NBER WORKING PAPER SERIES
LONG-TERM CARE IN THE NETHERLANDS
Pieter Bakx
Eddy Van Doorslaer
Bram Wouterse
Working Paper 31823
http://www.nber.org/papers/w31823
NATIONAL BUREAU OF ECONOMIC RESEARCH
1050 Massachusetts Avenue
Cambridge, MA 02138
November 2023
Results based on calculations by Erasmus University using non-public microdata from Statistics
Netherlands. We thank the Community Health Services, Statistics Netherlands & National
Institute for Public Health and the Environment for access to survey data from the Public Health
Monitor (Gezondheidsmonitor). Furthermore, we thank SCP Netherlands Institute for Social
Research for access to the SCP informal care survey and Mirjam de Klerk for providing advice
on using these data. The views expressed herein are those of the authors and do not necessarily
reflect the views of the National Bureau of Economic Research.
At least one co-author has disclosed additional relationships of potential relevance for this
research. Further information is available online at http://www.nber.org/papers/w31823
NBER working papers are circulated for discussion and comment purposes. They have not been
peer-reviewed or been subject to the review by the NBER Board of Directors that accompanies
official NBER publications.
© 2023 by Pieter Bakx, Eddy Van Doorslaer, and Bram Wouterse. All rights reserved. Short
sections of text, not to exceed two paragraphs, may be quoted without explicit permission
provided that full credit, including © notice, is given to the source.

Long-term care in the Netherlands
Pieter Bakx, Eddy Van Doorslaer, and Bram Wouterse
NBER Working Paper No. 31823
November 2023
JEL No. I10,I13,I18
ABSTRACT
We describe the financing and use of long-term care in the Netherlands. Public long-term care
insurance is universal and comprehensive; user fees are low compared to other countries. We use
linked survey and administrative data to document the distribution of the need for long-term care
in the 65+ population, long-term care costs and how they are paid for. The findings reveal that no
other country spends more per capita on publicly financed formal care than The Netherlands. A
potential reason is that the threshold to receive formal care appears to be lower in the Netherlands
than in other countries. Still, a considerable share of the adult population provides informal care.
Caregiving is concentrated in specific demographic groups. The costs of informal care provision
are considerable, but as a share of total spending on long term care they are smaller than in most
developed countries. Adding the costs of informal care to formal care expenditures changes the
view on who bears the costs of long-term care.
Pieter Bakx
Erasmus University Rotterdam
The Netherlands
Eddy Van Doorslaer
Erasmus University Rotterdam
The Netherlands
Bram Wouterse
Erasmus University Rotterdam
The Netherlands
1
Classification: Internal
Long-term care in the Netherlands
Pieter Bakx ([email protected])
Eddy van Doorslaer (vandoorslaer@ese.eur.nl)
Bram Wouterse (wouters[email protected]ur.nl)
Erasmus University Rotterdam
Acknowledgement
Results based on calculations by Erasmus University using non-public microdata from Statistics
Netherlands. We thank the Community Health Services, Statistics Netherlands & National Institute for
Public Health and the Environment for access to survey data from the Public Health Monitor
(Gezondheidsmonitor). Furthermore, we thank SCP Netherlands Institute for Social Research for
access to the SCP informal care survey and Mirjam de Klerk for providing advice on using these data.
Introduction
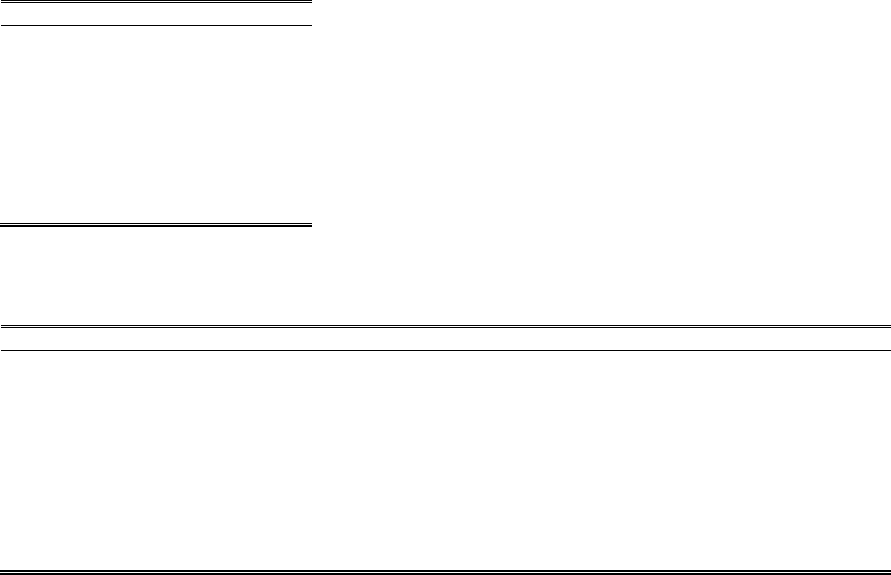
The Dutch population is aging rapidly (Figure 1). The share of the population over age 65 has grown
from 12% in 1990 to 22% in 2020 and is expected to be around 25% by 2050. This trend is similar to
trends in other European countries, including Germany and Denmark, and to the trend in the United
States (Gruber and McGarry 2023; Geyer et al. 2023; Gørtz et al. 2023). The share of the oldest old
has increased from about 1.5% in 1990 to currently about 2.5% and is expected to rise to nearly 6%
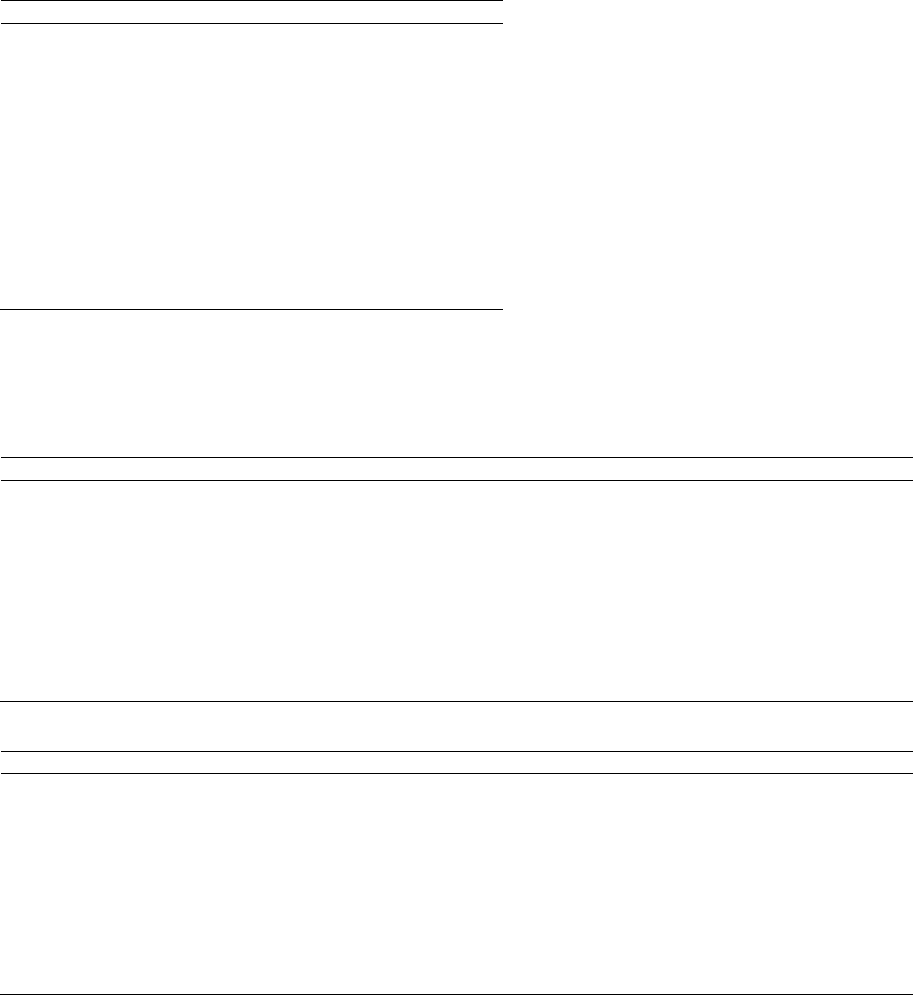
by 2050, which is a fourfold increase in just 60 years. Consequently, among the over 65, the share of
over 85 is expected to rise from 9% in 1990 to around 22% in 2050 (Figure 2). The growing share of
the oldest part of the population is, together with other – related – trends, likely to generate a rapid
rise in the need for assistance and care (De Meijer et al. 2013).
Will the public programs be able to keep funding most of the care for those increased needs when the
share of the working population is declining at the same time? The current public long-term care
insurance system in The Netherlands is more generous than in most other countries. The Netherlands
provides universal public long-term care insurance to its population, which is more comprehensive
than in many other OECD countries. This means broad access to good-quality home care and nursing
home care (Tenand et al. 2020, 2020a), while out-of-pocket costs are relatively low (Bakx et al. 2015),
and relatives may be better shielded against the burden of informal caregiving than in other countries
(Rellstab et al. 2020). But it also comes at the cost of having the highest public expenditures on long-
term care of all countries when expressed as the share of the gross domestic product (OECD 2022).
In this paper, we provide an overview of the long-term care use in The Netherlands and highlight
differences and similarities with other countries. We go beyond the care provided by professionals
and consider informal care provided by relatives, friends and others. While long-term care in the
Netherlands is available for everyone with chronic health problems that require care or support, we
focus on the 65+ population, which is the largest group of care recipients.
The remainder of this chapter is structured as follows. Part 1 discusses the care needs, well-being, and
costs of care for the 65+ population. Part 2 discusses how long-term care is financed and organized in
The Netherlands. Furthermore, Part 3 discusses the total costs of long-term care for the 65+
population.

2
Classification: Internal
Figure 1: Share of population ages 65 or older
Source: CBS 2020a, 2021
Figure 2: Share of 65+ population that is age 85 or older
Source: CBS 2020a, 2021
Part I: Aging, Disability and Well-Being
Sample and definitions
For this chapter, we use two sets of data. First, we use aggregate-level statistics when these were
available. These aggregate-level statistics have been generated by the OECD and Statistics
Netherlands (CBS), among others, and these sources are cited in the respective footnotes to the tables
and figures in which they are used.
Second, we use linked administrative and survey data for the year 2016. We use administrative
registers for the full Dutch population. These administrative registers are linked at the individual level
and include demographic information, information on income and wealth, and long-term care
eligibility and use. Where needed, we link these administrative records to data from the Public Health
Monitor survey of the Community Health Services, Statistics Netherlands and the National Institute
for Public Health and the Environment (Dutch Health Monitor 2016). From these survey data, we use
information on informal care provision and use, functional limitations, and measures of well-being.
Nursing home residents are undersampled in the Public Health Monitor. To deal with this, we apply
probability weights by gender and 5-year age groups to the analyses in which these data are used.
Appendix A contains a full list of all datasets used.
Long-term care use is defined as follows. Informal care receipt is measured over the 12-month period
prior to the interview, while formal care use is measured during the calendar year that we study (i.e.
0
0.1
0.2
0.3
1990 2000 2010 2020 2030 2040 2050
0
0.1
0.2
0.3
1990 2000 2010 2020 2030 2040 2050
3
Classification: Internal
2016). Home care consists of two types. First, it consists of nursing and personal care organized and
financed through the social health insurance scheme. Second, it includes domestic help, ADL or IADL
assistance, transportation, home adaptations and use of medical devices financed through the Social
Security Act. The data on this second set of formal care types only contain information on person-
specific care (i.e. tailored to one’s needs – maatwerkvoorzieningen) for which the user was charged a
copayment; use of other types of care and support (algemene voorzieningen) is not included because
of data limitations. Nursing home care includes care received in a nursing home or substitute care that
is received elsewhere, e.g. at home or another private setting such as a private care home; persons
choosing care vouchers (4%; Hussem et al. 2020) are excluded. While the latter type of nursing home-
like care has been growing in recent years, the total share of users who lived in a regular nursing home
was 84% in 2016 (Hussem et al. 2020), i.e. the year that this chapter focuses on. For this type of care,
we only include care use by persons who are eligible for elderly care (Verpleging en verzorging) rather
than care for the disabled or long-term mental health care, unless indicated otherwise. We do not
have information on fully private expenditures on long-term care but these are negligible and hence
this group of users is likely very small (Hussem et al. 2020).
In the Public Health Monitor survey data, functional limitations are measured using the OECD scale
rather than the activities of daily living scale (ADL) and the instrumental activities of daily living (IADL)
scales. Limitations defined as not being able to or having much difficulty with (1) listening to a
conversation with 3 or more persons; (2) having a conversation with one person; (3) reading the small
print of a newspaper; (4) recognizing someone’s face at 4 meters distance; (5) carrying an item of 5kg
for 10 meters; (6) reaching for something on the ground; (7) walking for 400 meters without standing
still. Using other Dutch survey data (Health Survey) that contains both scales, we compare scores on
this scale to scores on the 5-item versions of the ADL and IADL scales as used in the other chapters.
Based on the comparison (see Appendix), we conclude that the median person with 0-1 limitations on
the OECD scale does not report any limitation on the ADL or IADL scale; the median person with 2
limitations reports at least one IADL limitation, while the median person with 3 limitations on the
OECD scale has an ADL score of 1; the median person with 4 limitations on the OECD scale has an ADL
score of 2, with 5 limitations has 3 ADLs, etc. When grouping by the number of limitations, we group
individuals accordingly, to enable a direct comparison of the limitation groups used here to those
based on ADLs in the other chapters.
Prevalence of functional limitations
Ageing comes with increased functional impairment: 12% of individuals aged 65+ report three or more
limitations from the OECD list of functional limitations, and about 7% at least four (Table 1). These
shares rise steeply with age: for those 85+, 44% report having difficulty with at least three and 29%
with at least four limitations. Hence, the expected rapid rise in the share of the population aged 85+
(Figure 2) – and hence in the number of individuals with functional limitations – is likely to lead to a
substantial growth in the demand for care in the next few decades.
Table 2 details which limitations are most frequently reported by 65+ and 85+ respondents, both
overall and conditional on reporting any. As soon as at least one limitation is reported, the probability
of reporting other limitations also increases. For both age groups, and both unconditional and
conditional on reporting any limitations, the most frequently reported activity with severe limitation
is carrying an item of 5kg for 10 meters, while the least reported limitation is having a conversation
with one person.
4
Classification: Internal
Table 1: Share with functional limitations, by age
# of limitations
65+
85+
0-1
.82
.43
2
.06
.12
3
.05
.15
4
.03
.12
5
.02
.08
6
.01
.05
7
.01
.05
Observations
225,653
18,203
Note: functional limitations are measured using the OECD scale, see Appendix A for an explanation and a mapping of the
OECD scale and limitations based on the IADL and ADL lists.
Table 2: Distribution of each of the functional limitations, by age
Note: functional limitations are measured using the OECD scale, see Appendix A for an explanation and a mapping of the
OECD scale and limitations based on the IADL and ADL lists.
Well-being
Health problems
Next, we consider the self-perceived physical and depression scores at older ages (Table 5) by age of
the respondent and by number of functional limitations. Self-perceived health of the 85+ is much
lower than of those aged 65+: the 85+ subgroup is only half as likely to report that their health is good
or better. Furthermore, in both age groups, only 5% of the respondents with 5+ functional limitations,
rates their health as good or better.
Mental health also appears to fall with rising age and functional limitations. While only 6% of the
respondents aged 65+ has a high score on the depression scale, this percentage rises to 17% for the
85+. Among the group reporting 3+ functional limitations, the fraction with a high depression score
rises to around one-third in both groups. Furthermore, no less than 43% of the 65+ and 67% of the
85+ have a high or moderate depression score. The fraction with moderate or high depression scores
is 88% for both the 65+ and the 85+ with 3+ functional limitations. These findings are confirmed by
prior research (Bom et al. 2022) showing higher levels of loneliness and a perception of limited control
over one’s life among the oldest old, both among those living at home and those living in a nursing
home, when compared to the middle-aged population.
In sum, the health, income and wealth distributions show similar patterns as elsewhere, how these
distributions are correlated is similar as well. Yet, income poverty rates and inequality among Dutch
65+ are much lower than in other OECD countries.
65+
85+
All
Conditional on any
All
Conditional on any
Listening to a conversation with 3 or more persons
.11
.37
.36
.50
Having a conversation with one person
.03
.12
.13
.18
Reading the small print of a newspaper
.08
.28
.24
.33
Recognizing someone’s face at 4 meters distance
.04
.15
.16
.22
Carrying an item of 5kg for 10 meters
.17
.58
.55
.77
Reaching for something on the ground
.13
.43
.42
.58
Walking for 400 meters without standing still
.16
.55
.51
.71
Observations
225,653
57,829
18,203
11,359

5
Classification: Internal
Table 3 Well-Being for those 65+ and 85+ by functional limitations.
65+
65+ with 3+
functional
limitations
85+
85+ with 3+
functional
limitations
Self-Report of Health – Good or Better
.62
.10
.34
.10
Depression score: high
.06
.34
.17
.32
Depression score: moderate or high
.43
.88
.67
.88
Observations (unweighted)
219,683
16,787
17,294
5,078
Note: functional limitations are measured using the OECD scale, see Appendix A for an explanation and a mapping of the
OECD scale and limitations based on the IADL and ADL lists.
Financial situation
One determinant of the wellbeing of the older population is their financial situation. Table 3 examines
the distribution of standardized net household income and wealth for those aged 65 and older, and
85 and older. For this population, income is not always a very adequate measure of financial well-
being: older individuals above the retirement age who hold substantial assets may also use these
assets to finance consumption. Not surprisingly, the wealth distribution for the elderly shows greater
inequality than the income distribution. For instance, the bottom 5% of the 65+ wealth distribution
on average reports close to zero wealth, while the top 5% is holding around 644,000 euro on average.
The wealth inequality is slightly lower for individuals aged 85 and older.
The share of older people who have a standardized household income below 50% of the median is
low (Table 4, panel A). This suggests that Dutch pensions protect the incomes of older population well,
also at the bottom of the income distribution, and succeeds in keeping income inequality among the
elderly low. The Netherlands has the lowest poverty rate among all OECD countries included in the
OECD (2021) Pensions at a glance report, with 3% of the 65+ population having an income below 50%
of median equivalent household income. Furthermore, the poverty rate is lower than the poverty rate
for the entire Dutch population, which is 8.5%. In addition, the ratio of the median income to the
income at the 10
th
percentile is 1.4 for the 65+ population, which is the lowest among the OECD
countries included in the analysis, suggesting that income inequality is lower than elsewhere (OECD
2021).
Despite this extensive income protection, incomes and limitations are inversely related: as the number
of functional limitations rises, the share of the population in the lower income categories also tends
to rise (Table 4). For example, 39% of those with 0-1 functional limitations have an income between
50% and 100% of the median household income while this share rises to approximately two-thirds for
those with 3 or more functional limitations. Yet, the negative relationship between income and
number of functional limitations is much weaker than in the U.S. (Gruber and McGarry 2023). The
picture looks very similar for the relationship between wealth and functional limitations in Panel B:
the lower wealth groups are more likely to report more functional limitations than the groups with
higher wealth.
6
Classification: Internal
Table 4: Income and wealth distribution
Income in 1000s
Wealth in 1000s
65+
85+
65+
85+
Percentile
5
14
14
0
1
10
16
15
1
3
25
18
17
12
12
50
23
20
89
43
75
30
26
218
206
90
39
34
414
398
95
47
41
644
597
Mean
26
23
201
173
Observations
3,281,069
420,208
3,281,009
420,207
Notes: 2015 figures for the population on 1/1/2016. All figures converted to 2019 euros using consumer price index
information for 2015-2019 (CBS 2022). Income refers to standardized disposable household income; wealth is standardized
total household wealth. Standardized using the OECD equivalence scale.
Table 5: Income and wealth distribution by functional limitations for 65+ population
Panel A: Income
Functional limitations
% of median standardized household income
0-1
1
3
4
5+
Share of total in row
<50
.01
.01
.01
.01
.01
.01
50-100
.39
.60
.64
.67
.64
.43
100-150
.39
.29
.27
.24
.24
.37
150-200
.15
.07
.06
.06
.09
.13
200+
.07
.03
.02
.02
.02
.06
Share of total in column
.82
.06
.05
.03
.04
Observations
184,328
13,607
12,225
6,348
8,846
Panel B: wealth
Functional limitations
% of median standardized household wealth
0-1
1
3
4
5+
Share of total in row
<50
.30
.46
.53
.52
.53
.33
50-100
.10
.09
.09
.09
.09
.10
100-150
.11
.09
.07
.06
.05
.10
150-200
.11
.08
.07
.06
.07
.10
200+
.38
.27
.24
.26
.25
.36
Share of total in column
.82
.06
.05
.03
.04
Observations
184,355
13,607
12,227
6,348
8,848
Note: Shares displayed are shares within the column, unless indicated otherwise. Income refers to standardized disposable
household income; wealth to standardized household wealth. Standardized using the OECD equivalence scale. Median
income is median standardized household income for the 65+ population; median wealth is median standardized household
wealth for the 65+ population. The share of people with above median income or wealth is not equal to .5 because of
undersampling of lower-income individuals in the Public Health Monitor data that is not corrected for through sample
weights.
Care received
Table 6 reports the distribution of nursing and personal care use (panel A) and of informal caregiving
(panel B) expressed in hours per week. The numbers from the two panels are not directly comparable
and hence no overall distribution of care hours is reported. Panel A reports the distribution based on
annual (administrative) data; Panel B is based on current users at the time of the survey. Because
some individuals use care for only part of the year (e.g. after a hospital admission or illness), the
number of hours reported in Panel A underestimates the number of weekly hours used by users in the

7
Classification: Internal
weeks that they use care. Furthermore, nursing and personal care do not represent total formal home
care use; data on the number of hours of domestic help, guidance and support are not available.
Among users of nursing and personal care, the distribution is highly skewed (Panel A): while the
median users aged 65 only uses 1 hour per week (1.6 for 85+), this rises to 7.7 hours for the 95th
percentile (7.8 for 85+). Panel B highlights that the distribution of informal care among users is even
more skewed, ranging from only 1 (for 65+) or 2 (85+) reported hours per week at the 5th percentile
to 168 (65+) and 105 hours (85+).
Nursing home care is an alternative to formal or informal care at home. In the Netherlands, most
nursing home admissions are the final stage of life and only few residents return to their homes after
admission. Table 7 reports the lengths of stay for nursing home residents in 2016. The distribution is
highly skewed: while the average resident had lived in a nursing home for almost three years, the
median is only about 2 years. At the tails, the 90
th
percentile is at 6 years, while the 10
th
percentile is
at just over 3 months.
The total costs for home care would be a substantial share of a user’s income or wealth if they had to
pay these costs out-of-pocket: the amount of home care that users use on a weekly basis (Table 6)
valued at the going rate of one hour of home care comprises a substantial share of the income for
many older people (Table 3). For instance, one year of 3 hours of home care per week, which is close
to the 75
th
percentile of the distribution in Table 6, would cost close to 9,000 euro per year (2019 price
level) and that would be almost half of the median income of the 85+ population (Table 3).
Furthermore, the cost of a 2-year nursing home admission at 175 euro per day (dementia care, 2016
price level) would cost approximately 130,000 euro, and hence exceed the income and wealth of most
older persons. Wouterse et al. (2022) estimate that a Dutch 65-year-old will use, on average, 75,000
euro of formal long-term care over their remaining lifetime, with the top 5 percent of biggest users
using over 320,000 euro of care. In the Netherlands, most of these costs are covered through social
insurance. Despite this extensive coverage, user fees for nursing home care pose a financial risk. The
remainder of this chapter discusses the public long-term care system in the Netherlands and what is
means for the distribution of the costs of long-term care.
Table 6 Distribution of weekly hours of home care received in last month by type.
Panel A: Distribution of weekly hours of nursing and personal care, among users.
65+
85+
Percentile
5
0.0
0.1
10
0.1
0.1
25
0.3
0.5
50
1.0
1.6
75
2.9
3.7
90
5.5
6.4
95
7.7
8.7
Mean
2.1
2.7
Observations
443,366
161,767
Note: conditional on receiving any nursing or personal care at some point during the calendar year. Administrative registers
report total expenditures on nursing and personal care. This is approximately 42% of all formal home care in terms of
expenditures (Bakx et al. 2021). Annual expenditures are converted to weekly hours using the average price per hour
reported by NZa (2019): 54.42 euro.

8
Classification: Internal
Panel B: Distribution of weekly hours of informal care, among informal care recipients
65+
85+
Percentile
5
1
2
10
2
2
25
4
4
50
9
8
75
21
15
90
80
40
95
168
105
Mean
25.5
19.7
Observations
17,340
5,291
Note: conditional on receiving any informal care in the period directly prior to the interview.
Table 7 Distribution of nursing home stay lengths
65+
Days since admission
Average
996
Median
731
10
th
percentile
103
90
th
percentile
2,470
Share in nursing home in 2+ years
.50
Observations
193,202
Note: all users of nursing home care in 2016. If users had multiple stays during 2016, the length of stay was added over all
stays, thus mimicking survey data asking about the total length of stay during the year.
PART II: Long-term care system
Public financing
The Dutch health care system aims to provide affordable care of good quality to all its citizens.
Universal health coverage has been in place in the Netherlands for decades and has included long-
term care as early as 1968. There is no private long-term care insurance in the Netherlands.
1
This universal health coverage is achieved through three complementary public financing schemes
that each pay for specific types of care (Table 8). First, social long-term care insurance pays for
institutional care (including nursing homes and hospice care). Second, social health insurance pays for
nursing and personal care provided at home. Third, the Social Support Act makes municipalities
responsible for organizing and financing assistance and social support for elderly living in their
community. Each of these public schemes pays for care for the full population
2
.
Enrolment in the social insurance schemes is mandatory. The two social insurance schemes are
primarily funded through earmarked insurance premiums, and the Social Support Act is fully financed
1
Hence, the section about private long-term care insurance that is included in other chapters is omitted.
2
In addition to elderly care, the three schemes also cover care for individuals with severe physical or sensory
disabilities, and care for individuals with a long-term mental illness. For this reason, this part reports
expenditures for all types of long-term care for the full adult population. This is also what is reported in other
international comparisons, e.g. those done by the OECD, and what is focused on in this part of the chapter. Part
3 reports expenditure calculations for the 65+ population.

9
Classification: Internal
through general taxation. Cost sharing is relatively low (Figure 4).
3
Income-dependent co-payments
amount to 7% of spending on institutional care, and a deductible on home care financed through the
Social Support Act pays for 4% of the expenditures on home care (Figure 6). There is no cost sharing
for home care paid for through social health insurance. This financing mix implies substantial
intrapersonal (across the life-cycle) and interpersonal (from the healthy to those with limitations)
redistribution (Bakx et al. 2016).
Table 8: Main characteristics of public long-term care financing
Scheme
Social long-term care
insurance
Social health insurance
Social Support act
Type of LTC covered
Nursing home care
a
Nursing and personal
care at home
Assistance and social
support
How it is paid for
Income-related
insurance premiums and
general taxation,
income-related co-
payments
Insurance premiums
(partially income-
related), general
taxation
b
General taxation,
deductible
Eligibility for coverage
Full population, mandatory or automatic enrolment
How benefits are paid
In-kind provision, beneficiaries may opt for a cash benefit
What is covered
Formal care, but cash benefits may also be used to pay informal caregivers (few
% of expenditures)
Notes:
a
Including intensive (around the clock) care in other settings;
b
Home care covered through public health
insurance is exempted from the deductible. Source: adapted from Bakx et al. 2021.
Expenditures
This universal and comprehensive coverage of long-term care expenditures comes at a cost. The
Netherlands spends 4.0% of its Gross Domestic Product on long-term care (Figure 3), which is more
than any other country (OECD 2022). Although cost containment has been mentioned as a policy
objective when announcing policy reforms, costs have kept increasing substantially over the past
decades, both in absolute amounts and as a share of GDP.
The share of long-term care expenditures devoted to institutional care versus home care has remained
constant (Figure 5), despite an increased number of the oldest old. Possibly this is in part because of
policy measures promoting ageing-in-place. Ageing-in-place has been an explicit policy goal for at least
three decades (De Meijer et al. 2015). This has led to a series of policy reforms, including increasing
the availability of home care and stricter eligibility rules for institutional care. The share of long-term
care expenditures devoted to institutional care is similar as in Germany (Geyer et al. 2023) but higher
than in the United States (Gruber and McGarry 2023) and in Denmark (Gørtz et al. 2023).
3
As Table 8 shows, eligibility for long-term care is not age-restricted. Figures 3 and 4 are for the full 18+
population; estimates for the 65+ population are available from cost-of-illness studies from RIVM (2022) and
show a similar trend. Expenditure data for the 65+ population are presented in Part 3 of this chapter.

10
Classification: Internal
Figure 3: Share of GDP spent on long-term care over time
Source: OECD 2022. Note: long-term care for the full 18+ population.
Figure 4: Percent of long-term care financing by source
Note: expenditures in million euro in 2020 for System of Health Accounts categories HC.3 (LTC Health) HCR.1 (LTC social)
taken together. Public expenditures are category HF1; out-of-pocket expenditures are HF3, which equals HF3.2 (cost sharing)
because HF3.1 (direct out-of-pocket payments) equals zero. Long-term care for the full 18+ population. Source: CBS 2022a.
0
1
2
3
4
5
1972 1980 1990 2000 2010 2020
% of GDP
Total Long-term care (health, after 1998)
Long-term care (social) Long-term care (health, pre-1998)
Public
insurance, 94%
Out-of-pocket,
6%

11
Classification: Internal
Figure 5: Spending on institutional care versus home care
Source: OECD 2022. Notes: definitions according to System of Health Accounts. Home care is defined as System of Health
Accounts categories HC.3.2-HC.3.4 and HCR.1. Institutional care is defined as System of Health Accounts category HC.3.1.
Definitions changed in 1998; the reason for the change in 1988 is unknown. Long-term care for the full 18+ population.
Figure 6. Expenditures on home care and institutional care, by source of funds.
Source: CBS (2022b). Note: long-term care for the full 18+ population in 2020.
0%
50%
100%
1972 1980 1990 2000 2010 2020
Expenditures, % of total by type
Inpatient long-term care (health) Home care
Public insurance,
96%
Out-of-pocket,
4%
Home care
Social insurance
(WLZ), 93%
Co-payments
(WLZ), 7%
Institutional care

12
Classification: Internal
Allocation and contracting
Eligibility for benefits is assessed for each of the three schemes separately and is done by different
organizations using different sets of rules (see Bakx et al. 2021 for details). However, in all cases,
eligibility is only based on need and not restricted to certain subgroups in the population according to
e.g. income or age. A substantial share of all applications for eligibility to care financed through Social
long-term care insurance is rejected (Algemene Rekenkamer 2018). These rejections may have a
number of reasons, e.g. applicants may not meet the requirements for eligibility, may end the
application process or is referred to care financed through another scheme. Tenand et al. (2020a,
2020b) find that among the 65+ population, there is no variation in the probability of being eligible by
income, age and other non-need factors after controlling for differences in need studying data from
2012. However, there is some variation in long-term care use conditional on entitlements by
socioeconomic and demographic characteristics.
Individuals who are eligible for long-term care may choose between care in-kind or a voucher (cash
benefit) that they may use to contract a care provider themselves. In-kind benefits are provided by
private organizations. These providers are contracted by a contracting party: municipalities contract
providers of social support and assistance (Social Support Act), health insurers contract providers of
nursing and personal care (Social health insurance) and regional single-payers contract institutional
care providers (Social long-term care insurance). Providers negotiate an annual contract and are paid
on a fee-for-service basis. In addition, contracts may include a budget ceiling. Home care providers
may be for-profit or non-profit organizations, institutional care providers are all non-profit
organizations. Vouchers may be used to contract non-professional caregivers, including family
members. However, the share of informal caregivers that reports getting paid is merely 3% (SCP 2015).
In addition to the choice between care in-kind and a voucher, individuals who are eligible for
institutional care may choose to receive care in-kind in an institutional setting or at home or another
private setting.
4
The other housing options are all private initiatives, either set up by residents or by
other private parties (for-profit or non-profit). These include e.g. assisted living facilities, homes that
may be fully adapted to the resident’s functional limitations and apartments that are built next to a
nursing home and that enable people to use some facilities of the nursing home. Care that is received
by people living in such housing arrangements is usually funded through the public system and for this
care the same eligibility criteria apply as for all other home care and institutional care. When care is
used in an institutional setting, the costs of room and board are covered by the social insurance. In
other settings, these costs are paid by the individual.
There is a growing niche market for high-end nursing home care with about 300 high-end nursing
homes that accounted for about 5,400 residents in 2019 (SCP 2019). Standard care is typically publicly
funded but these nursing homes allow topping up for additional services and require payments for
room and board (Hussem et al. 2020).
Long-term care receipt
24% of the 65+ population uses either formal or informal long-term care, while 72% of the 85+
population does (Table 9). As expected, the probability of care use is strongly correlated with the
number of functional limitations that are reported and virtually all individuals with 5 or more
limitations use some type of care. These shares are considerably higher than in the United States and
Denmark, but substantially lower than in Germany (Gruber and McGarry 2023; Gørtz et al. 2023; Geyer
et al. 2023).
4
Care at home or in another private setting may be provided by for-profit providers.

13
Classification: Internal
Figures 7 and 8 zoom in on the mix of care types that is used. These figures highlight that a large share
receives formal home care: 52% of the care recipients aged 65+ (46% for the 85+), while the share of
care users who only receive informal care is only 19%, which is much smaller than in Denmark, the
United States and Germany, where more than half of all care users are in the latter group (Gruber and
McGarry 2023; Gørtz et al. 2023; Geyer et al. 2023). A large share of care users living at home reports
using both formal home care and informal care. Approximately 44% of all formal home care users also
receive informal care. Conversely, 55% of all informal care users also receive formal home care.
Furthermore, the type of care that is used differs by age: the share using nursing home care is higher
among those aged 85+ than among the total 65+ population (Figure 7).
The type of care used also differs by the number limitations (Figure 8). Those with fewer functional
limitations more often receive no care or care at home rather than in a nursing home. Furthermore,
more than half of those with 4+ limitations who receive care at home receive a combination of formal
home care and informal care instead of just one of these care types.
19% of the care recipients aged 85 or older who report no or only one limitation receive nursing home
care (Figure 8; 65+: 0.10). A potential explanation is the functional limitations used in this analysis
capture physical health problems requiring care or support, they are less likely to fully capture mental
and cognitive limitations, which may also require care or support, and thus be a reason for long-term
care use. Yet, this share is larger than the shares that are reported for the United States and Germany
using similar measures (Gruber and McGarry 2023; Geyer et al. 2023).
Table 9: Shares of elderly who received care, by age and functional limitations.
65+
85+
All
.24
.72
0-1 limitations
.12
.46
2 limitations
.56
.78
3 limitations
.78
.90
4 limitations
.87
.95
5+ limitations
.94
.98
Observations
225,653
18,203
Note: functional limitations are measured using the OECD scale, see Appendix A for an explanation and a mapping of the
OECD scale and limitations based on the IADL and ADL lists. The grouping used in this table is closest to the grouping used in
the other chapters. Source: own calculations based on linked survey and administrative data.
Figure 7: type of care received by age, conditional on using any care
Panel A: 65+
Informal
care, 0.19
Formal home
care, 0.29
Informal +
formal home
care, 0.23
Nursing
home care;
0.29

14
Classification: Internal
Panel B: 85+
Source: own calculations based on linked administrative and survey data.
Figure 8: Type of care by age and limitations, conditional on using any care
Panel A: 65+
Panel B: 85+
Note: functional limitations are measured using the OECD scale, see Appendix A for an explanation and a mapping of the
OECD scale and limitations based on the IADL and ADL lists. The grouping used in this table is closest to the grouping used in
the other chapters. Source: own calculations based on linked survey and administrative data.
Informal
care, 0.08
Formal home
care, 0.22
Informal +
formal home
care, 0.24
Nuring home
care; 0.45
0%
25%
50%
75%
100%
0 or 1 2 3 4 5+
Limitations
Informal care Formal home care
Informal + formal home care Nursing home care
0%
25%
50%
75%
100%
0 or 1 2 3 4 5+
Limitations
Informal care Formal home care
Informal + formal home care Nursing home care

15
Classification: Internal
Formal long-term care supply
Nursing homes
Table 10 reports that there are 1,922 nursing homes
5
, with 142 thousand beds, meaning that the
average nursing home has 74 beds. In addition, 9,000 individuals received institutional care in another
setting (TNO 2019). There is no publicly available information on occupancy rates by region, but
information on waiting lists for nursing home care (ZN 2022) suggests that there is substantial
variation in whether the supply of nursing homes is able to meet the demand: waiting lists are zero or
very small in most regions but substantial in some regions. Compared to other countries, the number
of beds in institutional settings (per 1000 65+) is above the OECD average (OECD 2022)
6
.
Table 10: Absolute number of nursing homes, beds, and occupancy rate.
Nursing homes
1,922 (2017 figure)
Nursing home beds in 1000: theoretical
165 (2017)
Nursing home beds in 1000: operational
152 (2018)
Nursing home beds in 1000s contracted
142
Nursing home occupancy rate
.935 (2018)
Population size 65+
3,314,004
Beds per 1000 65+
43
Population size 85+
376,706
Beds per 1000 85+
377
Source: CBS (2020a), TNO (2019, 2020). Note: figures for 2019 unless indicated otherwise.
Nursing home care is provided in nursing homes that have been adapted to the needs of their
residents. Nursing home residents typically live in one-person bedrooms. The types and amount of
care that a resident receives depend on the type of care package that the resident is eligible for.
Typically, nursing home residents receive between 11 and 29.5 hours of care and assistance per week
(Bureau HHM 2011)
7
.
To address concerns related to the quality of care in nursing homes, the government increased the
budget by 2.1 billion per year in 2017 (Bakx et al. 2020), which is approximately 10 percent of the total
budget. Organizations providing institutional care could apply for additional funding. The jump
resulting from this increase in spending appear to be clearly visible in Figure 3, though the effects on
quality-of-care have not been reported so far, likely in part because data on nursing home quality is
mostly limited to measures of the organization structure, processes, mortality, and hospitalizations
(Bakx et al. 2020; Bar et al. 2022).
Long-term care workers
Personal carers are the largest group of healthcare workers in nursing homes and in home care (Figure
9). Doctors, registered nurses, and other registered workers make up for only one-tenth of all workers
in long-term care. The number of workers in nursing homes is twice as large as in home care (CBS
2022). This reflects the higher care needs of nursing home residents compared to home care users
5
Nursing homes may be part of a larger conglomerate.
6
OECD reports beds in all types of institutional care. Nursing home users make up 59% of all institutional care
users (CBS 2022c).
7
Values for care packages 4-8. Care packages 1-3 have been phased out; package 9 is for rehabilitation and
package 10 for hospice care.

16
Classification: Internal
given that the number of home care users is three times as large as the number of nursing home
residents (cf. Part 3).
8
Many workers do not have a full-time job; the mean fulltime equivalent (FTE) per worker is 0.63 in
nursing homes and 0.55 in home care in 2021 (CBS 2022d). As a fulltime job in the long-term care
sector is 36 hours a week, this means that on average these workers work 20-23 hours per week,
which is lower than the overall mean hours worked (30 hours) reported for the Netherlands by
Eurostat (2021). This is the case for all types of workers for which data are reported (CBS 2022e).
Therefore, if expressed as the number of FTEs instead of the number of workers, the absolute number
of workers would be much lower but the split across the types of workers may not change much.
There are only formal training requirements for medical and paramedical staff for which registration
is mandatory, i.e. doctors, registered nurses and pharmacists, psychotherapists, physiotherapists,
medical psychologists. There are no formal requirements for other types of healthcare workers, yet
providers need to ensure that their workers are sufficiently qualified for the tasks that they have been
assigned and this is checked by the Healthcare Inspectorate.
Figure 9: Worker types in nursing homes and home care
Notes: 2021 estimates based on the CBS Health Care Workers Survey. The Figure contains the number of workers rather
than the fulltime equivalent (FTE). Registered medical and paramedical staff includes doctors, registered nurses and other
medical or paramedical workers for which registration is mandatory (pharmacists, psychotherapists, physiotherapists,
medical psychologists). Other paramedical and medical staff includes Including medical or paramedical staff for which
registration is not mandatory such as practical nurses and medical assistants. Source: CBS 2021a.
Table 11 shows that hourly pay for formal care workers is 23.6 euro in 2019, which was close to the
mean hourly pay in the Netherlands (23.1 euro – CBS 2021b). On average, working fulltime yields an
annual gross salary of 44 thousand euro, which is equal to the median income for all workers and close
to the average income for the seventh decile of the overall income distribution (CBS 2021c). Wages
are agreed upon at the sector level by employer’s and employee’s representatives and set in a
collective labor agreement. An employee’s wage depends on the type of job and the number of years
worked in the current job.
8
In addition to the categories listed in Figure 9, nursing homes and home care providers also have support staff,
including management and services jobs such as cleaning and cooking, and other staff. Support staff accounts
for 19%-25% (58,000 FTE in nursing homes; 34,000 FTE in home care); the other staff for 8% in nursing homes
(25,000 FTE) and 7% in home care (9,000 FTE).
0.14
0.16
0.10
0.09
0.14
0.16
0.62
0.58
0%
50%
100%
Nursing homes Home care
Registered (para)medical staff Social workers
Other (para)medical staff Personal carers

17
Classification: Internal
Table 11. Pay for full-time care workers at nursing homes and in home care.
Annual pay per FTE in
1000 euro
Hourly pay in
euro
Total
44.4
23.6
Doctors
109.9
58.5
Registered nurses
53.4
28.4
Other registered medical or paramedical workers
a
62.8
33.4
Other workers
b
42.2
22.5
2019 figures.
a
For which registration is mandatory (pharmacists, psychotherapists, physiotherapists, medical psychologists),
b
Including medical or paramedical staff for which registration is not mandatory such as logopedics, occupational therapists,
exercise therapists. Notes: All figures refer to gross payment, including overtime and other additional payments. Hourly pay
is derived from annual pay (dividing by 156,5 hour per month times 12 months). Source: CBS 2022f
Who are the caregivers
Figure 10 reports the demographic characteristics of informal caregivers (left) and formal care workers
(right). Compared to formal care workers, informal caregivers are older: the share of formal care
workers aged 35 or under (0.30) is more than twice as large than the share of informal caregivers aged
<30 (0.06) and aged 30-39 (0.08) combined. Furthermore, as in other countries (Gruber and McGarry
2023; Gørtz et al. 2023; Geyer et al. 2023), the vast majority (92%) of all formal care workers are
female, while 61% of the informal caregivers is female. Finally, informal caregivers are less likely to
have education level “middle” than formal care workers: informal care is relatively often provided by
higher educated and lower educated persons compared to formal care. 79% of all caregivers provide
care to another family member, of which roughly half to a parent and half to either a spouse or another
family member; 21% provides care to a friend, neighbor or someone else (Figure 11).
Taken together, the Dutch long-term care system is characterized by comprehensive, universal public
programs in which eligibility is based on need. Hence, formal care is accessible for all who need it.
Furthermore, user-fees make up only a few percent of total expenditures. The workforce providing
this formal care often works parttime and is predominantly female. Similarly, informal care is provided
by a specific subgroup in the population.

18
Classification: Internal
Figure 10: Demographic composition of formal care workers (left) and informal caregivers (right)
< 30, 0.06
30-39,
0.08
40-49
,
0.18
50-59,
0.31
60-69,
0.23
70+, 0.15
Informal caregivers - Age
Under 35,
0.30
35-54,
0.41
55 and
over, 0.29
Formal care workers: age
Male, 0.39
Female,
0.61
Informal caregivers - Gender
Female,
0.92
Male,
0.08
Formal care workers: gender
Low, 0.37
Middle,
0.46
High, 0.43
Missing,
0.07
Informal caregivers - Education level
Low, 0.21
Middle,
0.58
High, 0.20
Unknown,
0.02
Formal care workers: education

19
Classification: Internal
Sources: CBS 2020b, 2022g (formal care workers); own calculations based on Health Monitor data linked to administrative
registers (informal caregivers). Notes informal caregivers: the number of observations is 75,685. Education level categories
“low” and “middle 1” were merged to best mimic the data available for formal caregivers. Informal caregivers provide care
to care recipients of all ages, the data do not contain information about the age of the care recipient or the relationship
between the caregiver and the care recipient. Figures for 2016. Notes formal caregivers: weighted average of nursing home
workers and home care workers. Figures for 2021 quarter 4.
Figure 11: informal caregivers: for whom do they care
Source: own calculations based on SCP informal care survey 2019 (SCP and CBS 2020). Notes: 4,921 observations.
Respondents are interviewed about the person who they provide most care to. Parent category also includes parents in-law
and step parents. See De Klerk et al. (2021) for details on the survey data.
Part III The cost of long-term care
Private financing of long-term care is a good as absent in the Netherlands, which means that the costs
of LTC are divided between publicly financed formal care and informal care. To calculate the costs of
informal care, we apply the same approach as in the rest of this book, and use an estimate of
opportunity costs based on wages
0.83
0.07
0.10
Formal care workers: migrant
background
No migrant background
Migrant background, born in Netherlands
First generation migrant: born abroad
Spouse; 0.13
Parent; 0.41
Other family
member; 0.25
Friend, neighbor,
someone else;
0.21

20
Classification: Internal
We first report home care expenditures and nursing home care expenditures for the 65+ population.
Subsequently, we measure the value of informal care. Finally, we combine the data on formal and
informal care spending to derive estimates of total long-term care spending in the Netherlands.
Formal care costs
Table 12 reports the number of users, total spending, and average spending by user for formal home
care and nursing home care for the 65+ population by source. 211 thousand individuals in used
institutional care in 2016, which is 6.4 percent of the Dutch 65+ population. Users aged 65 and over
make up 67 percent of all institutional care users. Institutional care is fully financed by social long-
term care insurance. In total, 13.4 billion euro is spent on nursing home care for the 65+ population.
Most of this care is provided in-kind in an institutional setting which includes room and board, but
users can also opt to use care in-kind (excluding room and board) provided in a private setting or a
cash-transfer. Co-payments are income-dependent and wealth-dependent and equal 11 percent of
total spending on institutional care (Appendix A5).
About 445,000 65+ individuals use formal personal care and nursing, covered by public health
insurance. For this type of care, users do not pay any cost sharing. Total spending on personal care
and nursing is 2.8 billion euros. The rest of home care is domestic care and assistance financed by
municipalities. Around 367 thousand individuals aged 65+ use this type of care. For the services that
are person-specific, users pay a fixed monthly fee out-of-pocket, which amounts to 3 percent of the
total spending on home health services.
There are large differences in expenditures per user across countries. Total costs per nursing home
care users are 63 thousand euro in the Netherlands, which is very similar to expenditures per user in
Denmark, yet almost 50% higher than in Germany, but half as much as in the United States (Gruber
and McGarry 2023; Gørtz et al. 2023; Geyer et al. 2023). These differences may have many, potentially
partially offsetting causes, including differences in the case mix between these countries – the share
of care users who are using nursing home care varies internationally – but also in the quality of care
and other services provided, and which types of expenditures are included in these figures.
Combined expenditures on all types of home care (personal care, nursing, domestic help and
assistance) are 11 thousand euro per user in the Netherlands, which is roughly similar to expenditures
levels in Germany and Denmark and just over 50% of the expenditures per home care user in the
United States (Gruber and McGarry 2023; Gørtz et al. 2023; Geyer et al. 2023). As with nursing home
care, there may be large differences in the size and composition of the group using home care, but
also in the types of care and the level of quality that are provided.
Table 12. Formal care costs for the 65+ population
Types
Number of users
Total spending
Spending per user
(in 1000)
(in billion euro)
(in 1000 euro)
Institutional care
211
13.37
63.38
Home care – personal care and nursing
445
2.86
6.43
Home care – domestic help and assistance
367
4.10
11.17
Note: 2016 figures, expenditures adjusted to 2019 price level (CBS 2022). The total number of home care users aged 65+ is
614 thousand and hence mean spending is 11,335 euro. Source: own calculations based on administrative microdata and
CBS (2022b), CBS (2022h), CBS (2022i), CBS (2022j), RIVM (2019).
Informal care costs
We use the two approaches to estimating the opportunity costs of informal caregiving discussed in
Gruber and McGarry (2022). First, we use a counterfactual (potential) wage for each caregiver based
on the wage of individuals with the same characteristics in the general population (opportunity cost

21
Classification: Internal
method). To estimate the counterfactual wage, we regress the probability of being employed and the
estimated hourly gross wage of all employed respondents in the 2016 Public Health Monitor on age
group indicators, gender, education and household type. We then use the coefficients from these
regressions to impute the potential wage for the respondents who provided informal care. The
predicted average wage for those providing informal home care, and thus our estimate of the value
of a caregiver’s time, is 20.86 euro per hour (2019 price level).
Second, we combine the opportunity cost estimate with a market-based approach and value informal
care using the average hourly wage of home care workers (proxy good method). Not everyone who is
providing informal care would otherwise be in paid work. Specifically, many informal caregivers are
above the pension age (Figure 10). The hourly wage for formal workers who do comparable tasks as
informal caregivers was 11.70 euro on average in 2016 in the Netherlands (European Commission
2021). We use the opportunity cost method for those who work and the proxy good method for those
who do not.
To estimate the number of hours of informal care that is provided to the 65+ population, we use the
share of the 65+ sample of the 2016 Public Health Monitor who stated that they received informal
care within the last 12 months (13 percent). The average number of hours of care received per week
is based on the reported number of hours received in the last week, among those reporting currently
receiving informal care (20.5 hours).
The results are shown in Table 13. 456 million care hours per year are provided to the 65+ population
in the Netherlands. Depending on the costing method used, the estimated costs of informal caregiving
to the 65+ population are 9.51 billion euro per year (when using opportunity cost method) to 10.6
billion (when using the combined method).
Table 13. Valuation of Informal Home Care.
Opportunity
cost method
Combined: opportunity cost
and proxy good method
Valuation (billion euros)
9.51
10.65
Hours informal care received (million)
a
456
456
Predicted probability of working
0.79
0.79
Predicted wage*probability of working
20.86
20.86
Predicted wage if working
26.45
26.45
Home Health Aide Wage
11.70
Note: 2016 figures, adjusted to 2019 price level (CBS 2022).
a
Hours are per week for respondents indicating that they
currently received care. To get the number of hours, this conditional number of hours (20.5) is multiplied by the share of
respondents indicating that they received care in the past 12 months (0.13), 52 weeks and the size of the 65+ population.
Home health aide wage taken from European Commission (2021). Appendix Table B2 contains the estimate using the proxy
good method. The data do not allow us to distinguish between informal care recipients by age. In the SCP informal care
survey (SCP and CBS 2020), the probability of working is 7 percentage points lower for informal caregivers to the 65+
population than in the overall sample of caregivers. This 7-percentage point lower probability to work would translate into
a 1.8 billion euro lower (opportunity cost method) and 0.5 billion euro (combined method) lower valuation.
Total costs
Table 14 summarizes the estimates of expenditures on formal care and informal care costs to provide
a national estimate of total long-term care spending. The total costs of long-term care for the 65+
population are 31 billion euro (4 percent of GDP). The costs of informal care account for around 34
percent of total costs (1.3 percent of GDP). Despite the extensive public formal care system, informal
care costs are still substantial, both in absolute terms and as a percentage of total spending on long-
term care for the 65+ population.

22
Classification: Internal
This 34% of total spending that is attributed to informal care is lower than the 50% reported for
Germany by Geyer et al. (2022), which has traditionally relied less on formal care and more on informal
care than the Netherlands. Estimates for the United States are similar to those for the Netherlands,
while estimates of the share of informal care costs for Denmark are much lower than for the
Netherlands (Gruber and McGarry 2023; Gørtz et al. 2023). Table 13 sheds light on some of the causes
for these differences: they are not only caused by the number of informal care hours that is provided
but also by the cost estimates per hour, which may differ by as much as a factor 2.5 across these four
countries. These cost estimates per hour are in turn affected by whom provides the informal care, the
probability of working, the predicted wage if working. For instance, in the Netherlands 79 percent of
the informal caregivers works, compared to 67% in Denmark, 59% in Germany, and 48% in the United
States (Gruber and McGarry 2023; Gørtz et al. 2023; Geyer et al. 2023). Strikingly, estimates of the
hourly wage of home care workers are relatively small.
The share of formal home care costs in the total costs of long-term care are roughly equal to the share
in the US and in Germany (Gruber and McGarry 2023; Geyer et al. 2023) but lower than in Denmark
(Gørtz et al. 2023). These differences possibly reflect differences in the relative focus of the long-term
care system on nursing home care or home care as well as differences in costs per home care user and
per nursing home care user that were described above.
Table 14. Total costs by type of care, in billion euros and as a percentage of gross domestic product
(GDP)
Care type
Source
Informal care valued at opportunity
costs
Informal care valued using combination of
opportunity cost method and proxy good method
Spending in billion euros
% of GDP
Spending in billion euros
% of GDP
Nursing home
Public
11.89
1.6%
11.89
1.6%
Private
1.48
0.2%
1.48
0.2%
Total
13.37
1.8%
13.37
1.8%
Home care
Public
6.78
0.9%
6.78
0.9%
Private
0.19
0.0%
0.19
0.0%
Total
6.96
0.9%
6.96
0.9%
Informal care
Private
9.51
1.3%
10.65
1.4%
Total
Public
18.67
2.5%
18.67
2.5%
Private
11.18
1.5%
12.37
1.6%
Total
29.84
4.0%
31.03
4.1%
Notes:2016 figures, expenditures adjusted to 2019 price level (CBS 2022). Source: own calculations based on microdata and
CBS (2022b), CBS (2022h), CBS (2022i), CBS (2022j), RIVM (2019). As explained in Part 2, the number of informal caregivers
who report that they get financial compensation is very small meaning that the risk of double counting is limited.
IV Conclusions
This chapter provides an overview of long-term care use and the organization of long-term care in the
Netherlands. We have documented the distribution of well-being and need for long-term care, the
financing and organization of long-term care, the long-term care costs and how they are paid for.
We arrive at four main conclusions. First, no other country spends more per capita on publicly financed
formal care than The Netherlands, according to the System of Health Accounts of the OECD (OECD
2022). Although the Dutch definition of long-term care may be relatively broad in terms of services
and population groups included, this chapter reconfirms that the Netherlands indeed has one of the
most extensive and comprehensive public long-term care systems.
The frequent use of formal care is associated with a relatively limited reliance on informal care. The
share of informal care costs in the total costs of long-term care is lower than in some countries. When
23
Classification: Internal
considering the opportunity cost of informal care, the differences between the Netherlands and other
countries in the total costs of long-term care become much smaller (cf. European Commission 2022).
At the same time, the differences do not disappear entirely. For instance, while the share of GDP per
capita spent on formal long-term care is three times larger in the Netherlands than in the US, informal
care costs as a % of GDP are roughly twice as high in the Netherlands: 1.4% versus 0.7% (Gruber and
McGarry 2023).
Second, accounting for informal care not only has a large impact on the estimated level of long-term
care costs but also on the distribution of these costs. Formal care costs are paid for through public
programs and user payments make up for only a few percent of total revenues. Since the public
programs are funded by income-dependent premiums and general taxation, the costs of these
programs are by and large paid for according to ability to pay. By contrast, the opportunity costs of
informal care – as well as the health costs (Bom et al. 2019; Bom and Stockel 2021) – are fully borne
by informal caregivers, which is a selected and relatively small subpopulation. The findings presented
in this chapter show that the average informal caregiver provides a substantial amount of care
meaning that these opportunity costs per caregiver may be substantial too. Furthermore, the
demographic composition of the group of informal caregivers shows that some subpopulations, e.g.
middle-aged or older women, are more likely to provide informal care than others and thus take on a
greater burden, possibly despite being in a disadvantaged position for other reasons. Hence, factoring
in the costs of informal care also changes the view on the extent to which overall long-term care costs
are borne in an equitable way.
This conclusion also has implications for the consequences of future increases in long-term care use
when population ageing means that long-term care needs in the population will increase (De Meijer
et al. 2013). Will the costs of this additional care be covered through public programs that increase
expenditures when needs increase? Or by formal care users who pay greater user fees and by informal
caregivers who step in if public expenditure rises do not keep up with increases in needs? Ultimately,
how the costs of long-term care are allocated among three groups – society, users and informal
caregivers – is a political decision: to what extent is society willing, and able to continue to take an
increasing long-term care burden away from the other two groups (Bakx et al. 2020)?
Third, the threshold to receive formal care appears to be lower in the Netherlands than in other
countries. That is, the probability of formal care use is already substantial at low or moderate levels
of limitations. This is true for both home care and for nursing home care. Among the 85+ with 0-1
limitations, 44% receives formal care, of which 19% (i.e. 8% of the total population) receives nursing
home care. These individuals may have other limitations (e.g. cognitive limitations) that are not
captured by the measure that we use but that do cause a need for care. Yet, this percentage is twice
the percentage reported in the chapters for other countries that used similar measures to report
functional limitations (cf. Gruber and McGarry 2023).
Fourth, a relatively large share of formal long-term care workers in the Netherlands works parttime.
This suggests that shortages in the labor market due to the increasing demand for formal care workers
might be reduced if these workers can be persuaded to work more hours. Yet, persuading these
workers may prove to be a major challenge because of increasing competing demands, including a
rise in the demand for informal care rises. While informal care provision currently seems to have
limited impact on the labor market outcomes of caregivers (Rellstab et al. 2020), this might change
when demands for both formal and informal work increase.
Taken together, these findings highlight the importance of a complete view on long-term care use and
costs when formulating responses to the expected increase in need for long-term care in the future.
These findings are helpful in generating a better understanding of some of the trade-offs that policy
24
Classification: Internal
makers will face when deciding about the future resource allocation in long-term care. The
Netherlands is clearly on one extreme of the spectrum of policy choices, providing extensive and
collectively financed social assistance, home care, and nursing home care to its population. As a result,
care is highly accessible and the financial risks for older individuals are limited. At the same time, the
extensive collective financing of care makes Dutch public finance relatively vulnerable to the pressure
of population ageing (Wouterse & Smid, 2017). Dutch policy makers thus face the challenge of how
ensure fiscally sustainable growth of long-term care spending, which might entail limiting coverage or
increasing private spending, while at the same time preserving access to care and financial protection
for the most vulnerable groups.
References
Algemene Rekenkamer. 2018. Focus op Toegang tot de Wet langdurige zorg.
https://www.rekenkamer.nl/publicaties/rapporten/2018/06/06/focus-op-toegang-tot-de-wet-
langdurig-zorg
Bakx P, Chernichovsky D, Paolucci F, Schokkaert E, Trottman M, Wasem J, Schut FT. 2015. Demand-
side strategies to deal with moral hazard in public long-term care insurance. Journal of Health Services
Research and Policy: 170-176;
Bakx P, O’Donnell O, van Doorslaer E. 2016 Spending on health care in the Netherlands: not going so
Dutch. Fiscal Studies: 593-625;
Bakx P, Bär M, Rellstab S, Wouterse B. 2020. Zicht op kwaliteit van verpleeghuiszorg? ESHPM
Research report 2020.03
Bakx P, Schut E, Wouterse B. 2021. Price setting in long-term care in the Netherlands. World Health
Organization Kobe Center Policy Series on Long-Term Care No. 6
Bär M, Bakx P, Wouterse B, van Doorslaer E. 2022 Estimating the health value added by nursing
homes. Journal of Economic Behavior and Organization
Bom J, Bakx P, Schut FT, van Doorslaer E. 2019. Health effects of caring for and about parents and
spouses. Journal of Economics of Ageing: 100196;
Bom J, Stöckel J. 2021. Is the grass greener on the other side? The health impact of providing
informal care in the UK and the Netherlands. Social Science & Medicine 269: 113562.
Bom J, Rellstab S, Bakx P. 2022. Well-being right before and after a permanent nursing home
admission. Health Economics 31 (12): 2558-2574
Bureau HHM, 2010. Zorgzwaartepakketten Sector V&V Versie 2011.
CBS. 2020. Prognose bevolking; geslacht, leeftijd, achtergrond en generatie, 2021-2070
https://opendata.cbs.nl/statline/#/CBS/nl/dataset/84872NED/table?dl=6FAA7
CBS. 2020a. 115 duizend mensen in verzorgings- of verpleeghuis. Link
CBS. 2020b. Werknemers met een baan in de zorg en welzijn; persoonskenmerken, 2010-2019.
https://azwstatline.cbs.nl/#/AZW/nl/dataset/24025NED/table?dl=6909A&ts=1664437416075
CBS. 2021. Bevolking; geslacht, leeftijd en burgerlijke staat, 1 januari.
https://opendata.cbs.nl/statline/#/CBS/nl/dataset/7461bev/table?dl=6FAA5
25
Classification: Internal
CBS. 2021a. Werknemers; beroep, regio.
https://azwstatline.cbs.nl/#/AZW/nl/dataset/24094NED/table?dl=68FF7
CBS. 2021b. Gemiddeld uurloon van werknemers in 2019. Link
CBS. 2021c. Inkomen van personen; inkomensklassen, persoonskenmerken.
https://opendata.cbs.nl/statline/#/CBS/nl/dataset/83931NED/table?dl=697B1
CBS. 2022. Consumentenprijzen; prijsindex 2015=100.
https://opendata.cbs.nl/statline/#/CBS/nl/dataset/83131NED/table?dl=6096E
CBS. 2022a. Zorguitgaven internationaal vergelijkbaar; functies en financiering.
https://opendata.cbs.nl/statline/#/CBS/nl/dataset/84043NED/table?dl=5D7D1
CBS. 2022b. Zorguitgaven internationaal vergelijkbaar; functies en financiering.
https://opendata.cbs.nl/statline/#/CBS/nl/dataset/84043NED/table?dl=5D84A
CBS. 2022c. Gebruik bijdrageplichtige Wlz-zorg; leveringsvorm, zzp, regio.
https://mlzopendata.cbs.nl/#/MLZ/nl/dataset/40055NED/table?dl=6FB44
CBS. 2022d. Werkgelegenheid in de zorg en welzijn; baankenmerken, regio.
https://azwstatline.cbs.nl/#/AZW/nl/dataset/24017NED/table?dl=69096
CBS. 2022e. Zorg; werkgelegenheid, beroepen in zorg en welzijn, zorgaanbieders.
https://opendata.cbs.nl/statline/#/CBS/nl/dataset/83738NED/table?dl=52590
CBS. 2022f. Zorg; werkgelegenheid, beroepen in zorg en welzijn, zorgaanbieders.
https://opendata.cbs.nl/statline/#/CBS/nl/dataset/83738NED/table?dl=5DAB6
CBS. 2022g. Werknemers; scholing en vaardigheden.
https://azwstatline.cbs.nl/#/AZW/nl/dataset/24070NED/table?dl=690A1
CBS. 2022h. Gebruik bijdrageplichtige Wmo-maatwerkvoorzieningen; type, vorm, regio.
https://mlzopendata.cbs.nl/#/MLZ/nl/dataset/40060NED/table?dl=6FD0E
CBS. 2022i. Wmo en Jeugdwet; gemeentelijke baten en lasten, regio.
https://mlzopendata.cbs.nl/#/MLZ/nl/dataset/40050NED/table?dl=6EFFE
CBS. 2022j. Zvw-wijkverpleging en -behandeling; declaraties.
https://mlzopendata.cbs.nl/#/MLZ/nl/dataset/40042NED/table?dl=63CC5
CBS. 2022k. Opbouw binnenlands product (bbp); nationale rekeningen.
https://opendata.cbs.nl/statline/#/CBS/nl/dataset/84087NED/table?dl=783B6
De Klerk, M, de Boer, A, Plaisier, I. 2021. Determinants of informal care-giving in various social
relationships in the Netherlands. Health and Social Care in the Community 29: 1779– 1788.
De Meijer C, Wouterse B, Polder J, Koopmanschap M. 2013. The effect of population aging on health
expenditure growth: a critical review. European Journal of Ageing 10: 353-361

26
Classification: Internal
De Meijer C, Bakx P, Koopmanschap M, van Doorslaer E. 2015. Explaining declining rates of
institutional LTC use in the Netherlands: a decomposition approach. Health Economics 2015: S18-
S31;
Dutch Health Monitor. 2016. Public health monitor 2016 of the community health services, statistics
Netherlands and the national Institute for public health and the environment.
European Commission. 2021. Study on exploring the incidence and costs of informal long-term care
in the EU. Link
Eurostat. 2022. Average number of usual weekly hours of work in main job, by sex, age, professional
status, full-time/part-time and economic activity (from 2008 onwards, NACE Rev. 2). Link
Geyer J, Börsch-Supan A, Haan P, Perdrix E. 2022. Long-term care in Germany. NBER book chapter
forthcoming
Gørtz M, Christensen B, Datta Gupta N. 2022. Long-term care in Denmark. NBER book chapter
forthcoming
Gruber J, McGarry K, 2022. Long-term care in the United States. NBER book chapter forthcoming
Hussem A, Bakx P, Tenand M. 2020. Publieke middelen voor particuliere ouderenzorg. Netspar
Design Paper 143
OECD. 2021. Pensions at a Glance 2021: OECD and G20 Indicators. Link
OECD. 2022. Stats.oecd.org
NZa. 2019. Monitor contractering wijkverpleging 2019. Link
Rellstab S, Bakx P, García-Gómez P, van Doorslaer E. 2020. The kids are alright. Labour market effects
of a parental health shock: evidence from the Netherlands. Journal of Health Economics: 102275;
RIVM. 2019. Kosten van ziekten 2017.
https://statline.rivm.nl/#/RIVM/nl/dataset/50050NED/table?dl=6FD13
SCP. 2015. Informele hulp: wie doet wat? The Hague: SCP
SCP. 2019. Wonen met zorg. Verkenning van particuliere woonzorg voor ouderen met zorg. The
Hague: SCP
SCP and CBS. 2020. Informele Zorg - IZG 2019. DANS. https://doi.org/10.17026/dans-xzy-69n3
Tenand M, Bakx P, van Doorslaer E. 2020. Eligibility or use? Disentangling the sources of horizontal
inequity in home care receipt in the Netherlands. Health Economics: 1161-1179
Tenand M, Bakx P, van Doorslaer E. 2020a. Equal long-term care for equal needs with universal and
comprehensive coverage? An assessment using Dutch administrative data. Health Economics: 435-
451;
TNO. 2019. Prognose capaciteitsontwikkeling verpleeghuiszorg. Link

27
Classification: Internal
TNO. 2020. Prognose capaciteitsontwikkeling verpleeghuiszorg fase II. Link
Wo
uterse B, Smid B. 2017. How to finance the rising costs of long
-te
rm care: Four alternatives for
the Netherlands. Fiscal Studies: 369-391.
Wo
uterse B, Hussem A, Wong A. 2022. The risk protection and redistribution effects of long
-term
care co-payments. Journal of Risk and Insurance: 161-186.
Zorgverzekeraars Nederland. 2022. Landelijke rapportage wachtlijsten Verpleging & Verzorging (Wlz)
4e kwartaal 2021. Link

28
Classification: Internal
Appendix
Appendix A: Data
Table A1 Linked administrative registers and survey data
Data source
Short description
Municipal registry
Address, demographics: age, gender
Central Administration Office Long-term care
Nursing home care use, co-payments, home care paid for through Social
Support Act
Health survey
Functional limitations
Public Health Monitor
Functional limitations, informal care, employment information
Tax office
Tax office data: income, household wealth
Health insurance claims
Expenditures on nursing and personal care
Tables A2-A3 reports the relation between limitations measured on the OECD and ADL scales. We use
the Public Health Survey 2016, which includes both scales. We record the percentage of the 65+
respondents who reports having IADLs and no ADLs, at most 1 ADL, at most 2 ADL, etc., by the number
of OECD limitations reported. We use the smallest number of OECD limitations for which the share of
reporting a particular number of ADLS is more than 50 percent as the cut-offs for our mapping from
OECD limitations to ADLs in this chapter. Table A3 shows the mapping that is used for Table 5; Table
A2 for all other tables and figures that contain information on functional limitations
Table A2 comparison OECD- IADL/ADL limitation scales: ADL and IADL separate
≤ 1 IADL
≤ 1 ADL
≤ 2 ADL
≤ 3 ADL
≤ 4 ADL
≤ 5 ADL
Observations
0 OECD
.100
.040
*
*
*
*
942
1 OECD
.304
.178
.046
*
*
*
415
2 OECD
.541
.325
.192
.082
*
*
255
3 OECD
.746
.583
.408
.317
.208
.117
240
4 OECD
.848
.696
.518
.357
.241
.143
112
5 OECD
*
.821
.714
.607
.488
.321
84
6 OECD
*
*
*
.588
.500
.353
34
Note: * means fewer than 10 observations or more than the total minus 10.
Table A3 comparison OECD-IADL/ADL limitation scales: ADL and IADL combined
Combined number of ADL and IADL
≤ 1
≤ 2
≤ 3
≤ 4
≤ 5
≤ 6
Observations
0 OECD
0.243
0.059
0.018
*
*
*
942
1 OECD
0.561
0.246
0.113
0.055
0.027
0.007
415
2 OECD
0.820
0.510
0.310
0.220
0.145
0.075
255
3 OECD
0.904
0.725
0.600
0.483
0.363
0.296
240
4 OECD
0.955
0.830
0.714
0.598
0.527
0.420
112
5 OECD
*
*
*
0.821
0.750
0.667
84
6 OECD
*
*
*
*
*
*
34
Note: * means fewer than 10 observations or more than the total minus 10. Shares not reported for 7-13 ADLs/IADLs.

29
Classification: Internal
Appendix B: Additional results
Table B1 Demographic composition of formal home care workers.
Nursing homes
Home care
Gender
Male
.09
.07
Female
.91
.93
Age
Under 35
.32
.27
35-54
.40
.43
55 and over
.28
.30
Migrant background
No migrant background
.83
.83
Migrant background
.17
.17
First generation migrant: born abroad
.10
.10
Education level
Low
.21
.20
Middle
.60
.54
High
.19
.21
Unknown
.01
.05
Number of workers (in 1000s)
282.6
148.6
Source: CBS 2022a, 2022b. Note: figures for 2021 quarter 4.
Table B2: Valuation of informal care using the proxy good (market wage) method
Valuation (billion euros)
5.33
Hours informal care received (million)
456
Home Health Aide Wage
11.70
Note: 2016 figures, adjusted to 2019 price level (CBS 2022). Number of hours. Hours are per week for respondents indicating
that they currently received care. This conditional number of hours (20.5) is multiplied by the share of respondents indicating
that they received care in the past 12 months (0.13), 52 weeks and the size of the 65+ population. Home health aide wage
taken from European Commission (2021).
Figure B1: Formal care expenditures, 65+ population
41%
56%
3%
Home care
Health insurance (ZVW, Personal care and nursing)
Muncipalities (WMO, Domestic help and assistance)
Co-payments (WMO, Domestic help and assistance)

30
Classification: Internal
Source: own calculations based on administrative microdata and CBS (2022b), CBS (2022h), CBS (2022i), CBS (2022j), RIVM
(2019).
89%
11%
Nursing home
Social insurance (WLZ) Co-payments (WLZ)
