specifically, ATS aggregates data from various systems and datasets—including the
Advance Passenger Information System and Passenger Name Record data provided by
airlines—to compare traveler, cargo, and conveyance information against law
enforcement, intelligence, and other enforcement data using risk-based scenarios and
assessments.
19
CBP uses an electronic data interchange system known as the Advance Passenger
Information System to collect passenger and crew manifest data for individuals traveling to
or from the United States by commercial or private aircraft, among other modes, as part of
the agency’s vetting process at ports of entry, which include some airports. In addition,
commercial airlines are required to provide CBP electronic access to certain passenger
reservation and/or departure information (if the airline maintains this information)
regarding passengers traveling on international flights to or from the United States. These
are called Passenger Name Record data. CBP also uses additional datasets as part of its
pre-travel information screening, such as the Global Enrollment System.

Page 11 GAO-22-105018 Contact Tracing for Air Travel
relevant information to public health authorities through a web-based
platform.
20
Several factors affect CDC’s efforts to collect the timely, accurate, and
complete air passenger information it needs to facilitate contact tracing.
21
Key factors include limitations in airlines’ ability to collect accurate and
complete information from passengers and the time it takes airlines to
respond to CDC’s requests for information. In addition, because there is
no single, complete, and reliable source of air passenger information
available, CDC must, in many cases, spend time conducting its own
research to fill in gaps.
Limitations in airline information. According to CDC, the agency relies
on airlines to identify specific passengers inside the contact zone of the
aircraft and provide any available contact information they have for those
passengers. However, CDC officials, airline representatives, and airline
association representatives we spoke with told us that airlines are
frequently unable to provide accurate and complete passenger
information.
22
For example, CDC reported that in a 2015 sample of
international manifest reports, 100 percent were missing at least one of
the five essential data elements—name, U.S. address, email, and primary
20
CDC transmits this information through its Epidemic Information Exchange system,
which according to CDC, is a secure, web-based platform that allows for instant transfer of
public health data, including information regarding contact investigations, from CDC to
jurisdictions across the United States.
21
CDC officials and representatives from local public health associations discussed other
challenges related to contact tracing for air travel that are outside of the scope of this
report. These challenges included the capacity of state and local health authorities to
notify CDC of infectious passengers based on their case investigations and to act on
notifications from CDC of air passenger contacts.
22
In response to a requirement in 42 C.F.R. § 71.4(c) to evaluate the burden of its 2017
Final Rule, CDC reported in 2019 that airlines only provided complete information for
about 16 percent of CDC’s requests for passengers traveling on inbound international
flights (an increase from almost zero percent). These results were based on examination
of 48 randomly selected airline manifests provided in response to CDC requests between
June 17, 2017, and January 12, 2018. See CDC, CDC Report as Required by the 2017
Control of Communicable Diseases Final Rule (Atlanta, Ga.: Feb. 6, 2019).
Multiple Factors
Impede CDC’s
Collection of Timely,
Accurate, and
Complete Passenger
Information

Page 12 GAO-22-105018 Contact Tracing for Air Travel
and secondary phone number.
23
According to these stakeholders, there
could be several reasons for this limitation.
First, according to one airline representative, airlines may not have
complete information because passengers are not required to provide
airlines all five of the essential data elements of contact information that
CDC seeks, such as an email address, to book a ticket or check in to a
flight. And in the case of airlines operating under a marketing code-share
agreement, passenger contact information may be collected by the
marketing airline and not available to the operating airline to provide to
CDC, according to representatives from an airline association.
24
Second, passengers may choose not to provide the airline with accurate
or complete contact information, according to representatives from three
airline associations and from two of the six airlines we interviewed. These
airline representatives highlighted that airlines lack a means to confirm
the accuracy of passenger-reported information.
Finally, passenger contact information may be incomplete as a result of
how the airline ticket was purchased. Representatives from all six of the
selected airlines we interviewed told us that for tickets purchased through
third parties, such as an online travel agency, the phone number and
email address provided to the airline for booking purposes may be for the
travel agency, not the passenger. Depending on the airline, more than
half of an airline’s tickets may be booked through third parties.
Representatives from a travel industry association and from an
organization that provides the technologies to distribute booking
information to and from airlines explained that travel agencies often
23
This explanation was stated in CDC’s Federal Register publication of its 2017 rule
requiring airlines to respond to a CDC manifest order within 24 hours by making available
to CDC elements of passenger information for passengers potentially exposed on
international inbound flights to the extent that they were readily available and already
maintained by the airline. Control of Communicable Diseases, 82 Fed. Reg. 6890, 6931
(Jan. 19, 2017).
24
Marketing airlines are those airlines that market flights to consumers, whether the airline
operates those flights or those flights are operated by a codeshare partner airline.

Page 13 GAO-22-105018 Contact Tracing for Air Travel
provide their own contact information as a way to support customers (i.e.,
passengers) in managing reservation changes and cancellations.
25
Time for airlines to provide information. CDC has reported that prior to
COVID-19, it often took airlines longer than the requested timeframe of 24
hours to provide passenger information and that in some cases, airlines
took up to 3 days to respond.
26
Representatives from all six airlines we
interviewed told us they consistently provide CDC with passenger
information within the requested timeframe of 24 hours.
27
However,
representatives from two of the six airlines we spoke with said that delays
may occur when they do not receive complete or accurate information
about the infected traveler from CDC, such as an incorrect flight number,
travel date, or misspelled name—information airlines need to retrieve the
appropriate manifest and identify passengers seated in the contact zone.
For example, a representative from one airline said that CDC may only
provide a name and date of travel, with no flight number, and that it can
take the airline several days to retrieve the manifest with such limited
information. On the other hand, this representative said the airline could
provide the requested information in 2 to 3 hours when CDC provides the
flight number in addition to the passenger’s name and date of travel.
CDC officials told us that information on infected passengers comes
directly from local public health authorities, and that CDC is limited by
what those authorities are able to provide. Public health authorities collect
any available information from the infectious passenger seeking treatment
in their jurisdiction, but the passenger might not provide complete or
accurate information or be able to recall the travel details.
Need to seek supplemental information. Due to gaps or obvious errors
in data provided by airlines, CDC often must seek supplemental
information from additional sources, such as from CBP or research
databases, adding further time to the contact tracing process. CDC
officials estimate that after the agency has been notified of an infected
passenger, it can take up to 2 weeks to collect information on potentially
25
These technologies—known as global distribution systems—are computer systems that
display airline flight schedule and fare information so that travel agents can query it to
“book” (i.e., reserve and purchase) flights for consumers.
26
CDC, CDC Report as Required by the 2017 Control of Communicable Diseases Final
Rule (Atlanta, Ga.: Feb. 6, 2019).
27
We interviewed representatives of six U.S. commercial passenger airlines. CDC officials
told us that foreign airlines may take longer to respond to CDC’s requests for passenger
information.

Page 14 GAO-22-105018 Contact Tracing for Air Travel
exposed passengers and share this information with local public health
authorities. This delay can contribute to broader community spread of a
disease, as potentially exposed passengers may become difficult to
locate and notify, or they may become symptomatic or infectious during
this time.
For passengers traveling on inbound international flights, CDC is able to
supplement airline-provided information with data provided by CBP. CDC
officials told us that CBP may have more accurate passenger
information—such as an up-to-date physical address where the
passenger resides or is staying in the United States—because CBP
checks the information against a passenger’s passport, and the
passengers risk penalties if they provide false information.
28
However,
CBP only collects data for passengers on flights arriving into the United
States.
29
These passengers constituted about 25 percent of the travelers
(or about 120 million travelers) flying into and within the United States on
scheduled flights in 2019, and about 13 percent since the onset of the
COVID-19 pandemic.
For cases in which the information collected from airlines and CBP is
outdated or incomplete, and for all cases in which the passengers were
traveling on domestic interstate flights, CDC conducts manual searches
for contact information in other databases, such as LexisNexis—further
extending the length of this process.
Even after conducting supplemental research, CDC may not have
complete or accurate passenger contact information. Representatives
from two organizations representing public health authorities told us that it
is not uncommon for CDC to provide them with incomplete contact
information, such as a partial name. In such cases, public health staff
must invest significant resources to identify and locate the correct
individual, according to these representatives.
28
For example, individuals may be fined or imprisoned for willfully and knowingly using, or
attempting to use, a passport that was secured by false statements. 18 U.S.C. § 1542.
29
CBP also collects data on passengers departing the United States. See, e.g., 19 C.F.R.
§ 122.75a.

Page 15 GAO-22-105018 Contact Tracing for Air Travel
Since the COVID-19 global pandemic began in March 2020, CDC has
taken some actions to improve the timeliness, accuracy, and
completeness of the information it collects from various sources for
passengers arriving on flights into the United States. These actions
included expanding coordination with CBP and establishing new
requirements for inbound international flights.
In response to the COVID-19 pandemic and following a series of
Presidential proclamations, CBP, in coordination with CDC, has taken
steps to provide more timely and complete information to CDC for
passengers on inbound international flights believed to have been
exposed to a communicable disease.
30
Specifically, since the pandemic
began, CBP has (1) automated the process by which it searches for and
provides passenger information to CDC in certain scenarios and (2)
expanded the federal agency datasets through which CBP searches for
information.
31
First, CBP built automated rules within its Automated Targeting System
such that, without waiting for CDC requests for individual passengers,
CBP officials can identify travelers who are subject to travel restrictions
due to an outbreak in their departure country, but who are permitted to
travel to the United States under an approved exemption. For example,
following the identification of the Omicron variant in South Africa, a
Presidential proclamation on November 26, 2021, invoked section 212(f)
of the Immigration and Nationality Act to restrict travel of noncitizens with
30
On January 31, 2020, the White House issued the “Proclamation on Suspension of
Entry as Immigrants and Nonimmigrants of Persons who Pose a Risk of Transmitting
2019 Novel Coronavirus,” the first of several proclamations issued regarding COVID-19
related travel restrictions. Proclamation No. 9984, 85 Fed. Reg. 6709 (Jan. 31, 2020).
31
CBP also reported that during the pandemic, Department of State agreed to begin
sharing visa application data with CBP and subsequently CDC.
CDC Has Made
Some Improvements
to the Quality of Air
Passenger
Information It Collects
for Inbound
International Travel
CDC and CBP Have
Expanded Coordination for
International Travel

Page 16 GAO-22-105018 Contact Tracing for Air Travel
recent presence in any of the eight listed African countries.
32
CBP could
then extract relevant passenger data from ATS, aggregate them into
person-centric records for each traveler, and transmit the record to CDC
within 8 hours of the flight’s arrival through a secure data file transfer.
In February 2021, CBP expanded the agreement with CDC to allow CBP
to share information for passengers traveling on inbound international
flights beyond those who recently traveled from 212(f)-restricted
countries.
33
In some cases, however, CDC continues to rely on the labor-
intensive, semi-automated process of submitting a request to CBP for
specific passengers identified through airline manifests. CDC officials also
told us that as of December 2021, no decision had been made as to
whether CBP’s automated process of search and transmission would
continue beyond the pandemic.
Second, CBP expanded the number of federal datasets it searches for
relevant information to share with CDC. For example, U.S. Citizenship
and Immigration Services (USCIS), a component of DHS, collects and
maintains information from noncitizens applying for immigration benefits,
including their contact information. To support CDC’s public health follow-
up efforts, CBP has shared with CDC biographic information on approved
and pending lawful permanent residents collected by USCIS since
September 2020.
Since the onset of the COVID-19 pandemic, CDC has taken several
regulatory actions that increased the requirements for airlines to collect,
maintain, and transmit to CDC specific elements of passenger
information. Prior to the pandemic, CDC regulations for contact tracing
generally did not require airlines to collect any specific data elements
from passengers to support contact tracing or to provide them in any
32
Section 212(f) of the Immigration and Nationality Act (INA) gives the President of the
United States the authority to issue Presidential proclamations to suspend entry of any
noncitizen for a period of time deemed necessary by the President whenever the
President finds that entry of such individuals would be detrimental to the interests of the
United States. 8 U.S.C. § 1182(f). The restrictions on these eight countries have been
rescinded, effective December 31, 2021.
33
CBP has published Privacy Impact Assessments on this data exchange. See
Department of Homeland Security, DHS/CBP/PIA-066 CBP Support of CDC for Public
Health Contact Tracing (Washington, D.C.), accessed March 14, 2022,
https://www.dhs.gov/publication/dhscbppia-066-cbp-support-cdc-public-health-contact-
tracing.
Selected Foreign Countries’ Actions
Some of CDC’s actions have similarities with
strategies for air travel that other countries
have recently undertaken in response to
COVID-19. Public health and border
protection officials we spoke with from
Australia, Canada, and the United Kingdom
told us that their countries also increased
automation in collecting and managing
passenger information. Some countries are
also working to improve coordination with their
respective border protection agencies to
leverage more information. To help inform the
public, one country publishes on a website
flights that had passengers infected with
COVID-19 onboard.
Source: GAO summary of interviews with public health and
border protection officials from selected foreign countries. |
GAO-22-105018
CDC Has Established
New Requirements for
Inbound International
Flights

Page 17 GAO-22-105018 Contact Tracing for Air Travel
particular format.
34
While airline representatives we interviewed
expressed reservations about the new requirements, they told us that
they are ultimately willing and able to comply with them.
In early 2020, following the first reported cases of COVID-19 in China,
CDC held discussions with the airline industry and other federal agencies,
including CBP and FAA, to identify actions to improve the quality of
information CDC could collect from airlines. In February 2020, CDC
issued an Interim Final Rule requiring airlines to, in response to a CDC
order, collect and provide CDC with five designated pieces of information
for passengers traveling on inbound international flights.
35
Under this
interim rule, CDC issues implementing orders to airlines to trigger the
requirements.
36
In October 2021, CDC issued its most recent order—a global contact
tracing order, which requires airlines to collect, maintain, and, after
receiving a CDC request, transmit to CDC specific elements of passenger
information within a specific timeframe.
37
CDC reports that these
requirements are intended to provide timelier, accurate, and complete
passenger information to CDC for passengers traveling on flights arriving
into the United States. Airlines are to:
• Collect the five designated elements of contact information—to the
extent that they exist—from all passengers traveling on inbound
international flights no more than 72 hours before departure. CDC
34
Specifically, CDC’s regulations required airlines only to respond to a CDC manifest
order within 24 hours by making available to CDC passenger data to the extent that they
were already available and maintained by the airline. Control of Communicable Diseases,
82 Fed. Reg. 6890, 6975 (Jan. 19, 2017) (codified at 42 C.F.R. § 71.4).
35
These five designated elements of passenger contact information comprise the
international traveler’s full name, address while in the United States (or permanent
residence if a U.S. citizen or lawful permanent resident), primary phone number,
secondary phone number, and email address. Control of Communicable Diseases;
Foreign Quarantine, 85 Fed. Reg. 7874, 7880 (Feb. 12, 2020) (codified at 42 C.F.R. §
71.4(d)–(e)).
36
For example, CDC issued an order in February 2020 requiring airlines to collect and
provide data for passengers who were in the People’s Republic of China within 14 days of
entry into the United States. Collection of Certain Data Regarding Passengers and Crew,
85 Fed. Reg. 10439 (Feb. 24, 2020).
37
This order went into effect November 8, 2021. See Requirement for Airlines to Collect
and Transmit Designated Information for Passengers, 86 Fed. Reg. 61246, 61246 (Nov. 5,
2021).

Page 18 GAO-22-105018 Contact Tracing for Air Travel
explains in the order that the best way to ensure passengers’ contact
information is available in real time is to collect the information before
they board a flight.
• Transmit the contact information to CDC in a defined format, using
one of the specified data transfer mechanisms.
38
By requiring airlines
to provide CDC data in a specified format, the information can be
entered into its QARS data management system more quickly,
ultimately improving the overall timeliness of the data.
Stakeholders had mixed views on CDC’s recent rule and orders.
Representatives from a major airline association told us that while they
believe the rule and orders have placed an outsized burden on the
industry, airlines are ultimately willing and able to comply with the
requirements.
39
Several aviation stakeholders, including representatives
from four airline associations and three airlines, highlighted that FAA’s
leadership and knowledge were particularly helpful in “translating” the
nuances of airlines’ processes and systems for CDC officials.
On the other hand, representatives from a major airline association and
one airline told us that despite repeated requests, CDC has not
communicated with them where the gaps exist in the passenger
information it collects, or the extent to which these requirements would
improve the accuracy or completeness of information. As discussed
above, one such example of a gap is that passenger contact information
may still be inaccurate for passengers who have purchased tickets
through third parties, such as an online travel agency.
Nevertheless, according to CDC officials, their recent regulatory actions
have resulted in the agency being able to more quickly collect more
complete and up-to-date information for passengers traveling on inbound
international flights. CDC officials said that, as of March 2022, they were
38
Depending on the transmission mechanism used, airlines may in some cases also be
required to maintain the passenger data for up to 30 days and provide the data within 24
hours of a CDC request (i.e., CDC manifest order).
39
To comply with the global contact tracing order, representatives from three airline
associations and four airlines told us airlines will need to make—and some airlines already
have made—significant modifications to their IT systems potentially costing millions of
dollars in order to collect and maintain the required data elements for transmission to CDC
in the required format.
Selected Foreign Countries’ Processes for
Collecting Information
During the pandemic, in contrast to the United
States, some foreign governments expanded
and automated a process by which they
collect information directly from passengers
arriving on international flights rather than
through the airlines. For example, Australia,
Canada, and the United Kingdom each
developed an online form, web portal, or
mobile application to collect information from
passengers before departure. Officials from
these countries told us that the information
they collected also supported enforcement of
national quarantine and vaccination policies.
These officials said their efforts improved data
quality, but that collecting accurate
information directly from passengers did pose
challenges. Officials from one of the countries
noted that no country has a “golden ticket”
solution for contact tracing following air travel.
Source: GAO summary of interviews with public health and
border protection officials from selected foreign countries. |
GAO-22-105018

Page 19 GAO-22-105018 Contact Tracing for Air Travel
undertaking an assessment of these improvements, but that the results of
the assessment were not yet complete.
However, as currently issued, the new requirements are temporary. CDC
officials and airline representatives told us in March 2022 that they
assumed these requirements would be permanent, yet it is uncertain
when, or if, a permanent rule will be issued.
40
The Interim Final Rule
states that CDC promulgated the rule in response to the COVID-19 public
health emergency and that the rule will cease to be in effect either when
the pandemic is over or when the Secretary of HHS determines there is
no longer a need.
41
While CDC has taken some steps to improve the quality of information it
collects for passengers on inbound international flights, other limitations in
how CDC collects and manages air passenger information have not been
addressed and hinder the agency’s efforts to facilitate contact tracing.
Specifically, CDC lacks sufficient controls to reduce the risk of errors and
inconsistencies resulting from manual entry of passenger information. In
addition, CDC has not fully assessed potential opportunities to improve
data quality. Moreover, the outdated design of the QARS data
40
The Department of Homeland Security published in the Fall 2021 Unified Agenda that it
is working on a proposed rule that would require air carriers to transmit additional data
elements through the Advance Passenger Information System (APIS) for all commercial
airline passengers arriving in the United States in order to support border operations and
national security. According to the Unified Agenda publication, this collection of additional
data elements will also support the efforts of CDC’s contact tracing for air travel. 87 Fed.
Reg. 5002, 5086 (Jan. 31, 2022). Airline representatives told us they expect this new rule
will include a requirement for all international airlines to provide the five designated
elements of contact information that CDC is currently requiring under the global contact
tracing order.
41
The Interim Final Rule states: “Unless extended after consideration of submitted
comments, this interim final rule will cease to be in effect on the earlier of (1) the date that
is two incubation periods after the last known case of 2019–nCoV, or (2) when the
Secretary determines there is no longer a need for this interim final rule.” 85 Fed. Reg.
7874, 7874 (Feb. 12, 2020).
Unaddressed
Limitations in How
CDC Collects and
Manages Air
Passengers’
Information Hinder
Contact Tracing

Page 20 GAO-22-105018 Contact Tracing for Air Travel
management system does not meet CDC’s needs for disease
surveillance in air travel.
42
CDC’s process for entering air passenger information into its QARS data
management system has the potential for errors and inconsistencies, due
to the need to manually enter information collected in varying formats
from multiple sources. Data entry by numerous staff and contractors
across the country, including for the same case investigation record,
further heightens this risk. However, CDC lacks sufficient controls on data
entry, such as adequate training and procedures for system users and
consistent validation checks, to help ensure data quality and reliability.
As shown in figure 3, CDC collects and receives information from multiple
sources. This information is received in a variety of formats. For example,
representatives from all six airlines we interviewed told us they generally
transmit data to CDC in encrypted email attachments in a range of
formats, such as Microsoft Word, Excel, or Adobe Acrobat. Some airlines
provide information on Telex printouts that often have illegible portions,
according to one CDC official we interviewed.
43
CDC staff and contractors
must translate and enter these data—often manually—into spreadsheets,
which are then uploaded into CDC’s QARS data management system.
42
In the past, we have also reported on issues related to CDC’s data security. For
example, in June 2018, we identified control and program deficiencies in the core security
functions related to safeguarding the confidentiality, integrity, and availability of CDC’s
information systems and information. That report was designated as “limited official use
only” (LOUO) and not publicly released because of the sensitive information it contained.
We published a subsequent report in December 2018 that discussed the findings in our
June 2018 report, but with references to the sensitive information removed. CDC has
taken actions to address all 195 recommendations contained in those reports. See GAO,
Information Security: CDC Needs to Improve Its Program and Resolve Control
Deficiencies, GAO-18-437SU (Washington, D.C.: June 20, 2018) and GAO, Information
Security: Significant Progress Made, but CDC Needs to Take Further Action to Resolve
Control Deficiencies and Improve Its Program, GAO-19-70 (Washington, D.C.: Dec. 20,
2018).
43
Telex is an international system of sending written messages. Messages are converted
into signals, which are transmitted over a network and then printed out by a machine in
another place.
CDC Lacks Sufficient
Controls to Reduce the
Risk of Errors and
Inconsistencies Resulting
from Manual Data Entry

Page 21 GAO-22-105018 Contact Tracing for Air Travel
Figure 3: Illustration of CDC’s Reliance on Manual Entry to Process Air Passenger Contact Information into Its Quarantine
Activity Reporting System
In addition, while CBP has recently automated portions of the process for
contact investigations pertaining to passengers traveling on international
inbound flights, CDC’s process for entering the passenger information
from CBP may include numerous non-automated steps between
requesting and receiving the data. For example, according to CDC
officials, if airlines are unable to provide a partial airplane manifest of the
contact zone to CDC, then officials located at CBP’s National Targeting
Center must query CBP data systems for all passenger records and seat
numbers to determine which travelers were within the contact zone.
44
This process entails a CDC or CBP official manually populating the
configuration of an entire flight into a spreadsheet in order to determine
where an infectious passenger sat in relation to other passengers. Finally,
regardless of the source, CDC may need to fill gaps in passenger contact
information by conducting its own research using additional databases,
such as LexisNexis, and manually entering these data into QARS.
Numerous CDC staff and contractors across the agency’s locations and
divisions—including headquarters and the 20 regional quarantine
44
CBP’s National Targeting Center leads all of CBP’s pre-departure targeting and vetting
efforts. The National Targeting Center is a 24/7 operations entity responsible for providing
advance information and research about high-risk travelers and cargo and facilitating
coordination between law enforcement and intelligence agencies in support of CBP’s anti-
terrorism mission and efforts to keep high-risk individuals and cargo from boarding U.S.-
bound flights.

Page 22 GAO-22-105018 Contact Tracing for Air Travel
stations—enter information from these sources into QARS, sometimes
even for one passenger’s case record. For example, when local public
health authorities notify a quarantine station in their jurisdiction of a
person who may have traveled while infectious, staff at that location open
a case investigation by manually entering into QARS the information
provided. Then, as part of the process of collecting supplemental
passenger information, additional staff may access and edit the case
records, including staff in headquarters and in regional Quarantine
Stations.
The process of numerous individuals translating data from various
formats and manually entering them into the QARS data management
system presents risk of errors. For example, CDC officials reported
instances in which staff mislabeled passenger information, such as by
erroneously entering the flight’s arrival date as predating its departure or
creating duplicate entries when entering the results of a passenger’s
laboratory test. Moreover, providing access for multiple staff to enter
information into one case record may be helpful, but it can lead to
inconsistencies in the way information is documented. For example,
information used to identify whether a case investigation is warranted is
inconsistent among case records because staff may enter this information
using personal judgement, according to CDC officials.
CDC’s reliance on additional contracted staff to enter information into
QARS for the increased number of contact investigations during the
pandemic could introduce further risk of inconsistencies. CDC estimates
that for each year from 2015 through 2019, about 80 to 130 distinct flights
warranted at least one contact investigation, compared to more than an
estimated 25,000 distinct flights in 2020.
45
Officials at one regional
quarantine station told us that since the outset of the pandemic, the
number of staff has increased from four full-time employees to more than
30 additional contractors.
Federal standards for internal controls highlight the importance of
adopting and implementing controls for data entry and information
processing to maximize data quality.
46
A control activity may include
45
Because one infected passenger may travel on multiple flights, the number of distinct
flights warranting at least one contact investigation may be greater than the number of
notifications received by CDC warranting contact investigations.
46
GAO, Standards for Internal Control in the Federal Government, GAO-14-704G
(Washington, D.C.: Sept. 10, 2014).

Page 23 GAO-22-105018 Contact Tracing for Air Travel
providing adequate training to users, developing standard operating
procedures for data entry, or conducting consistent validation checks of
data entered.
CDC has taken some steps to improve data quality since the pandemic
began. CDC officials who work with QARS told us they have provided
some training to staff to reduce errors and increase consistency in data
entry. For example, recognizing the need for additional training to account
for the expanded number of contractors using QARS, a data analyst from
CDC headquarters visited one of CDC’s 20 regional quarantine stations
to personally oversee staff training and provide training materials, such as
“practice homework.” However, because the training is not
institutionalized across CDC offices, its effectiveness is limited and
continuation uncertain. In addition, CDC was unable to provide us
documentation of a detailed user manual or other documented standard
operating procedures for QARS users.
CDC officials who work with QARS told us they recently began to conduct
informal, manual retrospective reviews of QARS data to track frequent
data entry errors and find ways to improve data reliability. In response to
these reviews and other work, the officials have implemented some
automated system logic checks, such as to restrict a QARS user from
incorrectly entering a flight arrival date that precedes the flight’s
departure. However, CDC prioritizes logic checks for the “highest impact”
variables due to limited resources, and additional checks are needed,
according to the officials.
Without sufficient data entry controls, such as adequate training that is
institutionalized across the agency, standard operating procedures, and
comprehensive logic checks, to help increase data reliability, CDC is
limited in its ability to facilitate contact tracing and effectively monitor the
public health risk associated with air travel more broadly. For example,
due to irregularities in data quality, CDC officials were unable to provide
us with sufficiently reliable information—such as the number of manifest
requests CDC has submitted to airlines, or the total number of
passengers who were exposed and warranted a contact investigation—
for each year from 2015 through 2020. Rather, CDC provided estimations
of this information with explanations of the limitations of its reliability.
Using unreliable data, CDC may be overestimating or underestimating the
number of cases it conducts annually in total or at one of its quarantine
stations, hindering the agency’s ability to make informed decisions about
workload or staff resource allocations among its 20 regional quarantine

Page 24 GAO-22-105018 Contact Tracing for Air Travel
stations. CDC officials said that in some instances, data analysts have
discovered data entry errors much later—sometimes years later—when
they were attempting to analyze the data for secondary purposes. This
raises questions about additional undiscovered errors in the air
passenger information CDC shares with its public health partners.
Data entry controls can help to reduce errors and inconsistencies when
manual data entry is required. However, CDC has not fully assessed
other potential opportunities to improve data quality. CDC officials told us
that in their efforts to respond to the COVID-19 pandemic, they have
identified some steps that may improve how CDC collects and manages
passenger information—such as standardizing how local public health
authorities share this information with CDC—but they have not assessed
feasibility or fully explored whether other potential opportunities exist.
47
Specifically, CDC officials told us that CDC and state and local health
authorities use established data exchange standards when sharing
information for other activities, including disease surveillance, but those
standards are not currently compatible for air passenger information.
48
For example, those data exchange standards do not apply to personal
identifiable information, which passenger contact information contains.
CDC officials said that if public health authorities and CDC were able to
adopt data exchange standards for air passenger information, such
standards could increase automated data sharing between CDC and local
public health authorities and reduce the need for some manual entry.
In addition, CDC officials told us they frequently do not receive
information on the outcomes of case investigations performed by local
47
We recently issued a report that discussed CDC efforts related to other public health
data systems. CDC has made progress in modernizing the U.S. public health collection
and surveillance infrastructure through its Data Modernization Initiative. However, CDC’s
Data Modernization Initiative’s strategic implementation plan does not articulate the
specific actions, time frames, and allocation of roles and responsibilities needed to
achieve its objectives. We recommended that CDC define specific action steps and time
frames for the agency’s data modernization efforts, and HHS agreed with this
recommendation. See GAO-22-105397.
48
Data standards can be defined generally as technical specifications that describe how
data should be stored or exchanged for the consistent collection and interoperability of
that data across different systems, sources, and users. CDC reports that CDC and local
public health authorities use National Notifiable Diseases Surveillance System (NNDSS)
architectural standards as a basis for integrated surveillance information systems in public
health departments. These architectural standards help public health agencies accept
electronic data exchanges from healthcare systems and enables health departments to
create and send standards-based case notifications to CDC for NNDSS.
CDC Has Not Fully
Assessed Potential
Opportunities to Improve
Data Quality

Page 25 GAO-22-105018 Contact Tracing for Air Travel
public health authorities. Representatives from organizations representing
public health officials told us that some state health departments have
reported that it is unclear whether CDC has a standardized process for
soliciting feedback on contact tracing investigation outcomes from state
and local public health authorities. CDC officials said data exchange
standards that increase bi-directional exchange of data with local public
health authorities may increase the information CDC receives on
outcomes, allowing the agency to better assess the overall quality of
information it provides as part of the contact tracing process.
In addition, CDC has previously recognized that standardizing the format
in which it receives manifest information from airlines could improve data
quality but has not fully explored the feasibility of doing so for information
on passengers traveling on interstate flights. CDC officials told us that its
recent global contact tracing order requiring airlines to provide information
for passengers traveling on inbound international flights in a standardized
format has improved the timeliness and accuracy of the information. Yet
airlines still provide information for domestic interstate flights to CDC in
different formats, and it is unclear if the Interim Final Rule and global
contact tracing order will become permanent.
49
CDC officials told us they
focused on passengers traveling on inbound international flights—despite
being a small proportion of the total passengers flying into and between
states—because CDC’s Division of Global Migration and Quarantine,
which spearheads the collection of air passenger information, focuses on
activities that reduce the chance of diseases crossing international
borders.
While CDC officials told us the agency has recently begun to take steps
to evaluate its process for collecting and managing air passenger
information, these officials said that constrained resources and competing
priorities have limited CDC’s ability to advance these efforts. Evaluation
plays a key role in program planning, management, and oversight by
49
In 2005, CDC proposed requirements for airlines to collect and transmit passenger
information for international and interstate flights to CDC within a specified timeframe, but
ultimately the rule was not finalized. Control of Communicable Diseases, 70 Fed. Reg.
71892 (proposed Nov. 30, 2005).

Page 26 GAO-22-105018 Contact Tracing for Air Travel
providing feedback on both program design and execution.
50
Agencies
can use performance information to make various types of management
decisions to improve programs and results. In addition, federal standards
for internal control state that agencies should develop monitoring
activities, including periodic evaluations, to ensure programs are meeting
agency objectives.
51
CDC officials told us they are still discussing developing a plan to identify
gaps in its process and opportunities to address them, as well as to
assess the overall quality of the information it shares with local public
health partners. One of the areas that officials said they hope to explore is
the feasibility of adapting data exchange standards to decrease manual
entry of data into QARS. While such efforts appear promising, as of
March 2022, CDC was still discussing details of the plan and did not have
a timeline for completion.
Initially developed in the mid-2000s, CDC’s data management system for
air passenger information (QARS) limits CDC’s ability to effectively
facilitate contact tracing and conduct disease surveillance for air travel.
The QARS system has independent rather than linked case records,
lacks the functionality to efficiently analyze data, and has limited data
fields. This situation makes it difficult for CDC to assess and aggregate
data across individual cases, develop its own contact tracing protocols,
and evaluate its performance in collecting and sharing timely, accurate,
and complete passenger information.
More specifically, officials told us that CDC developed QARS from a
legacy record-keeping system that collected and managed information for
each passenger case independent of others. Because QARS was not
designed for rapid assessment or aggregation of public health data
across individual cases, it hinders CDC’s ability to report key information
as part of the contact tracing process. For example, CDC is unable to
quickly and accurately identify the number of passengers exposed to a
specific infected passenger, or their relationship to the infected passenger
(e.g., family member or travel companion). As a result, it is difficult to
50
GAO, Program Evaluation: Strategies to Facilitate Agencies’ Use of Evaluation in
Program Management and Policy Making, GAO-13-570 (Washington, D.C.: June 26,
2013); Performance Measurement and Evaluation: Definitions and Relationships,
GAO-11-646SP (Washington, D.C.: May 2011); and Managing For Results: Enhancing
Agency Use of Performance Information for Management Decision Making, GAO-05-927
(Washington, D.C.: Sept. 9, 2005).
51
GAO-14-704G.
CDC’s Data Management
System Is Outdated and
Does Not Meet CDC’s
Needs

Page 27 GAO-22-105018 Contact Tracing for Air Travel
share with public health authorities any connected cases within their
jurisdictions or trends regarding outbreaks in their area. According to
representatives from an organization representing local public health
authorities, when CDC shares information on potentially exposed
passengers who may have been exposed, CDC does not always indicate
that the case is connected to a traveler the local public health authority
previously notified CDC about. These representatives said this type of
information could help local public health authorities prioritize and conduct
their contact investigations.
The system’s outdated design, which does not allow CDC to efficiently
analyze data, also affects CDC’s ability to develop its own protocols for
supporting contact tracing. For example, to develop a reporting threshold
protocol for COVID-19—such as, the number of days passed since
exposure after which public health authorities no longer need to report an
infectious passenger to CDC—the agency had to engage in a process it
described as resource intensive to extract data from QARS and conduct
additional analyses outside of the system. CDC developed this threshold
to prioritize cases with the highest likelihood of spreading COVID-19, as
CDC would not initiate a contact investigation in QARS for cases reported
outside of this time period. During the time it took CDC to develop the
threshold, state and local public health authorities may have been using
their constrained resources to initiate contact investigations for cases that
CDC would no longer characterize as high priority.
The design of QARS system also impedes CDC’s ability to assess the
quality of air passenger information it receives from other sources.
Officials told us QARS does not contain the data fields necessary to allow
them to assess timeliness, accuracy, or completeness of information
collected from its sources. For example, according to officials, QARS
does not contain the information necessary to quickly and accurately
determine how long it takes an airline to fulfill a manifest request.
CDC officials also told us they are unable to use QARS to identify and
thus distinguish among the various sources of data elements, hindering
their ability to assess the quality of data received from airlines versus
other sources. Rather, CDC must often use time-consuming
supplemental processes—such as by using Excel spreadsheets,
visualization dashboards, or proxy variables to obtain information—to
assess the information it collects.
CDC has conducted a formal evaluation of the timeliness and
completeness of passenger contact information provided by airlines for

Page 28 GAO-22-105018 Contact Tracing for Air Travel
international flights one time, in 2019.
52
According to CDC officials,
because CDC could not identify information collected from airlines versus
other sources, staff had to extract data from QARS and create
spreadsheets outside of the system to evaluate data. This process took
several months to complete, as CDC had to review each individual case
file.
53
CDC has only minimally assessed the quality of information it
receives for passengers traveling on domestic interstate flights, in part
because QARS system limitations make such analyses time-consuming
and resource-intensive. However, officials estimate contact investigations
for domestic interstate flights constituted more than 90 percent of total
contact investigations in 2020.
The limitations in the design of the QARS system prevent CDC from
meeting the standards of its own strategic documents or federal
standards for internal control. Specifically, CDC’s strategic documents call
for the ability to swiftly disseminate contact data to local public health
authorities, identify gaps in current prevention and control efforts, and
update aging technology systems in order to store, access, and transport
timely, quality data.
54
Federal standards for internal control state that
agencies should design information systems that help achieve their
objectives and respond to risks.
55
CDC officials told us they have
identified many areas to improve QARS but have not fully defined the
system requirements that would better enable the agency to meet its
needs.
CDC officials said the limitations of the QARS system were somewhat
manageable before the COVID-19 pandemic, when CDC received about
100 notifications per year of an infected passenger warranting contact
tracing, compared with more than an estimated 17,000 in 2020. Even so,
prior to the pandemic, CDC had been assessing the limitations in the
design of QARS and was in the early stages of developing a
52
This evaluation was conducted as required by its 2017 rule. See 42 C.F.R. § 71.4(c).
53
The 2019 evaluation report stated that there was some evidence that timeliness
improved since the 2017 regulation went into effect; however, completeness of contact
data provided by airlines generally did not change.
54
See U.S. Centers for Disease Control and Prevention, A CDC Framework for Preventing
Infectious Diseases: Sustaining the Essentials and Innovating for the Future. (Atlanta, Ga.:
October 2011); National Center for Emerging and Zoonotic Infectious Diseases Strategic
Plan: 2018-2023 (Atlanta, Ga.: August 2018); and Information Technology Strategic Plan
(ITSP) FY 2021-FY 2023 (Atlanta, Ga), accessed Apr. 22, 2022,
https://www.cdc.gov/od/ocio/it-strategic-plan/2021-23/overview/goal1/index.html.
55
GAO-14-704G.
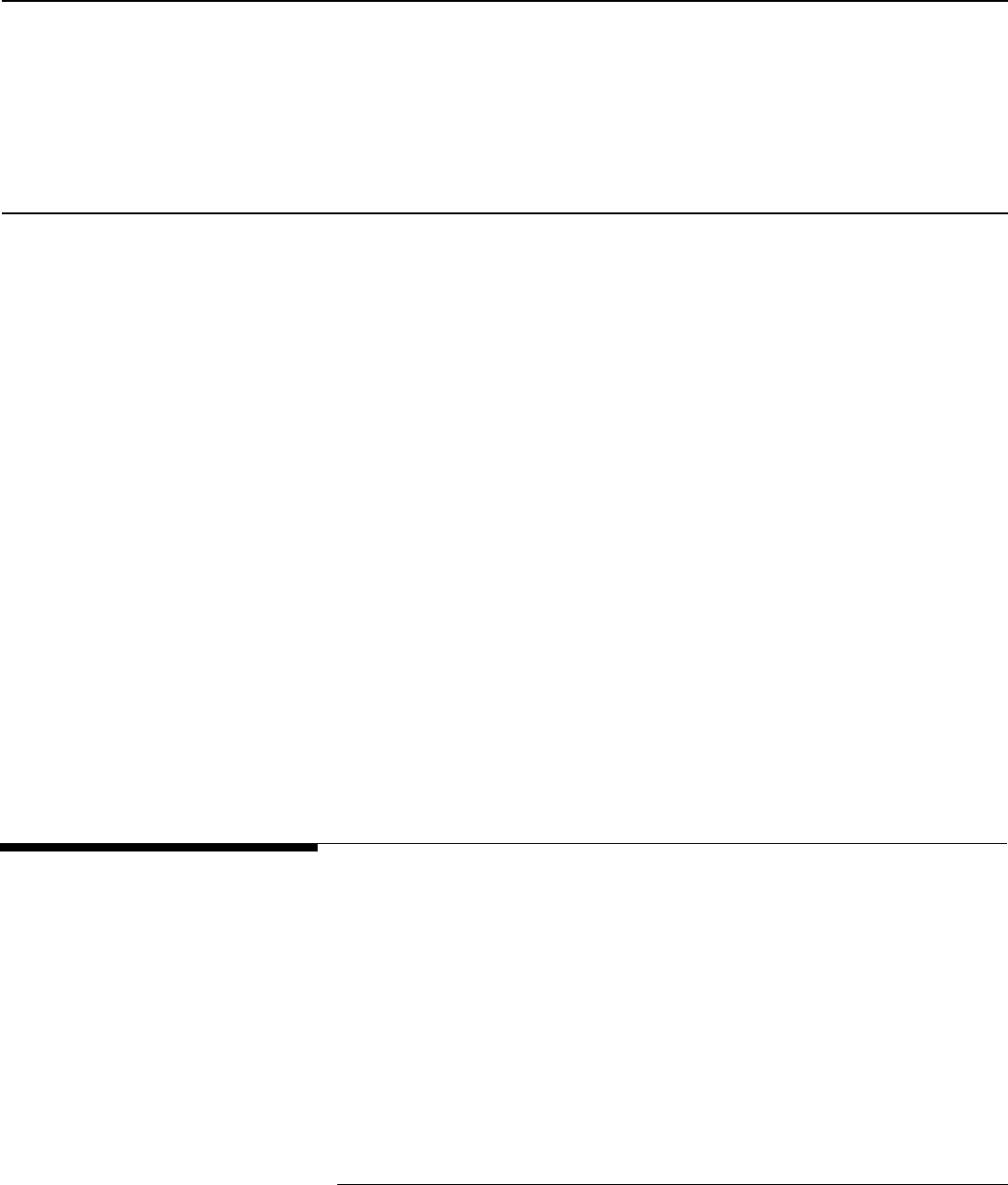
Page 29 GAO-22-105018 Contact Tracing for Air Travel
modernization plan, according to officials. However, officials said CDC put
those efforts on hold during the height of the pandemic to focus resources
on their response efforts. In April 2022, officials told us they had
recommenced efforts to identify and define system requirements but had
not finalized a work plan or timelines for when or if QARS would be
updated or replaced.
CDC officials fully acknowledged the system’s limitations, but said
competing priorities and resource constraints within the agency have thus
far curtailed any attempts to make improvements. OMB’s Federal Data
Strategy states, however, that an agency should provide resources
explicitly to leverage data assets, which includes ensuring that sufficient
human and financial resources are available to support the management,
maintenance, and use of strategic data assets, as well as data driven
agency decision-making.
56
The explanatory statement accompanying the Consolidated
Appropriations Act, 2022, designated an increase of $8 million for
quarantine programs, which as provided by the President’s proposed
budget for fiscal year 2022, would support modernizing public health
programs that protect U.S. communities from infectious diseases.
According to officials, modernizing QARS and other data systems that
connect CDC to state and local public health authorities would be among
the modernization efforts. CDC officials told us the agency is formulating
plans for specific funds.
The COVID-19 pandemic has revealed major shortcomings in CDC’s
process for facilitating contact tracing by state and local public health
authorities for passengers potentially exposed to communicable diseases
during flights. In a connected world, COVID-19 is not the first, and will
likely not be the last, communicable disease to spread quickly beyond
borders and threaten U.S. public health and the economy. Contact
tracing—when performed effectively in conjunction with other public
health measures like testing and quarantining—can help slow or stop the
chain of disease transmission. Given the role that air travel plays in the
initial and subsequent spread of communicable disease, CDC and local
public health authorities have an acute need to access high-quality
passenger contact information.
56
Office of Management and Budget, Executive Office of the President, Memorandum for
the Heads of Executive Departments and Agencies, Federal Data Strategy – A
Framework for Consistency (Washington, D.C.: June 4, 2019).
Conclusions

Page 30 GAO-22-105018 Contact Tracing for Air Travel
However, CDC faces significant challenges in collecting timely, accurate,
and complete passenger information. Recent efforts to improve the
quality of information it collects from airlines and CBP to facilitate contact
tracing have helped but mostly apply to passengers traveling on inbound
international flights—a small fraction of the total number of air travelers. In
addition, these efforts may only be temporary. Moreover, CDC has yet to
fully address limitations in its data entry process and in the system it uses
to manage air passenger contact investigations, resulting in unreliable
data that are of limited use.
In the short term, implementing sufficient data entry controls could enable
CDC to quickly improve the quality of its data. Further, undertaking
longer-term and more complex efforts—including assessing other ways to
improve the quality of air passenger information it collects and manages,
and updating or replacing its data system—can strengthen CDC’s ability
to monitor public health risks related to air travel, support contact tracing
by state and local health authorities, and evaluate and improve its own
processes.
We are making the following three recommendations to CDC:
The Director of CDC should implement controls for the entry of data into
its Quarantine Activity Reporting System (QARS), including by providing
adequate training and standard operating procedures that are
documented and institutionalized for system users and by conducting
consistent validation checks. (Recommendation 1)
The Director of CDC should assess additional opportunities to improve
the quality of air passenger information it collects and manages—
including opportunities to increase automation by adopting or establishing
data exchange standards—and take action, as appropriate, based on this
assessment. (Recommendation 2)
The Director of CDC should re-design QARS or deploy a new data
system that would allow CDC to more effectively facilitate contact tracing
for air passengers and conduct disease surveillance for air travel.
(Recommendation 3)
We provided a copy of this report to HHS, DHS, and DOT for review and
comment. In written comments reproduced in appendix II, HHS concurred
with our recommendations. DOT, DHS, and HHS also provided technical
comments, which we incorporated as appropriate.
Recommendations for
Executive Action
Agency Comments

Page 31 GAO-22-105018 Contact Tracing for Air Travel
We are sending copies of this report to the appropriate congressional
committees, the Secretary of the Department of Transportation, the
Secretary of the Department of Health and Human Services, the
Secretary of the Department of Homeland Security, and other interested
parties. In addition, the report is available at no charge on the GAO
website at http://www.gao.gov.
If you or your staff have any questions about this report, please contact
for our Offices of Congressional Relations and Public Affairs may be
found on the last page of this report. GAO staff who made key
contributions to this report are listed in appendix III.
Heather Krause
Director, Physical Infrastructure

Page 32 GAO-22-105018 Contact Tracing for Air Travel
List of Addressees
The Honorable Patrick Leahy
Chairman
The Honorable Richard Shelby
Vice Chairman
Committee on Appropriations
United States Senate
The Honorable Ron Wyden
Chairman
The Honorable Mike Crapo
Ranking Member
Committee on Finance
United States Senate
The Honorable Patty Murray
Chair
The Honorable Richard Burr
Ranking Member
Committee on Health, Education, Labor, and Pensions
United States Senate
The Honorable Gary C. Peters
Chairman
The Honorable Rob Portman
Ranking Member
Committee on Homeland Security and Governmental Affairs
United States Senate
The Honorable Rosa L. DeLauro
Chair
The Honorable Kay Granger
Ranking Member
Committee on Appropriations
House of Representatives
The Honorable Frank Pallone, Jr.
Chairman
The Honorable Cathy McMorris Rodgers
Republican Leader
Committee on Energy and Commerce
House of Representatives

P
age 33 GAO-22-105018 Contact Tracing for Air Travel
The Honorable Bennie G. Thompson
Chairman
The Honorable John Katko
Ranking Member
Committee on Homeland Security
House of Representatives
The Honorable Carolyn B. Maloney
Chairwoman
The Honorable James Comer
Ranking Member
Committee on Oversight and Reform
House of Representatives
The Honorable Peter A. DeFazio
Chair
Committee on Transportation and Infrastructure
House of Representatives
The Honorable Richard E. Neal
Chairman
The Honorable Kevin Brady
Republican Leader
Committee on Ways and Means
House of Representatives
The Honorable Rick Larsen
Chair
Subcommittee on Aviation
Committee on Transportation and Infrastructure
House of Representatives
Appendix I: Objectives, Scope, and
Methodology
Page 34 GAO-22-105018 Contact Tracing for Air Travel
This report examines: (1) the factors that affect CDC’s ability to collect
timely, accurate, and complete air passenger contact information from
airlines and other sources; (2) the actions CDC has taken since the onset
of the COVID-19 pandemic to improve the quality of air passenger
contact information it collects; and (3) how effectively CDC collects and
manages air passenger contact information to facilitate contact tracing.
Contact tracing scenarios and process steps. This report focuses on
how CDC collects and manages contact information for passengers
traveling on inbound international and domestic interstate scheduled
flights. We focused on scenarios when the infected passenger is
identified after a flight.
1
Because the contact tracing process for airline
crew (e.g., flight attendants and pilots) is separate from that of
passengers, we excluded the process for collecting contact information
from airline crews from our review. We also excluded from our review any
efforts for identifying contacts outside the aircraft, such as when infectious
travelers may have come into contact before or after a flight with
transportation security officials or airport workers. We did not review the
methods used by public health authorities to conduct contact tracing after
obtaining air passenger contact information from CDC.
Federal departments and components. We assessed the activities of
three federal departments—the Departments of Health and Human
Services (HHS); Homeland Security (DHS); and Transportation (DOT).
We selected these departments because they represent the key federal
departments with roles for facilitating contact tracing for potentially
exposed air passengers. Within these three departments we collected
and reviewed available documentation and interviewed officials from
various components that play a key role at their respective departments,
principally HHS’s CDC, DHS’s U.S. Customs and Border Protection
(CBP), and DOT’s Federal Aviation Administration (FAA).
Selected CDC quarantine stations. We interviewed officials from four
CDC quarantine stations co-located with international airports: Atlanta
(Hartsfield-Jackson Atlanta International Airport); Chicago (O’Hare
1
In some cases, airlines may report that a passenger onboard the aircraft has symptoms
of an infectious disease to CDC, who then alert the public health authority within relevant
jurisdictions. CDC regulations require airlines to report travelers with certain signs and
symptoms of disease, and all deaths that occur during international flights coming into the
United States. 42 C.F.R. § 71.21. When this occurs, CDC may collect air passenger
contact information directly through a passenger locator form from travelers on impacted
flights, and CDC may use the passenger data to perform the contact investigation
themselves.
Appendix I: Objectives, Scope, and
Methodology
Scope

Appendix I: Objectives, Scope, and
Methodology
Page 35 GAO-22-105018 Contact Tracing for Air Travel
International Airport); Los Angeles (Los Angeles International Airport);
and San Francisco (San Francisco International Airport). We selected
these four quarantine stations from the 20 total stations based on several
factors, including high volume of international and domestic passengers
at airports co-located with the quarantine station, number of states within
the geographic jurisdiction of the quarantine station, recommendations
from federal and aviation industry stakeholders, and additional factors,
such as if the quarantine station is co-located at an airport in which an
airline we interviewed is headquartered.
2
We selected these factors in
order to obtain a breadth of perspective on CDC’s collection and
management of air passenger information as these quarantine stations
would likely have routinely conducted contact investigations both before
and during the COVID-19 pandemic, as well as had regular contact with
airlines that provided both domestic and international flights. The views of
the officials we spoke with from these quarantine stations are not
generalizable to the views of all officials working in CDC’s quarantine
stations.
Selected airlines. We interviewed or received written responses from six
selected U.S. commercial passenger airlines: American Airlines, Delta Air
Lines, JetBlue Airways, Southwest Airlines, Spirit Airlines, and United
Airlines. To select these airlines, we first identified U.S. scheduled large
passenger airlines that had operating revenues of $1 billion or more
during calendar year 2019.
3
We then selected these airlines based on
international flights’ passenger volume, the operation of both international
and domestic flights, recommendations from stakeholders, and other
unique factors, such as booking and seating practices, among other
2
To determine passenger volumes at airports, we used airline data for flights and
passengers by airports for passengers on U.S. mainline passenger airlines traveling from
international and domestic destinations in the U.S. for calendar year 2019. We obtained
these data from Diio, a private contractor that provides online access to U.S. airline
financial, operational, and passenger data with a query-based interface. We used
calendar year 2019 data because it is more representative of typical market activity prior
to the COVID-19 pandemic
3
Bureau of Transportation Statistics classifies as “Group III” airlines. We used calendar
year 2019 Bureau of Transportation Statistics groupings to match the most recent year of
passenger volume data available, which in calendar year 2019 included 10 mainline
passenger airlines in group III.

Appendix I: Objectives, Scope, and
Methodology
Page 36 GAO-22-105018 Contact Tracing for Air Travel
characteristics.
4
The views of these airlines are not generalizable to all
U.S. commercial airlines operating scheduled flights. We also did not
consider regional passenger airlines or air taxis in our selection because
regional airlines typically operate domestic flights on behalf of mainline
carriers. As a result, few regional airlines collect or transmit passenger
data to CDC for contact tracing. We also did not include cargo airlines or
charter flights in our selection because of their more limited role with
respect to contact tracing for air travelers.
To address our objectives, we reviewed relevant statutes and regulations.
For example, we reviewed a number of regulatory documents including
CDC’s 2005 proposed rule, 2017 final rule, and 2020 Interim Final Rule
for the Control of Communicable Diseases, as well as associated
implementing orders and submitted public comments.
5
We also reviewed
publications and studies from CDC, industry, and academia on topics
related to contact tracing for air travel. These documents were identified
and selected based on a search of relevant literature published between
January 2016 and March 2021.
6
To better understand factors affecting CDC’s process to collect and
manage air passenger contact information we reviewed policies,
guidance, and other documentation relevant to CDC’s process. In
particular, we reviewed CDC’s guidance to airlines and the public
regarding this process,
7
a 2004 CDC-commissioned study on the
4
We identified airlines with the highest volume of passengers traveling on international
flights through Diio airline market data for onboards on U.S. mainline passenger airlines
traveling from international destinations to the U.S. for calendar year 2019. We did not
consider domestic flight volume as the recent efforts undertaken by CDC to improve its
process to collect air passenger information only involved inbound international flights.
5
We reviewed 42 C.F.R. part 71, including proposed and final rules issued in 2005, 2017,
and 2020 (see, e.g., 85 Fed. Reg. 7874 (Feb. 12, 2020)). These regulations describe
CDC’s authority to collect air passenger information for inbound international flights. We
also reviewed 42 C.F.R. part 70, which describes CDC’s authority to collect air passenger
information for interstate flights.
6
The search was conducted in the following databases: EBSCO, ProQuest, ProQuest
Dialog, and Scopus.
7
See, for example, U.S. Centers for Disease Control and Prevention, Protecting Travelers’
Health from Airport to Community: Investigating Contagious Diseases on Flights (Atlanta,
GA.), accessed Feb. 16, 2021, https://www.cdc.gov/quarantine/contact-investigation.html.
Methodology

Appendix I: Objectives, Scope, and
Methodology
Page 37 GAO-22-105018 Contact Tracing for Air Travel
agency’s contact tracing process,
8
and a Memorandum of Understanding
between HHS and DHS establishing specific cooperation mechanisms to
enhance preparedness against the introduction, transmission, and spread
of communicable diseases from foreign countries into the U.S.
9
We also
interviewed officials or received written responses from the three selected
federal departments and respective components, the four CDC
quarantine stations, and representatives from the six selected airlines
identified above. We also interviewed representatives from five industry
groups representing the aviation sector,
10
two associations representing
local public health authorities,
11
two global distribution systems
companies,
12
and Travel Technology Association, a travel industry
association, to obtain broader stakeholder perspectives on contact tracing
for aviation.
To describe the actions CDC’s has taken since the onset of the COVID-
19 pandemic to improve the quality of air passenger contact information it
collects, we reviewed CDC regulatory documents related to its Interim
Final Rule and associated implementing orders, including technical
instructions to airlines, documents submitted to the Office of Management
and Budget to fulfil requirements related to the Paperwork Reduction Act,
and the Privacy Impact Assessment for QARS. We also reviewed
applicable CBP documents including information on the expansion of
8
Volpe National Transportation Center, Real-Time Data for CDC Location of At-Risk
Passengers: Final Report (Cambridge, MA: June 29, 2004).
9
Memorandum of understanding between the Department of Health and Human Services
and the Department of Homeland Security (October 2005).
10
We interviewed the following aviation industry groups: Airlines for America, International
Air Transport Association, National Air Carrier Association, and Regional Airline
Association.
11
We interviewed the following associations representing local public health authorities:
Association of State and Territorial Health Officials and National Association of County
and City Health Officials.
12
Global distribution systems are computer systems that display airline flight schedule and
fare information so that travel agents can query it to “book” (i.e., reserve and purchase)
flights for consumers. We interviewed the following companies: Amadeus and TravelPort.

Appendix I: Objectives, Scope, and
Methodology
Page 38 GAO-22-105018 Contact Tracing for Air Travel
coordination efforts between CDC and CBP in collecting information for
passengers traveling on inbound international flights.
13
For contextual information on how CDC’s actions compare to other
countries, we reviewed documents and interviewed officials from public
health, border protection, and transportation agencies of the three
selected countries: Canada, Australia, and the United Kingdom. To select
these countries, we first identified countries with foreign contact tracing
programs or initiatives as of April 2021.
14
We then identified from that list,
countries that had one million or more passengers arrive or depart on
direct flights to and from the United States in calendar year 2019 based
on DOT data.
15
We then selected these three countries to provide a
variety of regions and locations.
16
We also considered other unique
factors, such as characteristics of the country’s data collection program
(e.g., collection mechanism); similarities to the United States (e.g.,
privacy laws); and recommendations from other stakeholders.
To assess CDC’s ability to effectively collect and manage air passenger
contact information, we reviewed available federal agency documentation
on data strategies and our past work on public health threat response and
data management systems to identify leading practices for maintaining
and using health data to inform agency activities and respond to disease
13
Department of Homeland Security, Privacy Impact Assessment for the CBP Support of
CDC for Public Health Contact Tracing, DHS/CBP/PIA-066a (Washington, D.C.: Feb. 12,
2021).
14
We identified 97 countries that have programs to electronically collect passenger
information for public health purposes, most of which have been initiated due to the
COVID-19 pandemic.
15
We identified 16 countries under this criteria based on Diio airline data. In addition, we
considered data only from 2019 because it represents more typical flight patterns than
2020 data due to the COVID-19 pandemic. We also only considered flights operated by
U.S. airlines.
16
For variety, we did not select more than one country in the following regions: North
America, Central America, Caribbean, South America, Europe, Central and Southeast
Asia, and Pacific. We also selected at least one country in Europe and one country in
North America due to the higher volume of flights between the United States and
European Union and North America, and due to European privacy laws that airlines have
identified as of particular concern for contact tracing programs.

Appendix I: Objectives, Scope, and
Methodology
Page 39 GAO-22-105018 Contact Tracing for Air Travel
events.
17
We also reviewed leading practices GAO has previously
identified for program evaluation and performance measurement and
evaluation.
18
We compared CDC’s current process to collect and manage
air passenger contact information with relevant portions of these criteria.
We also determined that the control activities component of internal
control was significant to this objective, along with the three underlying
principles that management should design the entity’s information system
and related control activities to achieve objectives, respond to risks and
implement control activities through policies, and develop monitoring
activities, including periodic evaluations.
19
Specifically, we assessed the
agency’s process to collect and manage contact investigation data to
determine whether it was capable of meeting current program objectives
as described in agency documentation.
20
17
Office of Management and Budget, Executive Office of the President, Memorandum for
the Heads of Executive Departments and Agencies, Federal Data Strategy – A
Framework for Consistency (Washington, D.C.: June 4, 2019). For our previous work on
public health threats and disease response, see, for example, GAO, Emerging Infectious
Diseases: Asian SARS Outbreak Challenged International and National Responses,
GAO-04-564 (Washington, D.C.: Apr. 28, 2004); Air Travel and Communicable Diseases:
Comprehensive Federal Plan Needed for U.S. Aviation System’s Preparedness,
GAO-16-127 (Washington, D.C.: Dec. 16, 2015); and COVID-19: Federal Efforts Could be
Strengthened by Timely and Concerted Actions, GAO-20-701 (Sept 21, 2020). For our
previous work on data management systems, see, for example, GAO, Oil and Gas Wells:
Bureau of Land Management Needs to Improve Its Data and Oversight of Its Potential
Liabilities, GAO-18-250 (Washington, D.C.: May 16, 2018); Oil and Gas: Interior Should
Strengthen Management of Key Data Systems Used to Oversee Development on Federal
Lands, GAO-21-209 (Washington, D.C.: May 27, 2021); and COVID-19: Data Quality and
Considerations for Modeling and Analysis, GAO-20-635SP (Washington, D.C.: July 30,
2020).
18
GAO, Program Evaluation: Strategies to Facilitate Agencies’ Use of Evaluation in
Program Management and Policy Making, GAO-13-570 (Washington, D.C.: June 26,
2013); Performance Measurement and Evaluation: Definitions and Relationships,
GAO-11-646SP (Washington, D.C.: May 2011); and Managing For Results: Enhancing
Agency Use of Performance Information for Management Decision Making, GAO-05-927
(Washington, D.C.: Sept. 9, 2005).
19
GAO, Standards for Internal Control in the Federal Government, GAO-14-704G
(Washington, D.C.: Sept. 10, 2014).
20
See U.S. Centers for Disease Control and Prevention, A CDC Framework for Preventing
Infectious Diseases: Sustaining the Essentials and Innovating for the Future (Atlanta, Ga.:
October 2011); National Center for Emerging and Zoonotic Infectious Diseases Strategic
Plan: 2018-2023 (Atlanta, Ga.: August 2018); and Information Technology Strategic Plan
(ITSP) FY 2021-FY 2023 (Atlanta, Ga), accessed Apr. 22, 2022,
https://www.cdc.gov/od/ocio/it-strategic-plan/2021-23/overview/goal1/index.html.
Appendix I: Objectives, Scope, and
Methodology
Page 40 GAO-22-105018 Contact Tracing for Air Travel
We also reviewed the reliability of CDC’s data collected and managed in
its Quarantine Activity Reporting System (QARS). To assess the reliability
of contact investigation data, we interviewed CDC officials about how the
data were collected, managed, and used, and the steps CDC takes to
ensure the data are accurate, complete, and reliable. We also requested
that CDC provide us with contact investigation information from 2015
through 2020, such as the number of manifest requests CDC submitted to
airlines or the total number of passengers who were exposed and
warranted a contact investigation, among other things. CDC officials told
us that they were unable to provide this information with sufficient
reliability and ease due to irregularities in data quality and system
limitations within QARS. Instead, they provided a sample of extracted
data from a 3-month period in 2021. They also provided us the results of
data system queries we requested for each year between 2015 and 2020
with explanations of the limitations of its reliability, query results which we
used in our report to provide contextual information. We then reviewed
any available documentation related to procedures for data entry,
validation, and management to determine the extent to which these
elements assisted with agency objectives and aligned with selected
control activities.
We conducted this performance audit from February 2021 to July 2022 in
accordance with generally accepted government auditing standards.
Those standards require that we plan and perform the audit to obtain
sufficient, appropriate evidence to provide a reasonable basis for our
findings and conclusions based on our audit objectives. We believe that
the evidence obtained provides a reasonable basis for our findings and
conclusions based on our audit objectives.
Appendix II: Comments from the Department
of Health & Human Services
Page 41 GAO-22-105018 Contact Tracing for Air Travel
Appendix II: Comments from the Department
of Health & Human Services

Appendix II: Comments from the Department
of Health & Human Services
Page 42 GAO-22-105018 Contact Tracing for Air Travel

Appendix II: Comments from the Department
of Health & Human Services
Page 43 GAO-22-105018 Contact Tracing for Air Travel

Appendix III: GAO Contact and Staff
Acknowledgments
Page 44 GAO-22-105018 Contact Tracing for Air Travel
In addition to the individual named above, Paul Aussendorf, Eric
Bachhuber, Sue Bernstein, Scott Borre, Jonathan Carver, Erin Guinn-
Villareal, Hayden Huang, Neelaxi Lakhmani, Diona Martyn, Josh Ormond,
Katherine Raymond, Kelly Rubin, Gretchen Snoey, Michael Soressi, and
Laurel Voloder made key contributions to this report.
Appendix III: GAO Contact and Staff
Acknowledgments
GAO Contact
Staff
Acknowledgments
(105018)

The Government Accountability Office, the audit, evaluation, and investigative
arm of Congress, exists to support Congress in meeting its constitutional
responsibilities and to help improve the performance and accountability of the
federal government for the American people. GAO examines the use of public
funds; evaluates federal programs and policies; and provides analyses,
recommendations, and other assistance to help Congress make informed
oversight, policy, and funding decisions. GAO’s commitment to good government
is reflected in its core values of accountability, integrity, and reliability.
The fastest and easiest way to obtain copies of GAO documents at no cost is
through our website. Each weekday afternoon, GAO posts on its website newly
released reports, testimony, and correspondence. You can also subscribe to
GAO’s email updates to receive notification of newly posted products.
The price of each GAO publication reflects GAO’s actual cost of production and
distribution and depends on the number of pages in the publication and whether
the publication is printed in color or black and white. Pricing and ordering
information is posted on GAO’s website, https://www.gao.gov/ordering.htm.
Place orders by calling (202) 512-6000, toll free (866) 801-7077, or
TDD (202) 512-2537.
Orders may be paid for using American Express, Discover Card, MasterCard,
Visa, check, or money order. Call for additional information.
Connect with GAO on Facebook, Flickr, Twitter, and YouTube.
Subscribe to our RSS Feeds or Email Updates. Listen to our Podcasts.
Visit GAO on the web at https://www.gao.gov.
Contact FraudNet:
Website:
https://www.gao.gov/about/what-gao-does/fraudnet
Automated answering system: (800) 424-5454 or (202) 512-7700
A. Nicole Clowers, Managing Director, ClowersA@gao.gov, (202) 512-4400, U.S.
Government Accountability Office, 441 G Street NW, Room 7125, Washington,
DC 20548
Chuck Young, Managing Director, youngc1@gao.gov, (202) 512-4800
U.S. Government Accountability Office, 441 G Street NW, Room 7149
Washington, DC 20548
Stephen J. Sanford, Managing Director, spel@gao.gov, (202) 512-4707
U.S. Government Accountability Office, 441 G Street NW, Room 7814,
Washington, DC 20548
GAO’s Mission
Obtaining Copies of
GAO Reports and
Testimony
Order by Phone
Connect with GAO
To Report Fraud,
Waste, and Abuse in
Federal Programs
Congressional
Relations
Public Affairs
Strategic Planning and
External Liaison
Please Print on Recycled Paper.
