
The Economics of Long-Term Care in Canada
Kevin Milligan, University of British Columbia and NBER
Tammy Schirle, Wilfrid Laurier University
July 2023
This paper is written for the NBER international comparison project on long-term care. We
thank the organizers and other participants in the project for helpful suggestions, and
Moyosoreoluwa Sogaolu for research assistance. Some of the research was conducted at the
SWORD Research Data Centre under contract 21-MAPA-SWO-7104. Statistics Canada is not
responsible for the results presented in this paper.
1
Introduction
The Covid-19 pandemic brought the current state of long-term care into broad public focus as
many people in Canada and other countries wondered about the available quality of care. Going
forward, these concerns about the quality of long-term care will grow more acute by the aging of
the population. The first Canadians born in the baby-boom generation are now approaching their
80s, an age range where the use of long-term care grows rapidly. So, with increased demand for
higher-quality care and an increase in the demographic demand for care, the pressures on the
long-term care sector are set to increase.
This paper contributes a broad overview of the Canadian long-term care system. Taking an
economist’s viewpoint, we bring together supply and demand factors to provide an economic
analysis of the current and future path for long-term care. Canada’s situation shares similarities
with other countries, but also embodies unique structural characteristics.
The two key similarities of the Canadian situation with most other OECD countries are the
demographic pressures and the focus on residential care. Because of the aging of the baby boom
population the share of Canadians over age 65 will more than double from 11 percent of the
population in 1990 to a forecast of 24 percent in 2050. For those over age 85, the population
share is projected to go from 1 percent in 1990 to over 5 percent by 2050. These trends are
broadly aligned with other OECD countries. The other main similarity is the focus of the system
on residential care. While there has been increasing attention paid to home and community non-
residential care, the majority of public expenditures still go to residential care in nursing homes.
2
The main difference of the Canadian case with other OECD countries is the mix of public and
private care. There is large variance across countries in the public share of long-term care
spending, and Canada is overall in the middle of the pack. The Canadian private long-term care
insurance market is small; and shrinking further in recent years. The biggest difference from
other countries is the dispersion of the public-private mix within Canada, as other countries have
more uniform country-wide systems. Long-term care in Canada is regulated provincially and the
public systems are designed and funded provincially. The result is that different provinces have
very different systems. Quebec’s long-term care is largely in a unified public system, while New
Brunswick’s system is dominated by private not-for-profits and Ontario’s has a majority of
private for-profit facilities.
The analysis below aims to provide an introduction to and overview of the economics of long-
term care in Canada in the context of international comparison. We are somewhat constrained in
this comparison by lack of a large survey like the Health and Retirement Study in the United
States, or the SHARE data in many European countries. For this reason, we lack data on some
key metrics used to compare across countries, such as standardized measures of activities of
daily living. In addition, there is not one national system to describe but instead a plethora of
subnational systems, each with its own administrative information and design features.
The paper begins with background information on the demographics, wellbeing, health and
living arrangements of Canadian seniors. We then provide information on caregiving, focusing
both on the receivers and givers of care in institutional settings, as well as formal and informal
home-based settings. We then describe the structure of the long-term care system in Canada,

3
including public and private components. Finally, we offer calculations estimating the total cost
of long-term care of the elderly in Canada, including implicit costs for informal home care.
Part I: Demographics, Well-Being, Health, and Living Arrangements
This section provides background context to the discussion of caregiving for Canadian seniors.
We begin with statistics on demographic trends. We then provide an overview of the health of
Canadian seniors, their economic wellbeing, and their living arrangements.
I.A. Demographic facts and trends
The Canadian population is aging and is expected to age further over the next few decades. The
figures discussed in this section illustrate this trend. For women, life expectancy at birth (Figure
1) increased from 80.6 years in 1990 to 84.3 years in 2019. Our projections suggest women’s life
expectancy will increase further, reaching 87 years by 2050.
1
For men, life expectancy at birth
was 74.3 years in 1990, increasing to 80.2 by 2019 and expected to increase to 84.7 by 2050.
Life expectancy at age 65 shows similar trends (in Figure 2). In 1990, women aged 65 could
expect to live an additional 19.4 years and are project to see that increase to 24 years by 2050.
Men have seen greater improvements in old-age mortality, as men in 1990s expected to live
another 15.4 years after age 65, while men are projected to live another 22.2 years after age 65 in
the year 2050.
1
We use a simple Lee-Carter method for projecting mortality rates, estimating Canada-wide mortality separately for
men and women, using single-age mortality rates from 1981-2019 to form projections. We made use of the leecarter
command in Stata in developing these estimates, and the general time trend component is projected as a random
walk with drift process (using ARIMA in Stata). Projections are sensitive to the time period used in estimates and
these projections appear to underestimate life expectancy. See Bohnert et al. (2015) for information on the methods
used by Statistics Canada, which are more involved than what is used here.

4
Figure 1: Life Expectancy at Birth
Source: Authors’ tabulations using Canadian Human Mortality Database (2022) mortality rates.
Our projections based on Lee-Carter methods.
Overall, these projections indicate a large and sustained increase in lifespans, on average. In
Milligan and Schirle (2021) these average lifespan changes are disaggregated by splitting people
into quantile groups using earnings from ages 50-54. That paper finds that longevity is greater
for high earners than low earners, but that the gains in longevity over time have been almost
uniform across the earnings distribution.

5
Figure 2: Life Expectancy at Age 65
Source: Authors’ tabulations using Canadian Human Mortality Database (2022) mortality rates.
Our projections are based on Lee-Carter methods.
Alongside general reductions in fertility rates in Canada, the increase in life expectancy is a key
reason why older individuals now represent a larger share of the population. The share of the
population that is over the age of 65 (shown in Figure 3) rose from 11 percent in 1990 to nearly
18 percent in 2019. The trend is expected to slow after 2030 as the Baby Boom generation ages,
with the share age 65 and over reaching 24 percent by 2050.

6
Figure 3: Population over Age 65
Source: Authors’ tabulations based on Statistics Canada Tables 1700005 and 1700057.
For the population share age 85 or older, the Baby Boom generation again dominates the trends.
In Figure 4, the rapid increase in the population age 85 and older begins around 2030, 85 years
after the war’s end in 1945. The 85 and older population share will go from about 1 percent in
1990 to almost 6 percent by 2050. Correspondingly, those over 85 represent an increasingly
larger share of the older population after 2030 (Figure 5). So, the elderly population will grow to
have a much heavier share of the oldest old. These demographic trends underlie projections for
the increase and timing of an upswing in the demand for long-term care in the coming decades.

7
Figure 4: Population over Age 85
Source: Authors’ tabulations based on Statistics Canada Tables 1700005 and 1700057.

8
Figure 5: Share of Age 65+ population age 85+
Source: Authors’ tabulations based on Statistics Canada Tables 1700005 and 1700057.
I.B. Health measures
In Canada, we do not have the standard Activities of Daily Life (ADL) measure available in the
datasets we use for this paper. Instead, we focus on questions that report whether the respondent
needs “help” with an activity. Needing help is potentially a distinct concept from having a
limitation. When comparing our results to other countries, this difference should be kept in mind.
From pooling years in the Canadian Community Health Survey for those living in private homes,
we find that 22 percent of the population aged 65 or older, and 59 percent of the population aged

9
85 or older, report requiring help with at least one daily activity due to a long-term health
condition or aging.
2
In Table 1 we present both the types of help needed and the count for the
number of items with which help is needed, for the 65 and older and 85 and older populations.
Table 1: Proportion of Older Population Needing Help with Activity
Activity
65+
85+
Total
65+
85+
Meals
0.080
0.261
0
0.777
0.408
Errands
0.156
0.481
1
0.086
0.159
Housework
0.157
0.423
2
0.046
0.119
Finances
0.083
0.291
3
0.033
0.107
Basic
4
0.021
0.070
Personal care
0.057
0.201
5
0.019
0.075
Moving
0.033
0.093
6
0.019
0.063
Note: Canadian Community Health Survey master file tabulations, years 2009, 2010, 2013 and
2014. Individuals report whether they require help with each activity. Total indicates how many
of these activities an individual has reported needing help with.
It appears common for people to need support with tasks required for independent living (as 48
percent of seniors aged 85 or over need help running errands). However, a significant portion
also requires help with basic activities of daily living: 6 percent of those 65 and older, and 20
percent of those 85 and older, required help with personal care (which includes washing,
dressing, eating, or taking medications). The increase in need between the 65 and older and 85
and older population is striking. For many categories in Table 1 the need increases by a factor of
more than three between the two age categories. This finding emphasizes the very steep gradient
of need for help with the activities of life as Canadians age.
2
This number can be inferred from Table 4; by taking one minus the proportion needing help with zero activities in
the right-hand panel.
10
The greater need for help with daily activities seen above reflects a general deterioration in
health. In Table 2, we see older individuals are less likely to report good (or better) health than
younger individuals aged 18-64. Among older individuals, however, there is a large gap between
those who report needing help with personal care and the general elderly population. For
example, while 77 percent those 65 and older report good health, only 36 percent of those 65 and
older who require help with personal care also report good health. Those requiring personal care
are also less likely to report good mental health, although the gap between them and the general
population is not as large (81 percent vs. 94 percent among those 65 and older). Life satisfaction,
however, appears to decline with age and is quite low among those requiring help with personal
care. For those aged 65 and older who require help, 42 percent are satisfied with life. For ages 85
and older, this proportion drops slightly to 37 percent.
Table 2: Health and Wellbeing of Individuals
18-64
65+
85+
All
All
Personal
care
All
Personal
care
Good health
0.904
0.773
0.364
0.666
0.419
Good mental
health
0.940
0.944
0.810
0.916
0.831
Satisfied
0.908
0.820
0.419
0.651
0.372
Note: Canadian Community Health Survey master file tabulations, years 2009, 2010, 2013 and
2014. Personal care refers to anyone who reports needing help with personal care needs due to a
long-term health condition or aging. Good health indicates good, very good or excellent self-
reported health. Satisfied indicates that on a scale of 1 to 10 the respondent rates satisfaction with
life as 6 or higher.
In Table 3, we describe the income position of seniors who require help with personal care or
housework. We split the population of seniors by their position relative to the median income,
where the median income line is drawn using the incomes of all families with main income

11
earner age 18 and older. From our tabulations here, we find nearly 30 percent of people aged 65
and over have a household income that is less than half the median income of the broader
population. When restricted to the subset of seniors requiring help with personal care or
housework, there are fewer seniors in the middle-income groups, and more in the lowest income
groups. Among those needing help with personal care, 36.4 percent have less than half the
median income, a higher share than for the full age 65 and older population.
Table 3: Distribution of Household Income
No Personal Care
All 65+
Personal care
Housework
No
Housework
<50% median
0.295
0.364
.334
.285
50-100% median
0.305
0.256
.293
.310
100-150% median
0.122
0.096
.097
.128
150-200% median
0.045
0.027
.032
.048
200% + median
0.232
0.258
.241
.229
Note: Canadian Community Health Survey master file tabulations, years 2009, 2010, 2013 and
2014. Household income (normalized for family size) is compared to the median (normalized)
household income for respondents age 18 and over. The second column restricts the sample to
those reporting need for help with personal care.
I.C. Economic Well-being
We now describe the financial situation of Canadian seniors as context to the affordability of
care among older Canadians. The surveys we use here for assessing the economic well-being of
Canadians exclude from the sampling frame those who live in congregate living facilities. So, the
results are representative only for those who live in private dwellings. We return to this
discussion when assessing living arrangements below.
In Table 4, we report the income distribution of older families (age 65 and over) relative to the
income distribution of younger families (aged 18-64). To account for differences between the
12
two groups in terms of average family size, the lower panel (B) in Table 4 offers estimates based
on normalized income. When considering the incomes of those 65 and older to those age 18-64,
the high ratio at the 5
th
percentile of each distribution clearly stands out: the 5
th
percentile of
after-tax normalized income among older families and individuals is 1.65 times the income of
younger families. This largely reflects the relative generosity of Canada’s retirement income
system to the supports available to the non-elderly at the lowest part of the income distribution
(where child benefits are relatively generous but minimal supports are available to childless non-
elderly families).
For middle- and higher-income seniors, the numbers reported in Table 4 suggest seniors have
incomes that are lower than among younger families. Seniors at the 75
th
percentile of the
normalized after-tax income distribution have incomes that are 85 percent of the incomes of
younger families at the 75
th
percentile. It is worth noting the ratio of normalized before tax
incomes among seniors to younger families is magnitude similar to the earnings replacement
rates of retired couples in the upper half of the income distribution described in Ostrovsky and
Schellenberg (2010). The overall picture that emerges is a more compressed income distribution
for seniors than for younger Canadians. This finding is consistent with more detailed (but earlier)
research in Baker and Milligan (2009).

13
Table 4: Income Distribution
After-tax income
Before-tax income
18-64
65+
Ratio
18-64
65+
Ratio
A. Total
5th
14319
20696
1.45
14477
20798
1.44
10th
23703
21970
0.93
24544
22046
0.90
25th
45857
31834
0.69
50286
32649
0.65
50th
79016
48431
0.61
90786
51612
0.57
75th
121350
73490
0.61
145787
82655
0.57
90th
169658
104498
0.62
209811
124480
0.59
95th
208547
132187
0.63
265705
162991
0.61
Mean
91302
59293
0.65
109814
67660
0.62
B. Normalized
5th
11291
18606
1.65
11469
18831
1.64
10th
15901
20330
1.28
16162
20492
1.27
25th
25332
23313
0.92
27118
23478
0.87
50th
38501
32246
0.84
44220
34378
0.78
75th
54592
46254
0.85
65898
53058
0.81
90th
74224
64024
0.86
92750
77481
0.84
95th
90160
79196
0.88
116184
98814
0.85
Mean
43151
39081
0.91
51844
44552
0.86
Note: Incomes presented in 2019 Canadian dollars, using the 2018 Canadian Income Survey,
representing income of a census family, authors’ tabulations. For the bottom panel, income is
‘normalized’ using the OECD equivalence scale to account for the number and age of census
family members.
As older individuals may use their assets to finance consumption in retirement, we also consider
the wealth available to older and younger families (in Table 5). We categorize families by the
age of the major income earner within the family. At the 10
th
percentile, the net worth of seniors
is more than 8 times that of younger families (18-64). At the median, however, this ratio falls to
just over two. Both groups’ distributions are highly skewed, with seniors at the 95
th
percentile
holding 1.18 times the assets of younger families at the 95
th
percentile (worth 1.8 million in 2019
for younger families and 2.1 million for senior families).

14
Table 5: Wealth Distribution
Percentile
18-64
65+
Ratio
10th
1075
9000
8.37
25th
25950
103075
3.97
50th
192000
385000
2.01
75th
573350
850000
1.48
90th
1177005
1551050
1.32
95th
1812505
2147500
1.18
Mean
445891
642207
1.44
Note: Canadian dollars, 2019, Survey of Financial Security. Net worth of an economic family
excluding employer pensions.
Tables 4 and 5 then suggest the flow of income may be most important for judging the financial
well-being of lower-income seniors while net worth is more important for seniors in the middle
or upper end of the distribution. In Table 6 we consider the distribution of consumption
expenditures more directly. Across the distributions, the ratio of expenditures among seniors is
lower than among younger households. The normalized income estimates are important to
highlight—consumption at the lowest end of the distribution is nearly identical among seniors
(65+) and younger households (18-64), with a ratio of 0.91 at the 5
th
percentile.
Note the middle of these normalized expenditure distributions is where there appears the greatest
difference (0.80), however this is much larger a ratio than what was observed in Table 4 with
respect to income measures. This suggests that consumption of seniors is less different than
younger families than income. The difference is explained by more seniors having the ability to
draw down savings to fund current expenditures. These differences in younger and older family
consumption patterns are explored in detail in Milligan (2008).

15
Table 6: Consumption Distribution
A. Total
B. Normalized
18-64
65+
Ratio
18-64
65+
Ratio
5th
13186
10432
0.79
8929
8159
0.91
10th
17941
12477
0.70
11418
9733
0.85
25th
28021
17889
0.64
16122
12860
0.80
50th
45051
28298
0.63
23644
18834
0.80
75th
68289
45776
0.67
34970
28316
0.81
90th
96514
68738
0.71
49690
41673
0.84
95th
121288
87047
0.72
62922
53115
0.84
Mean
53002
35925
0.68
28192
23084
0.82
Note: Canadian 2019 dollars, using the 2017 Survey of Household Spending. Total consumption
of a household is presented here. Normalized amount adjusts household spending to account for
the number of household members and whether members are adults or children using available
information about household size and type and the OECD equivalence scales.
I.D. Living Arrangements
The well-being of individuals also depends on their living arrangements. Living with others is an
important determinant of opportunities to share income or receive care from family or friends.
In Table 7 we provide counts of Canadians in 2021 by the type of dwelling they lived in. The
vast majority of Canadians aged 65 or older (94 percent) live in private dwellings (whether
owned or rented). The remaining 6 percent of Canadians aged 65 or older live in ‘collective’
dwellings, which for the most part are the long-term care facilities—nursing homes and seniors’
residences—that provide care. A larger portion of those aged 85 and older (27 percent) live in
these collective dwellings. Later in the paper (in Part II.B) we return to discussing the situation
of seniors in long-term care facilities.

16
Table 7: Dwelling Type by Age Group, 2021
All ages
Age 65+
Age 85+
(1000s)
(%)
(1000s)
(%)
(1000s)
(%)
All
36986
100%
7021
100%
861
100%
Private dwellings:
Single detached
21496
58.12%
3948
56.23%
322
37.39%
Other
14832
40.10%
2639
37.58%
301
35.00%
Collective dwellings:
Health care facility
485
1.31%
408
5.82%
233
27.07%
Hospitals
11
0.03%
8
0.11%
4
0.44%
Nursing homes
185
0.50%
172
2.45%
100
11.62%
Seniors residence
160
0.43%
151
2.15%
89
10.33%
Nursing+res.
68
0.18%
65
0.92%
38
4.46%
Other
234
0.63%
39
0.56%
7
0.76%
Source: tabulations based on 2021 Census tables 98100046 and 98100045.
As mentioned earlier, survey-based data on income, consumption, and wealth are limited by the
sampling frame which includes only those in private dwellings. This means that for the older (85
and older) population, the 27 percent in nursing homes and seniors’ residences are not included
in those data.
The types of family Canadians live in changes over the lifecycle. In Figure 6 we consider the
living arrangements of individuals in private dwellings in 2016 using the Census. The figure
describes the likelihood of couples or single individuals to live independently (without others).
We see that at ages 65-74 and over age 75, most people are living independently (82 and 81
percent, respectively). A small share has older family members in their household (6 percent and
7 percent respectively) but are less likely than younger individuals to have older family living
with them. A slightly larger share of seniors over 65 are the oldest members of their household,
with younger family present (11 percent).

17
Figure 6: Living Arrangements of Individuals in Private Dwellings
In order to understand how living arrangements vary by health status, we turn back to a pooled
sample from the Canadian Community Health Survey. Tabulations presented in Table 8 indicate
that the seniors living with younger members may be able to rely on those younger members for
some care. The seniors (65 and older) needing help with personal care appear more likely to live
with one of their children (13 percent) than the broader sample of seniors (8.5 percent). Those
needing care are also slightly less likely to live alone.

18
Table 8: Living Arrangements of Older Individuals in Private Dwellings
65+
85+
All
Personal
care
All
Personal
care
Living arrangements
With spouse
0.587
0.447
0.313
0.260
With child
0.085
0.130
0.118
0.164
Alone
0.286
0.264
0.469
0.317
other
0.092
0.199
0.124
0.274
Homeowner
0.779
0.692
0.654
0.655
Note: Canadian Community Health Survey master file tabulations, years 2009, 2010, 2013 and
2014. Personal care refers to anyone who reports needing help with personal care needs due to a
long-term health condition or aging.
The analysis in this section shows that contemporary Canadian seniors are, overall, in a solid
economic situation with higher wealth and less low-income incidence than younger Canadians.
Most live in a home they own with their spouse. However, when looking at the age 85 and older
compared to the age 65 and older group, more live with their child or alone and fewer live in
their own house. These patterns are driven in part by deteriorating health at older ages, with
incidence of the need for help more than triple in the 85 and older population what is seen in the
age 65 and older population. Because the age 85 and older population is set to grow
substantially, the patterns among the older seniors we document in this section should attract
particular attention by policy makers.
Part II: Receipt and Provision of Care
After the broad overview of the demographic and economic situation of Canadian seniors in the
previous section, we now turn to the use and provision of care for Canadian seniors. We begin
with the receipt of care, looking at how institutional residential care and home-based care is
19
provided. We then focus on the labor market for caregivers, with analysis of the number of
workers and their wages.
II. A. Receipt of Care
In Canada, the vast majority of individuals over age 65 live in private dwellings—either
independently or with extended family, as described earlier in part I.D. As individuals age and
require more care, they are more likely to rely on institutional care—in nursing homes,
residential care facilities or facilities that combine the two (see Table 7 in the previous section).
In this section, we describe the extent to which elderly Canadians are receiving care in each
setting and the types of care they receive.
Institutional care
In 2021, there were 408 thousand individuals aged 65 or older living in seniors’ homes, nursing
homes, and health care facilities according to the Census. (See Table 7 in the previous section).
According to an institutional accounting provided by the Canadian Institute for Health
Information that we analyze in this section, the number of formal long-term care beds is just
under 200,000. This is consistent with the Census count if one considers that many of those who
identify as living in a “seniors’ home” may live in a facility that does not meet the technical
definition for a “long-term care bed.”

20
Table 9: Number of Beds and Facilities
Beds
Facilities
Jurisdiction
Number
of LTC
beds
Beds per
1000
persons
age 65+
Number
of LTC
homes
Share
Public
Share
private /
for profit
Share
private
/ NFP
Newfoundland and
Labrador
3014
26
40
98%
2%
0%
Prince Edward Island
1244
39
19
47%
47%
6%
Nova Scotia
6842
33
84
14%
44%
42%
New Brunswick
4925
29
70
0%
14%
86%
Quebec
40823
24
440
88%
12%
0%
Ontario
78902
30
627
16%
57%
27%
Manitoba
9765
44
125
57%
14%
29%
Saskatchewan
8924
47
161
74%
5%
21%
Alberta
15762
26
186
46%
27%
27%
British Columbia
27478
28
308
35%
37%
28%
Yukon
312
56
4
100%
0%
0%
Northwest Territories
201
51
9
100%
0%
0%
Nunavut
28
18
3
100%
0%
0%
Canada total
198220
29
2076
46%
31%
23%
Source: National Health Expenditure Database, Canadian Institute for Health Information, 2021.
The Canadian Institute for Health Information assembles the National Health Expenditure
Database, part of which focuses on long-term care. The database is assembled from the national
income and product accounts, provincial administrative records, and a number of different
surveys.
3
We use these data to report the overall counts of beds and facilities, along with the
breakdown by who owns the facility – publicly owned, owned by private for-profit organizations
or owned by private not-for-profit organizations.
3
See Canadian Institute for Health Information (2021). See also Grignon and Spencer (2018) for refinements and
criticisms of the measures used in the database.
21
The first column of Table 9 shows the number of beds in each province and territory, and the
second column normalizes the beds by the population age 65 and older. There is a large spread in
the number of beds per capita, ranging from 18 per 1,000 in Nunavut Territory to 56 per 1,000 in
Yukon Territory. The patterns defy easy description, with different mixes of political culture,
rural-urban differences, and incomes being contributing factors.
The right-hand panel of Table 9 shows facilities counts and how they break down into the share
owned by public, private for-profit, and private not-for-profit organizations. There is a wide
range. The systems in the territories are fully public, and Quebec is almost fully public. On the
other end, New Brunswick has no publicly owned homes, but an 86 percent share for private not-
for-profit. Ontario has the largest for-profit share, at 57 percent. British Columbia has an even
mix of the three types.
The main explanation for this cross-provincial difference is the constitutional assignment of
responsibilities to federal and provincial governments. Long-term care facilities are regulated
provincially. As long-term care facilities-based care is not publicly insured as part of federal-
provincial agreements, standards of care and staffing are set by provincial governments under
provincial statutes and regulations. For example, Ontario’s (recently rewritten) legislation is
called the “Fixing Long-Term Care Homes Act, 2021” (Statutes of Ontario Chapter 39). To be
granted a licence, there must be an infection prevention and control program, a policy to prevent
abuse and neglect, and a procedure for reporting and complaints, among other rules. For staffing,
the regulations require that personal support workers complete a program that meets established

22
standards, including 600 hours of class time and practical time. Other provinces have similar
types of legislation and regulations, but the scope and level of regulation varies across provinces.
Non-institutional care
In 2021, there were 6.6 million Canadians aged 65 or older living outside of institutions, often
independently but also in private homes with other family members. (See Table 7 and Figure 6 in
the previous section.) A substantial portion of this group requires help with personal care and
other daily activities in their own homes.
Figure 7: Older Individuals Receiving Help, Paid and Unpaid
Source: GSS Cycles 32 (2018) and 26 (2012) tabulations by authors. Respondents are asked
about the hours of care or help received in an average week.
In Figure 7 we describe how often older individuals (65 or older and 85 or older) indicate
receiving help, and whether they paid for the help they received. Among those aged 85 or older,

23
56 percent did not receive any care or help. Only 3 percent relied exclusively on paid help, 16
percent relied exclusively on unpaid help, and a larger group (25 percent) relied on both paid and
unpaid help.
Table 10: Hours of Care Received by Older Individuals
65+
85+
Unpaid
Paid
Unpaid
Paid
Average
22
8
26
13
25th percentile
2
1
3
1
Median
7
2
10
3
75th percentile
21
6
24
8
Source: GSS Cycles 32 (2018) and 26 (2012) tabulations by authors. Respondents are asked
about the hours of care or help received in an average week.
We can also examine the intensity of care by looking at the number of hours of care received.
Table 10 reports the distribution of hours of care received of both unpaid and paid types. There is
stronger reliance on unpaid care than paid care. Comparing the medians to the means, it appears
the distribution of hours is highly skewed. The mean of unpaid hours at age 65 and older, for
example, is 22 hours but the median is only 7 hours and the 75
th
percentile only reaches 21
hours. The average number of hours rises with age, but only by 30 percent on average across the
two age groups shown. This contrasts with the extensive margin (any care being received) in
Figure 7 which showed the proportion using any care at all more than doubled from ages 65 and
older to ages 85 and older. So while there are age gradients in both the intensive margin (Table
10) and the extensive margin (Figure 7), it is the extensive margin that shows the stronger age
gradient as more seniors find they need at least some care at older ages.

24
Reliance on paid home care services
In Table 11 we provide further information on the types of home care services individuals
receive. (We note that Figure 7 and Table 11 are based on different sources and that the former
suggests only a slightly different percentage of seniors relying on paid care.) Among the services
people pay for, it is most common for the elderly to require nursing care (11 percent of those age
85 or over) and personal or home support (23 percent of those age 85 or over). Both of these
categories also exhibit very strong growth from the younger (age 65 and older) to the older (age
85 and older) groups.
Table 11: Use of Paid Home Care Services, by Type of Service
Portion who report use
Type of home care used
65+
85+
Nursing care
0.038
0.114
Other health care
0.015
0.038
Medical equipment and
supplies
0.019
0.050
Personal or home support
0.055
0.234
Other services
0.013
0.051
Any Care
0.092
0.313
Source: CCHS tabulations, years 2015, 2016, 2018, 2019.
In Table 12, we describe the length of time people over age 65 have used different types of home
care services. It appears most types of home supports reflect a need for longer-term care: 42
percent of those using nursing care have been receiving help for more than one year and 67
percent of those receiving personal and home supports have received the help for more than one
year. Reliance on other health care services appears a bit more short-term, which includes
services such as physiotherapy. This pattern of shorter-term care may arise from recovery from
specific acute health events like a broken bone or a heart attack.

25
Table 12: Duration of Home Care Services Used, by Type of Service (Age 65+)
Duration of Care
Nursing
Other health
Med.
Equip
Support
Other
Less than 1 month
0.203
0.233
0.125
0.076
0.115
1-less than 3 months
0.152
0.199
0.167
0.076
0.094
3-less than 6 months
0.089
0.098
0.118
0.067
0.078
6 months - less than 1 year
0.135
0.141
0.114
0.110
0.133
1-3 years
0.220
0.168
0.224
0.311
0.285
More than 3 years
0.202
0.161
0.252
0.361
0.296
Source: CCHS tabulations, years 2015, 2016, 2018, 2019. Each column sums to 1.
When home care services are paid, it is not necessarily the care recipients paying for these
services directly. Similar to long-term care facilities-based care, home care services are not
publicly insured as part of federal-provincial agreements. As such, the standards for assessing
home care needs and the out-of-pocket costs to recipients vary by province. For example, in
Quebec a needs assessment determines whether individuals qualify for home care services (such
as nursing or personal support) and if approved there is no payment required by individuals. For
domestic help services (such as housekeeping) in Quebec, those needing assistance can receive a
subsidy (up to $18.65 per hour) depending on age, income, and family situation. In British
Columbia, a needs assessment also determines eligibility for home care services but payment for
services depends on income. BC individuals with low income (eg. such as those receiving the
Guaranteed Income Supplement) are not required to pay anything, but those with a modest
income will be charged up to $300 per month for support.
4
Overall, a large part of home care services is paid for by provincial governments (as discussed in
more detail in the next section). In Table 13 we see that most people receiving nursing care
services did not typically pay anything at all (as 87 percent of those aged 65 and over who used
4
A measure of annual income is multiplied by 0.00138889 to define a daily rate.

26
nursing services report spending $0). Only 6 percent of seniors who use nursing services paid
$200 or more in a typical month for the help received. People are more likely to pay for personal
and home support (which includes things like housekeeping) and other supports (such as meal
delivery). In a typical month, 18 percent of those relying on personal and home supports spend
$200 or more.
Table 13: Amounts Paid for Home Care Services Used, by Type of Service (Age 65+)
Amount paid (typical month)
Nursing
Other health
Med.
Equip
Support
Other
$0
0.87
0.83
0.66
0.51
0.35
$1-less than $50
0.04
0.05
0.08
0.11
0.22
$50-less than $100
0.02
0.03
0.05
0.11
0.17
$100-less than $200
0.01
0.03
0.06
0.10
0.10
$200 or more
0.06
0.06
0.14
0.18
0.16
Source: CCHS tabulations, years 2015, 2016, 2018, 2019. Each column sums to 1.
Reliance on informal or unpaid care
Our tabulations presented earlier in Figure 7 and Table 11 suggest 17 percent of individuals aged
65 or older, and 41 percent of individuals aged 85 or older, rely heavily on unpaid care or help.
We provide more granular detail on informal care provision at the end of the next subsection.
Total use of care
Combining our information on help received at home in Figure 7 with the information on the
proportion of people living in collective dwellings in Table 7 allows some insight into the overall
distribution of types of care. In Figure 8 we combine these data for those using care (either at
home or because they live in a nursing home or hospital) into one chart for each of the two age

27
groups.
5
These data come from different sources but are useful to gain a rough sense of how the
types of care are distributed. Among those using some type of care, the share in a nursing home
or hospital rises from 17 percent in the age 65 and older population to 28 percent in the age 85
and older population. A smaller proportion uses only unpaid help at age 85 and older than at
younger ages. The pattern here can be characterized as showing an increase in the use of
professional care types at older ages.
Figure 8: Distribution of Types of Care
Source: Combined data from Figure 7 and Table 7; see the sources indicated there. Each pie
segment shows the proportion needing the indicated care type, among the population using any
type of care for each age group.
II.B Care providers
The care sector is labor intensive, but that labor is employed through various occupations spread
across multiple sectors. There is also paid and unpaid work performed in this sector, with various
degrees of skill, both with and without formal training. This subsection looks at the types and
5
For this calculation, we exclude the residents of ‘seniors residences’ reported in Table 7 since these are not care
facilities. We do include the category of facilities that combine seniors’ residence and nursing home services, since
those facilities do provide care.
40%
35%
8%
17%
Age 65+
41%
27%
5%
28%
Age 85+
Both types of
help
Unpaid help
only
Paid help only
Nursing home
or hospital

28
characteristics of the workers providing the care, then moves onto wages and understanding
those who work without pay.
Institutional care workers
A wide range of occupations are involved in providing care to elderly individuals in institutions.
We describe those care workers who report working in the “nursing and residential care
facilities” industry (NAICS code 623) in Table 14 and Figure 9.
Table 14: Individuals Working in Nursing Homes and Residential Care, 2016
Occupations
NOCs
(4-digit)
Number
Female (%)
Canadian born
(%)
Registered Nurses,
Supervisors
3011-3012
32,240
92.3
64.1
Licensed Nurses
3233
23,095
91.2
64.4
Nurses aides, orderlies
3413
131,030
90.3
62.5
Total
NA
186,375
90.7
63.0
Source: Tabulations using Census 2016 master files. Sample of individuals working in NAICS
6230.
From Census data in Table 14, we see that in 2016 there were more than 186 thousand people
working in institutional care as care workers. Nurse aides and orderlies were the most common
occupation in this industry (131 thousand workers) and 55 thousand licensed and registered
nurses worked in these facilities. These jobs are predominantly filled by women (90.7 percent
overall). We note that while nursing occupations are more than 90 percent female, management
positions (not listed here) are more likely filled by men than other occupations (being 71 percent
female). The industry also tends to have fewer Canadian-born workers than the broader labor

29
force.
6
This is particularly true among those working as nurses’ aides and orderlies, where only
62.5 percent of workers are Canadian born.
Figure 9 Education of Workers in Nursing Homes and Residential Care, 2016:
Source: Tabulations using Census 2016 master files. Sample of individuals working in NAICS
6230 within select occupations. See Table 14 for occupation classifications.
Looking at education levels, there are very few nurses who have only completed high school, as
most positions require formal training in a college or university program.
7
Education standards
are part of regulations for long-term care facilities, and the precise details of the standards vary
across provinces. Those working as nurse aides and orderlies are more likely to have lower levels
of education, while 78 percent have completed college or university.
6
Using Statistics Canada Table 14-10-0085-01, Canadian born individuals represented 76 percent of the labor force
in 2016.
7
Given the small sample sizes within some professions at the lowest education levels, we have grouped high school
graduates with those having less than high school to meet confidentiality requirements associated with using the
Census master files.
0% 20% 40% 60% 80% 100%
Nurse aides, orderlies
Reg. Nurses
Licensed Nurses
High school or less College BA or more

30
Formal home care workers
In Table 15 and Table 16 we describe individuals who report working as home care workers
(NOC 4412) in 2016. These data are also drawn from the Census.
Table 15: Number of Home Care Workers in Canada by NAICS
Home Care Workers (NOC 4412)
NAICS:
Number of
workers
Portion
Home health care (6216)
18490
0.19
Nursing homes and res. Care (6230)
10190
0.11
Individual and family services (6241)
28630
0.30
Private Households (8141)
15050
0.16
All other NAICS
23650
0.25
Total
96010
1
Source: Census 2016 tabulations
In Table 15 we see these workers describe themselves as working in a range of industries—
including home health care, nursing homes, individual and family services and private
households. Like nurses and nurses’ aides in institutional care, home care workers (in Table 16)
are predominantly female (89 percent) and less likely than the broader labor force to be Canadian
born (63 percent). Home care workers are also less educated, on average, than those working in
institutional care with 37 percent having completed high school or less.
Table 16: Select Characteristics of Home Care Workers
Portion
Female
0.894
Canadian Born
0.634
Education
Less than high school
0.128
High school
0.247
College
0.482
University (BA+)
0.144
Source: Census 2016 tabulations

31
Wages of paid care workers
For many individuals providing paid care, occupation-specific skills are transferable between
industries. As such, we consider the usual hourly wages with select occupations without
restricting to specific industries. These wage data are presented in Table 17 (for April 2019) and
broader trends in nominal wages are presented in Figure 10.
Table 17: Usual Hourly Wages of Workers in Select Occupations, April 2019
April 2019 wages
Relative to Median Wages of
NOC
Average
Median
All workers
High School or less
Nurse
Supervisors
3011
40.27
43.00
1.68
2.39
Registered
Nurses
3012
37.63
39.00
1.57
2.17
Aides,
Orderlies
3413
20.76
20.35
0.86
1.13
Home Care
Support
4412
18.45
17.00
0.77
0.94
Source: Average and median wages by NOC are provided by the Labour Market Information
Council, using LFS master files. The median wage of all workers ($26.92) and those whose
highest degree is high school or less ($20) is found using the LFS April 2019 PUMF. All dollar
amounts are in nominal terms.
Given the higher education requirements for nurses, it is not surprising their average and median
wages are relatively high. In Table 17, we see that the median wage of registered nurses is 1.57
times the median wage of all workers. Aides and orderlies, who are less educated than nurses
(Figure 10) are paid roughly half as much as nurses and are paid slightly more than the average
worker with high school or less. Home care support workers are paid less than aides and
orderlies, with wages more in line with other workers with high school or less.

32
Figure 10: Wages of Care Workers
Source: Custom tabulations provided by the Labour Market Information Council, using LFS
master files.
In Figure 10 we see that wages of home care support workers have been catching up to those of
nurses’ aides and orderlies. Some of these workers are covered by centralized bargaining and
union contracts in some provinces. For example, Ontario nurses have contracts with hospitals
and nursing homes, using templates that are then tailored to specific workplaces.
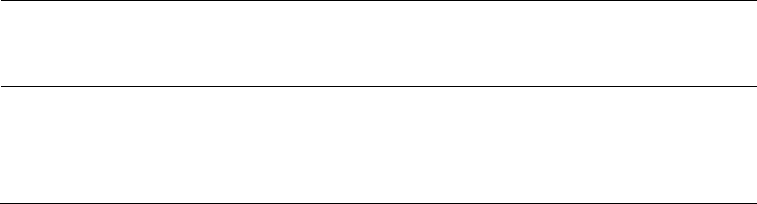
Unpaid caregivers
As shown in Figure 7, many seniors rely on unpaid care and help. In Figure 11, we describe the
portion of individuals (by age group) that reports providing informal unpaid care to someone
because of a long-term health condition or aging. We see a significant portion of the population
provides such care, with the largest share among those aged 50-59 (37 percent). We also see that
33
older individuals are more likely to be the caregivers of elderly recipients compared to a broader
sample of all caregivers.
Figure 11: Provision of Care by Age
Source: GSS Cycles 32 (2018) and 26 (2012) tabulations by authors. All caregivers represent
individuals who indicate they provide care to someone because of a long-term health condition
or aging. Caregivers of the elderly represents the subset of individuals who provide care to at
least one person age 65 or older.
The characteristics of caregivers are reported in Table 18. We see that caregivers are distributed
across all age groups, although those caring for at least one elderly person (age 65 or older) are
more likely from older age groups themselves. Caregivers are slightly more likely to be female
(54 percent) and their education levels closely resemble those of the broader population.
8
8
The education levels presented in Table 18 are similar to 2018 levels found using LFS PUMFs, where for example
26 percent of all individuals have a BA or more and 15 percent have less than high school.

34
Table 18: Characteristics of Informal Care Providers
All caregivers
Care for elderly
person
Age group
29 or under
0.205
0.158
30-39
0.128
0.105
40-49
0.176
0.188
50-59
0.243
0.272
60-69
0.159
0.177
70+
0.089
0.101
Female
0.540
0.540
Education
Less than High
School
0.129
0.113
High School Grad.
0.268
0.256
Trades/College
0.334
0.339
BA+
0.270
0.291
Source: GSS Cycles 32 (2018) and 26 (2012) tabulations by authors.
Sample of individuals who report being caregivers, providing care to family or
friends due to a long-term health condition or aging. Caregivers for an elderly
person are the subset of caregivers who provide care to at least one person age 65
or older.
We now turn to the question of who is providing informal care. In Table 19, the data shows that
spouses provide a lot of informal care, as 35.7 percent of care recipients reported their spouse as
the primary caregiver.
9
As one might expect given the age distribution of caregivers in Table 18,
the elderly often rely on their children for care. Daughters are commonly a person’s primary
caregiver (30.5 percent), while sons and in-laws are less likely to be the primary caregiver (15.3
percent and 3.4 percent respectively).
9
We note that when caregivers are asked who their primary care recipient is, only 8 percent of those caring for at
least one elderly person reports their spouse as the primary recipient. This suggests many caregivers are many
individuals’ primary caregiver.

35
Table 19: Primary Caregiver Relationship to Elderly Recipients
Relationship to care recipient
Portion
Spouse
0.357
Son
0.153
Daughter
0.305
Son/Daughter in law
0.034
Other relatives
0.073
Non-relative
0.079
Source: GSS Cycles 32 (2018) and 26 (2012) tabulations by authors.
Sample represents individuals aged 65 or older who receive informal care;
relationship characterizes who their primary caregiver is. Caregivers provide care
to family or friends due to a long-term health condition or aging.
The elderly will also rely on relatives other than their children and spouses. We also see in Table
19 that 7 percent of elderly care recipients report their primary caregiver is another relative—
such as an aunt or cousin. A sizeable group of elderly individuals rely on caregivers who are not
their relatives.
Table 20: Hours of Informal Care Provided per Week
Hours of care
All caregivers
Care for elderly
person
Mean
12
11
25th percentile
2
1
Median
4
3
75th percentile
10
10
Source: GSS Cycles 32 (2018) and 26 (2012) tabulations by authors.
Caregivers provide care to family or friends due to a long-term health condition or
aging. Caregivers for an elderly person are the subset of caregivers who provide
care to at least one person age 65 or older.
Finally, we turn to the hours of care provided by informal caregivers, in Table 20. Many
individuals provide care (as in Figure 11), but most provide only a few hours of care every week.
Typically, caregivers who provide care to at least one elderly person are providing only 3 hours
of care every week (median). The distribution of hours of care, however, is clearly skewed, with

36
an average hours of care that is higher than the 75
th
percentile. Worth noting, the hours of care
among caregivers of the elderly is not higher than the hours of care among all caregivers.
Part III: Canada’s Long-Term Care System
Long-term care in Canada is financed by public and private sources. In this section, we describe
the general structure of the public funding programs and the features of the private long-term
care insurance market. We close the section with a summary of the shares of spending from
different sources.
III.A. Public Systems
Each province and territory operates its own long-term care system. There are publicly owned
long-term care homes and also public subsidies for lower-income people. In many provinces the
public subsidies can be used at private facilities. Access to public facilities is by application, with
the criteria generally including citizenship, residency, age, and health. For example, in British
Columbia an applicant needs to be a Canadian citizen or permanent resident, have lived in
British Columbia for at least 3 months, be 19 years of age or older, and “be unable to function
independently because of chronic, health-related problems…”
10
Needs are assessed, and the
appropriate care facility type is offered.
10
See https://www2.gov.bc.ca/gov/content/health/accessing-health-care/home-community-care/are-you-eligible.

37
For public subsidies, each province has its own formula.
11
Typically, there is a minimum
contribution required which is generally aligned closely with the value of federal Old Age
Security and Guaranteed Income Supplement payments (designed to set a minimum personal
allowance for the person receiving care). For income higher than these federal pensions, the
provincial subsidy is typically clawed back. There are also asset tests in Quebec and in
Newfoundland and Labrador.
The public subsidy formula’s minimum personal allowance (or minimum contribution) and
clawback rates differ across provinces. For example, in Quebec (in 2022) the personal allowance
was set at $290 per month. Every dollar of income over that allowance is clawed back to pay for
the individual’s long-term care fees (at $2,019 per month). In British Columbia, a minimum
allowance of $325 is set aside, and 80 percent of additional income is clawed back (with a
maximum rate of $3,847.20 in 2023). In Saskatchewan, the personal allowance (for 2023) was
set at $466 per month (as the difference between their minimum fee and a first income threshold
defined at $1,759), and income is then clawed back at a rate of 57.5 percent (with a maximum
rate of $3,218).
III. B. Private Long-Term Care Insurance
Health insurance in Canada is dominated by provincial public health insurance programs that list
a wide range of insurable services. Many employers offer supplemental health insurance to cover
services not insured by the public plans, most notably pharmaceuticals, dental, and vision care.
Those on public income assistance have access to public coverage for these supplemental needs,
11
See Blomqvist and Busby (2012) for a description of the system and details on each province. Library of
Parliament (2020) provides an update.

38
but some Canadians have no supplemental health coverage. For long-term care insurance, few
employer-sponsored supplemental plans cover long-term care risks.
Beyond the group insurance market, there is a small and shrinking market for individual private
long-term care insurance. The available policies typically require two or more ADLs to trigger a
payment under the policy. The policies are priced by age and sex. These long-term care
insurance policies are not often bundled with other insurance products on the private market, but
instead sold as a standalone product. (Boyer et al. 2020, p. 139) This might make these products
more difficult to sell because of the increased marketing costs. Several providers have fallen out
of the market, with few options left on the market.
12
Table 21: Features of Long-Term Care Insurance Market
Age
Has
LTCI
Average
Premium
Average
Benefit
50-54
0.154
83
2307
55-59
0.113
173
1693
60-64
0.089
117
2310
65-70
0.054
120
2155
Source: Retirement Savings Institute, HEC Montreal survey RSI-01. See Boyer et
al. (2020).
A 2016 survey of Quebec and Ontario residents ages 50-70 found that 10.5 percent had
purchased a long-term care insurance policy. The average premium was $116 and the average
insured benefit was $2,467.
13
The age pattern of these characteristics is shown in Table 21. There
is a clear downward gradient in long-term care insurance uptake from 15.4 percent at ages 50-54
to 5.4 percent at ages 65-70. The premium and the benefit, however, do not have clear trends
12
For example, in 2021 Sun
Life (a major insurer) raised their long-term care insurance policy premiums for
existing customers and closed the product to new sales. SunLife now offers a new product that requires a 1 to 2
year waiting period for any benefit
https://www.sunlife.ca/en/health/long-term-care-insurance/clarica-and-sun-
long-term-care-insurance-policyowners/
13
See Boyer et al. (2020) for details.

39
across ages. As the number of firms offering such insurance has continued to shrink since 2016,
the proportions with a policy are likely even lower today.
III. C
. Summary of Financing Shares
Taking the different financing sources together, we can depict the different financing shares as a
percent of the total. The data from the OECD used here include all types of long-term care
(institutional, community care, and home care) for care recipients of any age. Later in the paper,
we focus more closely on those age 65 and older. Figure 12 shows that public financing
represents 78.4 percent of spending, with private spending making up the residual 21.6 percent.
The strong majority of the private financing comes from out-of-pocket spending, with insurance
payments making up only 3.3 percent of the total.
Figure 12: Long-Term Care Financing by Source
Source: OECD Health Expenditure and Financing database.
III.D. Long-term Care as Share of Economy
Public
78.4%
Private,
insurance
3.3%
Private, out
of pocket
18.3%

40
In Figure 13 we put these costs in context by comparing them to GDP. This comparison is useful
both to understand the impact of the long-term care system on the Canadian economy and also to
facilitate international comparisons. Again, we use the OECD data that include spending on all
types of long-term care and at all ages. Over the 31 years from 1990 to 2021, the share of GDP
going to long-term care rose from under 1 percent of GDP in 1990 to more than 2 percent by
2021. In constant 2019 Canadian dollars, this represents an increase from $11 billion in 1990 to
$52 billion in 2021.
14
The nominal value in current dollars for 2021 is $54 billion.
Figure 13: Share of GDP Spent on Long-Term Care
Source: OECD Health Expenditure and Financing database.
Part IV: Total Cost of Long-Term Care
In this section we bring together elements of the data presented in this paper to produce an
estimate of the total cost of care. We now narrow our focus to those age 65 and older. We aim
14
See Grignon and Spencer (2018) for a discussion of the shortcomings of the OECD long-term care estimates.
0.00
0.50
1.00
1.50
2.00
2.50
1990 1995 2000 2005 2010 2015 2020
41
our calculations for 2019, reported in 2019 Canadian dollars. For each of three line items
(residential long-term care, home care, informal care) we present an estimate of the number of
users and total spending. We then calculate a cost per user for each of the three line items. We
begin by going through the source of each element of the calculation for each line item, then
bring it together in a final calculation at the end of the section.
IV.A Residential long-term care
We have different sources to draw on for the total number of people in care and the total cost.
We describe the sources and our choices for the total cost calculation here.
For the count of people, our Census counts reported in Table 7 show 172,000 in nursing homes,
151,000 in seniors’ residence, and another 65,000 in combined nursing homes and seniors’
residences. So, a narrow definition of just “nursing homes” would yield 237,000 people. In Table
9, we report the National Health Expenditure Database count of beds in long-term care
residences, which is 198,220. For the total cost calculation, we use the Census count of nursing
homes: 237,000 people.
For costs, we rely primarily on data from the OECD Health Statistics Database OECD (2022),
supplemented with information from the National Health Expenditure Database (Canadian
Institute for Health Information 2021). The differences between these data sources are
documented and explored in Grignon and Spencer (2018), who find the OECD measures too
broad in most cases compared to their preferred measure. For residential long-term care, we
begin with the OECD estimates for “in-patient long-term care.” This includes individuals of any
age. To produce an estimate for ages 65 and older, we use the age-based breakdown from the

42
National Health Expenditures Database which finds for 2019 that those age 65 and older
represent 78.7 percent of total residential long-term care expenditures.
15
Our estimate for residential long-term care expenditures using this method is $27.9 billion for
2019. This is split between $19.6 billion in public spending and $8.3 billion in private spending,
for roughly a 70/30 percent public/private split. Our estimates are in line with other estimates,
including the results presented in National Institute on Ageing (2019).
IV.B Paid Home Care
We now turn to formal, paid home care. In Table 11 we use the Canadian Community Health
Survey and find that for those age 65 and older, the proportion who report paid care is 9.2
percent. In Figure 7 we employ the General Social Survey, where the percent who report using
any paid care is 11 percent. For our calculations, we use the number from the GSS: 11 percent.
There were 6.6 million Canadians ages 65 and older in 2019, so we estimate 726,000 are users of
formal paid home care.
For costs, we again rely on data from the OECD Health Statistics database (OECD 2022), which
provides a total cost of home care for the public sector. Grignon and Spencer (2018) note that the
OECD does not provide estimates for private home care, but instead allocates those expenditures
elsewhere in its health accounts. Alternatively, Grignon and Spencer (2018) present a method to
estimate private expenditures, finding for the period up to 2014 the average share of private
15
We use Series E3, Table E.3.24.1. The category “other institutions” is mainly residential long-term care facilities.

43
spending is about 28 percent. We use this number to interpolate a private expenditure for home
care, by applying the 28 percent share to the dollar value provided by the OECD.
The OECD public home care estimate (across all ages) is $11.5 billion. To adjust for the
proportion of these expenditures associated with those age 65 or higher, we draw on a data
source from the Canadian Institute for Health Information which reports the age splits for clients
in a subset of provinces.
16
This source has 87 percent of clients age 65+. Of course, the services
provided across ages may differ so this division is perhaps rough. We apply this 87 percent then
multiply by (0.28/0.72=0.3888) to find the associated private sector home care spending amount.
We arrive at an estimate of $10 billion for public homecare and $3.9 billion for private
homecare. This is larger than found by National Institute on Ageing (2019), who report only $4
billion in public and $2 billion in home care expenditures. However, our public homecare
estimate is in line with the National Health Expenditures Database reported total for 2019 of
$10.2 billion for the public sector across all ages.
IV.C Unpaid Home Care
To estimate the cost of unpaid home care, we first derive an estimate for the number of hours of
care that is used by recipients. Since those hours of care are not contracted in a market, there is
no wage to observe. The person providing the care does have a value for their time, either
because those hours could potentially be sold to the market (if the caregiving person is working)
or because those hours must come out of leisure time that could otherwise be maintained by
16
We use tables from the 2021 Home Care Reporting System data provided by the Canadian Institute for Health
Information.
44
paying for care. Below, we explain two different methods of valuing these hours provided to
caregiving that incorporate these opportunity costs of time in different ways.
For someone who has a job, hours spent caregiving might come out of hours that could be sold to
their employer. If the labor market is competitive and flexible, then we can value that time at the
observed market wage for those individuals. We do so by taking the average hourly wages in the
2019 Labour Force Survey by age-gender-education group. Then, we use the age-gender-
education information in Table 18 to develop a composite wage that corresponds to the typical
demographics of caregivers. The average wage calculated in this way for 2019 is $27.34/hour.
This estimate of a caregiver’s opportunity cost is how we value foregone potential work hours
that are devoted to informal caregiving. Below, we refer to this as
.
For someone without a job, the hours spent caregiving can be valued in different ways,
depending on how we think about leisure. At one extreme, hours taken out of leisure could be
valued at zero. At the other extreme, the hours could be valued at the potential cost of market
care—the observed hourly wage of homecare workers. Our estimate for this wage comes from
Table 17. For home-care support workers, the average hourly wage is $18.45/hour. Below we
refer to this as
.
We combine this information into a single estimate by using the composite wage for workers to
value time for those who have a job, and two different estimates ($0 and $18.45) for valuing the
time of those without a job. Using the comparable age-education-gender groups in the Labour
Force Survey we find the proportion of people in each group who are working and use this

45
proportion and the implicit wage information to form the estimate. The proportion working using
this cell-average strategy in 2019 is 0.584.
The ‘low’ valuation assigns no value to leisure:
(
)
×
+ 1
(
)
× 0.
The ‘high’ valuation incorporates the value of leisure at the cost of hiring a paid caregiver:
(
)
×
+ 1
(
)
×
.
In each valuation case, we multiply the resulting implicit cost by the total number of hours of
unpaid caregiving in Canada. To find this number, we start with Table 10Table 10 where we
report that the average number of hours per week of informal care, among those receiving care is
22. Figure 7, using data from the Canadian Community Health Survey, finds that the proportion
using any unpaid help is 17 percent. With 6.6 million Canadians ages 65 and older, that is
1,122,000 recipients of unpaid help. At an average of 22 hours per week and 1,144 hours per
year, the total number of hours per year comes to 1,284 million hours.
We summarize these valuation calculations in Table 22 below. The left column shows the ‘low’
valuation described above, while the right column shows the ‘high’ valuation.
Table 22: Valuation of Informal Care
Low
High
Valuation (billions)
20.5
30.4
Total hours unpaid work
(millions)
1,284 1,284
prob(employed)
0.584
0.584
Wages/hour if employed
$27.34
$27.34

46
Wages/hour of caregiver
0
$18.45
Valuation per hour
$15.97
$23.64
Source: authors’ calculations, as described in the text. Dollar values are in 2019 Canadian
dollars.
IV.D Total Cost of Care
We aggregate the estimates discussed above for residential long-term care, formal home care,
and informal care in Table 23 below. The first two columns are drawn directly from the
discussion above. The third column provides a comparison in terms of GDP, and the last column
shows a per capita amount for each category. These estimates are for Canadians ages 65 and
older, and the estimates are centered around 2019 so we report in 2019 Canadian dollars. We
provide both public and private sector estimates for residential long-term care and formal home
care, along with a total. The informal care cost considers the two cases with the low valuation
(zero value of leisure) and the high valuation (leisure funded by paying for market-wage
homecare).

47
Table 23: Estimates of Total Cost of Care
Number
of users
Total
Spending
GDP
Share
Spending per
user
Residential Long-term care
Public
19.6
0.85%
Private
8.3
0.36%
Total
237,000
27.9
1.21%
$117,865
Formal home care
Public
10.0
0.43%
Private
3.9
0.17%
Total
726,000
13.9
0.60%
$19,150
Informal care
Low valuation
1,122,000
20.5
0.89%
$18,270
High valuation
1,122,000
30.4
1.31%
$27,000
62.3
Total (low valuation)
2.69%
Total (high valuation)
72.2
3.12%
Source: authors’ calculations, as described in the text. Dollar values are in 2019 Canadian
dollars; shares are the share of 2019 GDP.
Summed across these three types, the total cost of care is $62.3 billion for the low valuation, and
$72.2 billion for the high valuation. Nominal GDP in 2019 for Canada was $2.31 trillion, so in
the second last column we restate all the total cost information as a share of GDP to provide
better context for the overall fiscal bite and for international comparisons. Using the low
valuation, long-term care costs 2.69% of 2019 GDP; using the high valuation it is 3.12%.
Finally, in the last column we express the cost per user. Residential long-term care is much more
expensive, at nearly $118,000 per year per resident. Formal home care is about $19,000 per year
on average, with informal care in the range of $18,000 to $27,000.

48
Conclusions
This paper has provided a broad overview of long-term care for older Canadians, looking at the
economics of both the demand and supply sides of caregiving. Like other OECD countries, the
coming demographic wave of older baby boomers will put tremendous stress on the existing
financial, organizational, and physical structures of the long-term care system. Unlike other
OECD countries, Canada’s system is organized almost entirely at the subnational level, with
provinces and territories having by far the largest role in financing and regulating long-term care.
The unique federal structure of long-term care in Canada presents challenges and opportunities.
The greater ease of the federal government to tax and borrow could provide extra revenue to
fund necessary investments in bricks and mortar infrastructure or in ongoing annual
expenditures. However, whatever financial role the federal government may play, the
opportunity of decentralized experimentation (in the “federalism as a laboratory” spirit of Justice
Brandeis) should not be dismissed.
17
Innovations on regulations, training, and financing may
arise from provinces pursuing different models. Even here, the federal government can
contribute by encouraging learning and co-operation through federal benchmarks as well as
convening national dialogue.
17
In the well-known case of New State Ice Co. V. Liebman 285 US 262 (1932), Justice Brandeis wrote “It is one of
the happy incidents of the federal system that a single courageous state may, if its citizens choose, serve as a
laboratory; and try novel social and economic experiments without risk to the rest of the country.”

49
References
Baker, Michael and Milligan, Kevin. 2009. “Government and Retirement Incomes in Canada,”
Report prepared for the Council of Federal, Provincial, and Territorial Finance Ministers.
Blomqvist, Ake and Busby, Colin. 2012. “Long-Term Care for the Elderly: Challenges and
Policy Options,” C.D. Howe Institute Commentary No. 367.
Bohnert, Nora, Jonathan Chagnon, Simon Coulombe, Patrice Dion and Laurent Martel. 2015.
Population Projections for Canada (2013 to 2063), Provinces and Territories (2013 to 2038):
Technical Report on Methodology and Assumptions. Statistics Canada, Catalogue No. 91-620-X.
https://www150.statcan.gc.ca/n1/en/pub/91-620-x/91-620-x2014001-eng.pdf?st=UxgEwf70
Boyer, M. Martin, De Donder, Philippe, Fluet, Claude, Leroux, Marie-Louise, and Michaud,
Pierre-Carl. 2020. “Long-Term Care Insurance: Information Frictions and Selection,” American
Economic Journal: Economic Policy. Vol. 12, No. 3, pp. 134-169.
Canadian Human Mortality Database. 2022. Department of Demography, Université de Montréal
(Canada). Available at http://www.bdlc.umontreal.ca/CHMD/ (data downloaded April 5, 2022).
Canadian Institute for Health Information. 2021. National Health Expenditure Trends, 2021 —
Methodology Notes. Ottawa, ON: CIHI.
Grignon, Michel and Spencer, Byron G. 2018. “The Funding of Long-Term Care in Canada:
What Do We Know, What Should We Know?” Canadian Journal on Aging, Vol. 37, No. 2, pp.
110-120.
Library of Parliament. 2020. “Long-Term Care Homes in Canada – How are They Funded and
Regulated?” Hillnotes online publication. https://hillnotes.ca/2020/10/22/long-term-care-homes-
in-canada-how-are-they-funded-and-regulated/
Milligan, Kevin. 2008. “The Evolution of Elderly Poverty in Canada,” Canadian Public
Policy, Vol. 34, No. 4, pp. s79-s94.
Milligan, Kevin and Schirle, Tammy. 2021. “The Evolution of Longevity: Evidence from
Canada,” Canadian Journal of Economics, Vol. 54, No. 1, pp. 164-192.
National Institute on Ageing. 2019. Enabling the Future Provision of Long-Term Care in
Canada. Toronto, ON: National Institute on Ageing White Paper.
Organization for Economic Co-operation and Development. 2022. OECD Health Statistics 2022.
Online database, https://www.oecd.org/els/health-systems/health-data.htm.
Ostrovsky, Yuri and Schellenberg, Grant. 2010. Pension coverage and earnings replacement
among Canadian couples. Statistics Canada Analytical Branch Studies Working Paper No. 327,
Catalogue no. 11F0019M.
