
i
Smoking and Tobacco Control Monograph No. 9
Preface
The recent increase in cigar consumption began in 1993 and was dismissed
by many in public health as a passing fad that would quickly dissipate. Recently
released data from the U.S. Department of Agriculture (USDA) suggests that the
upward trend in cigar use might not be as temporary as some had predicted. The
USDA now projects a total of slightly more than 5 billion cigars were consumed
last year (1997) in the United States. Sales of large cigars, which comprise about
two-thirds of the total U.S. cigar market, increased 18 percent between 1996 and
1997. Consumption of premium cigars (mostly imported and hand-made)
increased even more, an astounding 90 percent last year and an estimated 250
percent since 1993. In contrast, during this same time period, cigarette
consumption declined 2 percent.
This dramatic change in tobacco use raises a number of public health
questions: Who is using cigars? What are the health risks? Are premium cigars
less hazardous than regular cigars? What are the risks if you don't inhale the
smoke? What are the health implications of being around a cigar smoker?
In order to address these questions, the National Cancer Institute (NCI)
undertook a complete review of what is known about cigar smoking and is
making this information available to the American public. This monograph,
number 9 in a series initiated by NCI in 1991, is the work of over 50 scientists
both within and outside the Federal Government. Thirty experts participated in
the multi-stage peer review process (see acknowledgments). The conclusions
presented in the monograph represent the best scientific judgment, not only of
the NCI, but also of the larger scientific community.
There is sufficient evidence to conclude that a causal relationship exists
between regular cigar use and cancers of the lung, larynx, oral cavity, and
esophagus. Heavy cigar smoking, particularly for those who inhale, causes an
increased risk of coronary heart disease and chronic obstructive pulmonary
disease. There is also suggestive evidence for a relationship between cigar
smoking and cancer of the pancreas, but the evidence is insufficient at this time
to draw a causal inference. The data in this monograph strengthen and extend
the conclusions on disease risks contained in several reports of the Surgeon
General on smoking and health.
After a careful assessment of the available scientific evidence, the following
overall conclusions are warranted:
Cigar smoking can cause oral, esophageal, laryngeal, and lung
cancers. Regular cigar smokers who inhale, particularly those who
smoke several cigars per day, have an increased risk of coronary
heart disease and chronic obstructive pulmonary disease.

Preface
ii
Regular cigar smokers have risks of oral and esophageal cancers
similar to those of cigarette smokers, but they have lower risks of
lung and laryngeal cancer, coronary heart disease, and chronic
obstructive pulmonary disease.
Cigar use in the U.S. has increased dramatically since 1993. Adult
prevalence of cigar use in California has increased predominantly
among occasional cigar smokers. A substantial number of adult
former and never smokers of cigarettes are currently smoking cigars.
In contrast to cigarettes, much of the increased use of cigars by
adults appears to be occurring among those with higher incomes
and greater educational attainment.
Adolescent cigar use is occurring at a substantial level and is
currently higher than that recorded for young adults prior to 1993.
Currently, cigar use among adolescent males exceeds the use of
smokeless tobacco in several states. This use of cigars is occurring
among both males and females.
Some in the cigar trade have made the claim that cigar smokers experience
little or no increased disease risk. This claim is not supported by the available
scientific evidence and misleads cigar smokers to believe that cigar smoke is less
harmful than cigarette smoke. We believe an accurate statement is that the
risks of tobacco smoke exposure are similar for all sources of tobacco
smoke, and the magnitude of the risks experienced by cigar smokers
is proportionate to the nature and intensity of their exposure.
Differences in the intensity of tobacco smoke exposure between cigarette and
cigar smokers result from differences in the inhalation of the smoke and
differences in the proportion of smokers who smoke every day. While almost all
cigarette smokers inhale, the majority of cigar smokers do not. This may be due
to differences in the pH of the smoke produced by these two products. Cigar
smoke contains a substantial fraction of its nicotine as free nicotine, which can
be readily absorbed across the oral mucosa. In contrast, cigarette smoke is more
acidic, and the protonated form of nicotine it contains is much less readily
absorbed by the oral mucosa. As a result, cigarette smokers must inhale to get
their desired quantity of nicotine, whereas cigar smokers can ingest sufficient
quantities of nicotine without inhaling. This reduction in inhalation is one of
the reasons for the difference in disease risks between cigarette and cigar smokers.
However, even those who do not inhale have disease risks higher than those
who have never smoked any tobacco product. As this monograph clearly
demonstrates, regular cigar smokers who have never smoked cigarettes, even
those who do not inhale, experience significantly elevated risks for cancers of the
larynx, oral cavity (including pharynx), and esophagus.
1
For the California survey, current prevalence among adults was defined as a positive response to:
1) Have you ever smoked cigars? and 2) Do you now smoke cigars every day or some days?

iii
Smoking and Tobacco Control Monograph No. 9
Another reason for a difference in risk between cigarette and cigar smokers is
a difference in the frequency with which the two products are used. Most
cigarette smokers smoke every day. In contrast, as many as three-quarters of
cigar smokers smoke only occasionally, and some may only smoke a few cigars
per year. This difference in frequency of exposure translates into lower disease
risks.
We do not know the risk of addiction posed by cigar smoking. But the
difference in smoking patterns suggests a potential difference in addictive
properties between cigarettes and cigars.
Of special concern are the risks for those individuals who are mixed smokers
(current smokers of both cigars and cigarettes), or who switch to smoking cigars
from smoking cigarettes. A sizable fraction of today's cigar smokers are current or
past cigarette smokers. These individuals are much more likely to continue to
inhale when they switch to smoking cigars, and may therefore remain at much
higher risk for all the major smoking related diseases than are cigar smokers who
have never smoked cigarettes.
To those individuals who may be thinking about smoking cigars, our advice
is — don't. Cigars are not safe alternatives to cigarettes and may be addictive.
To those cigarette smokers who are thinking of switching to cigars, don’t be
misled. Unless you substantially reduce your exposure to smoke, your risks will
remain unchanged.
To those currently smoking cigars, quitting is the only way to eliminate the
documented harm that can result from cigar smoking.
Once regular tobacco use is established, no matter whether it’s cigarettes,
cigars, or smokeless tobacco, quitting may become extremely difficult.
To all smokers and nonsmokers, tobacco smoke contains over 4,000
compounds, including dozens of carcinogens. Because of their greater mass,
cigars generate much higher levels of many of these indoor pollutants than do
cigarettes. Smoke from a single cigar burned in a home can require 5 hours to
dissipate, thereby exposing other household members to a sizable involuntary
health risk.
A special concern generated by the data in this monograph is the rate of cigar
use among adolescents. Prior to the current upswing in cigar use, most cigar
smokers were middle aged or older men, and they began smoking cigars as adults.
In contrast, several studies now report cigar smoking prevalence rates among
adolescent males that are more than double the rates of smokeless tobacco use.
In a 1996 survey of Massachusetts school students in grades 6 through 12,
prevalence of current cigar use among males ranged from 3.2 percent in 6th
graders to 30 percent in high school. Adolescent girls also report surprisingly

Preface
iv
high rates of cigar use, with 6-7 percent of girls in high school reporting they
smoked cigars in the past 30 days. Similar findings are reported in other studies.
This high rate of cigar use among adolescents raises significant public health
questions and has serious implications for public health programming. Will
these high rates of cigar use continue as these youth move into adulthood? Will
nicotine addiction develop in these adolescent users and thereby influence their
inhalation and consumption patterns? Will cigar smoking transition large
numbers of youth into regular cigarette use later in life? If regular cigar use
develops, will quitting prove as difficult for cigars as it is for cigarettes?
It is premature to label cigar use as the next tobacco epidemic in the making;
but we would be wise to remember that a similar problem of smokeless tobacco
use confronted us in the late 1970's, and it was a number of years before the
public health community became concerned. Now, 20 years later, consumption
of smokeless tobacco, especially moist snuff, has reached record levels — 60
million pounds last year, and shows no sign of waning. The vast majority of all
snuff users are younger-age adults and adolescents, a pattern not dissimilar to the
current pattern of cigar use.
This monograph provides us with a snapshot of a rapidly changing pattern of
behavior with important potential public health consequences. I commend the
authors for providing the nation with clear and invaluable information about
this disturbing change in tobacco use.
Richard D. Klausner, M.D.
Director
National Cancer Institute

v
Smoking and Tobacco Control Monograph No. 9
Acknowledgments
Cigars: Health Effects and Trends was developed under the editorial direction of
Donald R. Shopland, Coordinator, Smoking and Tobacco Control Program
(STCP), National Cancer Institute, Bethesda, Maryland.
The Senior Scientific Editor for this monograph was David M. Burns, M.D.,
Professor of Medicine, School of Medicine, University of California San Diego, San
Diego, California. The Consulting Scientific Editors were Dietrich Hoffmann,
Ph.D., Associate Director, American Health Foundation, Valhalla, New York and
K. Michael Cummings, Ph.D., M.P.H., Senior Research Scientist, Roswell Park
Cancer Institute, Buffalo, New York. The Managing Editor for this monograph was
Richard H. Amacher, Project Director, KBM Group Inc., Silver Spring, Maryland.
The editors and STCP staff members gratefully acknowledge the
many researchers and authors who made this monograph possible.
Attributions for each chapter are as follows:
Chapter 1. Cigar Smoking: Overview David M. Burns, M.D.
and Current State of the Professor of Medicine
Science School of Medicine
University of California San Diego
San Diego, CA
Chapter 2. Trends in Cigar Karen K. Gerlach, Ph.D., M.P.H.
Consumption and Epidemiologist
Smoking Prevalence Office on Smoking and Health
Centers for Disease Control and Prevention
Atlanta, GA
K. Michael Cummings, Ph.D., M.P.H.
Senior Research Scientist
Department of Cancer Control and
Epidemiology
Roswell Park Cancer Institute
Buffalo, NY
Andrew Hyland, M.A.
Data Analyst
Department of Cancer Control and
Epidemiology
Roswell Park Cancer Institute
Buffalo, NY
Elizabeth A. Gilpin, M.S.
Senior Statistician
Cancer Prevention and Control
University of California San Diego
La Jolla, CA

Acknowledgments
vi
Michael D. Johnson, Ph.D.
Chief
Data Analysis and Evaluation Unit
California Department of Health Services
Tobacco Control Section
Sacramento, CA
John P. Pierce, Ph.D.
Professor and Associate Director
Cancer Prevention and Control
Sam M. Walton Professor for Cancer
Research
University of California San Diego
La Jolla, CA
Chapter 3. Chemistry and Toxicology Dietrich Hoffmann, Ph.D.
Associate Director
American Health Foundation
Valhalla, NY
Ilse Hoffmann, B.S.
Research Coordinator
American Health Foundation
Valhalla, NY
Chapter 4. Disease Consequences of Thomas G. Shanks, M.P.H., M.S.
Cigar Smoking Principal Statistician
University of California San Diego
San Diego, CA
David M. Burns, M.D.
Professor of Medicine
School of Medicine
University of California San Diego
San Diego, CA
Chapter 5. Indoor Air Pollution James L. Repace, M.S.
from Cigar Smoke Repace Associates
Bowie, MD
U.S. EPA Office of Radiation and
Indoor Air (Retired)
Wayne R. Ott, Ph.D.
Visiting Scholar
Department of Statistics
Consulting Professor
Department of Civil and Environmental
Engineering
Stanford University
Stanford, CA
Neil Klepeis, M.S.
School of Public Health
Environmental Health Sciences
University of California, Berkeley
Berkeley, CA

vii
Smoking and Tobacco Control Monograph No. 9
Chapter 6. Pharmacology and Reginald V. Fant, Ph.D.
Abuse Potential Pinney Associates, Inc.
of Cigars Bethesda, MD
Jack E. Henningfield, Ph.D.
Vice President
Research and Health Policy
Pinney Associates, Inc.
Bethesda, MD
Associate Professor
Department of Psychiatry and Behavioral
Sciences
Johns Hopkins University
School of Medicine
Baltimore, MD
Chapter 7. Marketing and John Slade, M.D.
Promotion of Cigars Professor of Clinical Medicine
University of Medicine and Dentistry of
New Jersey
Robert Wood Johnson Medical School
Saint Peter’s Medical Center
New Brunswick, NJ
Chapter 8. Policies Regulating Cigars Gregory N. Connolly, D.M.D., M.P.H.
Director of the Massachusetts Tobacco
Control Program
Massachusetts Department of Public Health
Boston, MA
We gratefully acknowledge the following distinguished scientists, researchers, and
others, both in and outside Government, who contributed critical reviews or assisted in
other ways:
Anthony Alberg, Ph.D., M.P.H.
Assistant Scientist
Johns Hopkins University
Baltimore, MD
Dileep G. Bal, M.D.
Chief
Cancer Control Branch
California Department of Health Services
Sacramento, CA
Steve Bayard, Ph.D.
Director
Office of Risk Assessment
Health Standards Program
OSHA, Department of Labor
Washington, DC
Neal L. Benowitz, M.D.
Professor of Medicine
Chief
Division of Clinical Pharmacology
and Experimental Therapeutics
University of California San Francisco
San Francisco, CA
Lois Biener, Ph.D.
Senior Research Fellow
Center for Survey Research
University of Massachusetts Boston
Boston, MA
Michele Bloch, M.D., Ph.D.
Chair
Tobacco Control and Prevention
Subcommittee
American Medical Women’s Association
Alexandria, VA

Acknowledgments
viii
Tom Capehart, M.S.
Agricultural Economist
Economic Research Service
United States Department of Agriculture
Washington, DC
Sir Richard Doll, F.R.S., F.R.C.P.
Emeritus Professor of Medicine
Radeliffe Infirmary
University of Oxford
Oxford
United Kingdom
Michael Eriksen, Sc.D.
Director
Office on Smoking and Health
National Center for Chronic Disease
Prevention and Health Promotion
Centers for Disease Control
and Prevention
Atlanta, GA
Lawrence Garfinkel, M.A.
Consultant
American Cancer Society
New York, NY
Ellen Gritz, Ph.D.
Professor and Chair of the Department of
Behavioral Science
University of Texas
MD Anderson Cancer Center
Houston, TX
S. Katharine Hammond, Ph.D., CIH
Associate Professor of Environmental
Health Sciences
School of Public Health
University of California
Berkeley, CA
Thomas P. Houston, M.D.
Director
Department of Preventative
Medicine and Environmental Health
American Medical Association
Chicago, IL
John Hughes, M.D.
Professor
Department of Psychiatry
Ira Allen School
University of Vermont
Burlington, VT
Murray J. Kaiserman, Ph.D.
Acting Director
Office of Tobacco Control
Health Protection Branch
Ottawa, Ontario
CANADA
C. Everett Koop, M.D.
Bethesda, MD
U. S. Surgeon General (1981-1989)
Claude Lenfant, M.D.
Director
National Heart, Lung, and Blood Institute
National Institutes of Health
Bethesda, MD
Alan I. Leshner, Ph.D.
Director
National Institute on Drug Abuse
National Institutes of Health
Rockville, MD
John L. Pauly, Ph.D.
Cancer Research Scientist V
Department of Molecular Immunology
Roswell Park Cancer Institute
Buffalo, New York
John Pinney, B.A.
President
Pinney Associates, Inc.
Bethesda, MD
Richard W. Pollay, Ph.D., M.B.A.
Professor of Marketing
Faculty of Commerce
University of British Columbia
Vancouver, British Columbia
CANADA
Bill Rickert, Ph.D.
President
Labstat Incorporated
Kitchener, Ontario
Associate Professor
Department of Statistics
University of Waterloo
Waterloo, Ontario
CANADA
Nancy A. Rigotti, M.D.
Director
Tobacco Research and Treatment Center
General Internal Medicine Unit
Massachusetts General Hospital
Boston, MA

ix
Smoking and Tobacco Control Monograph No. 9
Jeffrey Wasserman, Ph.D.
Consultant
The RAND Corporation
Santa Monica, CA
Judith Wilkenfeld, J.D.
Special Advisor to the Commissioner
Food and Drug Administration
Rockville, MD
Ernst L. Wynder, M.D.
President
American Health Foundation
New York, NY
Mitchell R. Zeller, J.D.
Associate Commissioner
Food and Drug Administration
Rockville, MD
Finally, the editors and STCP staff members would also like to acknowledge the
contributions of the following individuals who provided technical and editorial assistance
in the preparation of this monograph. We would particularly like to acknowledge the staff
of Business Images, Vienna, Virginia, especially Allen Côté, Marleen Flegel, and Ken Snow
for their invaluable assistance during the final production phase of the monograph.
KBM Group, Inc., Silver Spring, MD
Shelia Russell McCullers, M.S., Information Coordinator/Assistant Managing Editor
Thomas H. Gough, B.A., Technical Editor
Barbara A. Hatfield, A.A.,Copy Editor/Research Assistant
Keith W. Stanger, A.A., Graphics Designer
Heidi Volf, B.A., Copy Editor/Research Assistant
Carleen H. Wallington, M.S., Copy Editor/Research Assistant
Tobacco Control Policies Project, University of California San Diego,
San Diego, CA
Christy M. Anderson, B.S., Statistician
Maureen Arnn, B.S., Project Assistant
Robert W. Davingnon, M.S., Production Editor
Victoria L. Dirac, B.A., Project Assistant
Kathryn B. Gower, B.A., Statistical Assistant
Jacqueline M. Major, M.S., Statistician
Jonathan M. Samet, M.D., M.S.
Professor and Chairman
Department of Epidemiology
School of Hygiene and Public Health
Johns Hopkins University
Baltimore, MD
Jesse L. Steinfeld, M.D.
San Diego, CA
U. S. Surgeon General (1969-1973)
Michael J. Thun, M.D.
Vice President
Epidemiology and Surveillance Research
American Cancer Society
Atlanta, GA
Kenneth E. Warner, Ph.D.
Richard D. Remington Collegiate
Professor of Public Health
Department of Health Management
and Policy
School of Public Health
The University of Michigan
Ann Arbor, MI

Acknowledgments
x
Melissa L. Sage, B.A., Project Assistant
Jerry W. Vaughn, B.S., Programmer/Analyst
Kristina M. Webb, Project Assistant
HOW THIS MONOGRAPH This volume is the ninth in the series of Smoking and Tobacco
WAS PREPARED Control monographs published by the National Cancer
Institute (NCI) since their inception in 1991. One of the major reasons for
establishing the monograph series was to provide a mechanism for the rapid,
systematic, and timely dissemination of information important to the research
and public health communities about emerging issues in smoking and tobacco
use control. While the focus of the monographs has primarily centered on topics
related to public health interventions, this volume is somewhat of a departure in
that it is the first comprehensive examination of what we know about current
trends in cigar use and resultant health implications.
CIGARS: Health Effects and Trends, is being published, in part, because of the
growing and sustained interest in cigars as reflected by the countless inquiries
received over the past two years about the topic by NCI’s Office of Cancer
Communications.
Prior to 1994, smoking of cigars had declined by 60 percent in the United
States, a downward trend which started in the mid-1960’s. Surveys conducted
from the mid-1950’s through the early 1990’s confirmed that cigar smoking was
declining. The public health community assumed, incorrectly it now appears,
that cigar smoking would continue to decline in popularity and did not warrant
further investigation. But starting in the early 1990’s, the downward trend in
cigar use began to reverse; and between 1993 and 1997, cigar consumption
increased almost 50 percent with consumption of large, premium cigars increas-
ing nearly 250 percent.
Public interest, spurred by new magazines devoted entirely to cigars and cigar
smoking, and the social environment that cigar smoking purportedly involves,
was enough to rapidly increase the consumption of cigars. Unfortunately, the
public has been led to believe that cigar smoking is far less of a threat to an
individual’s health than cigarette smoking simply because it is a cigar. The
present monograph is an attempt to dispel this misconception and put the risks
of cigar smoking into their proper context.
The Smoking Tobacco and Control Program (STCP) staff continually
monitors the consumption of all forms of tobacco products, and consequently,
the recent interest and increased consumption of cigars was considered important
enough to the nation’s health to prepare a health oriented publication regarding
cigar smoking.
Once the decision was made by the STCP Coordinator to look into the matter
of cigar smoking, a broad outline was developed showing the major chapters or
topics to be covered in the monograph. A three-person scientific editorial team
was established, consisting of the Senior Scientific Editor, David M. Burns,
Professor of Medicine, University of California San Diego, California, and two

xi
Smoking and Tobacco Control Monograph No. 9
Consulting Scientific Editors, Dietrich Hoffmann, Associate Director, American
Health Foundation, Valhalla, New York, and K. Michael Cummings, Senior
Research Scientist, Roswell Park Cancer Institute, Buffalo, New York. After a more
detailed outline was developed, potential authors were identified and contacted to
determine their willingness to write individual chapters or sections of the
monograph.
A one-day meeting was convened in the Washington, D.C. area in February
1997 involving the entire monograph team. Each lead author presented an
overview of his/her assignment, including how they proposed approaching their
particular chapter, potential sources to be used, the need for primary or secondary
data analysis, and gaps or overlaps in coverage. Discussions and recommendations
followed each presentation.
PEER REVIEW Preliminary draft chapters were delivered to the NCI approximately
4 months following the initial meeting in Washington. The senior scientific
editor, in consultation with the other science editors, reviewed all chapter drafts
for scientific and technical content and advised authors if revisions were needed.
All chapter drafts were distributed to two or more outside experts knowledgeable in
the subject area of the chapter. All review comments received were considered and
a new iteration of the monograph was generated. The revised version of the entire
monograph was sent to a select list of 12 senior level reviewers as well as to a
number of Public Health Service agency heads, for review and comments. All
comments received from this review cycle were also integrated and a third version
of the volume was generated. A total of 30 outside experts participated in the peer
review.
CIGARS: Health Effects and Trends was the work of dozens of individuals, and is
organized into 8 chapters:
Chapter 1: Cigar smoking: Overview and current state of the science.
Chapter 2: Trends in cigar consumption and smoking prevalence.
Chapter 3: Chemistry and toxicology.
Chapter 4: Disease consequences of cigar smoking.
Chapter 5: Indoor air pollution from cigar smoke.
Chapter 6: Pharmacology and abuse potential of cigars.
Chapter 7: Marketing and promotion of cigars.
Chapter 8: Policies regulating cigars.

xiii
Smoking and Tobacco Control Monograph No. 9
Contents
Preface ...............................................................................................i
Acknowledgments ......................................................................................... v
Chapter 1. Cigar Smoking: Overview......................................... 1
and Current State of the Science
Trends in Consumption .............................................................. 1
Disease Risks ........................................................................... 3
Inhalation ................................................................................ 4
Nicotine Addiction .................................................................. 11
Adult Use .............................................................................. 11
Adolescent Use ...................................................................... 13
Marketing .............................................................................. 14
Environmental Tobacco Smoke ................................................ 17
Regulation and Taxation .......................................................... 18
Overall Conclusions ................................................................ 19
References ............................................................................. 19
Chapter 2. Trends in Cigar Consumption ................................ 21
and Smoking Prevalence
Introduction ........................................................................... 21
Discussion ............................................................................. 48
Monitoring Recommendations .................................................. 51
Conclusions ........................................................................... 52
References ............................................................................. 53
Chapter 3. Chemistry and Toxicology ...................................... 55
Historical Notes ...................................................................... 55
The Cigar .............................................................................. 55
Chemistry of Cigar Tobacco ..................................................... 59
Chemistry and Analysis of Mainstream Cigar Smoke .................. 64
Sidestream Smoke and Environmental Tobacco Smoke ............... 76

Acknowledgments
xiv
Chapter 3. Chemistry and Toxicology (Continued)
Toxicity and Carcinogenicity of Cigar Smoke ............................. 83
Biomarkers for the Uptake of Tobacco Smoke ............................ 93
Summary and Research Needs .................................................. 95
Conclusions ........................................................................... 97
References ............................................................................. 97
Chapter 4. Disease Consequences of Cigar Smoking ............. 105
Definition of Terms............................................................... 105
The CPS-I Study ................................................................... 106
All Cause Mortality............................................................... 110
Cause Specific Mortality........................................................ 113
Lung Cancer ........................................................................ 114
Oral Cancers ........................................................................ 120
Cancer of the Larynx ............................................................. 127
Cancer of the Esophagus ........................................................ 130
Bladder and Urinary System Cancers....................................... 130
Pancreatic Cancer ................................................................. 137
Coronary Heart Disease ......................................................... 140
Chronic Obstructive Pulmonary Disease (COPD) ...................... 145
Cerebro-Vascular Disease ...................................................... 149
Aortic Aneurysm .................................................................. 151
Conclusions ......................................................................... 155
References ........................................................................... 155
Appendix: Methods Used in Analyzing CPS-I Data ................... 159
Chapter 5. Indoor Air Pollution From Cigar Smoke ............. 161
Introduction ......................................................................... 161
Mathematical Models for Cigar ETS Concentrations ................. 161
Cigar Emissions: Machine Smoking ........................................ 162
Cigar Emissions: Human Smoking .......................................... 164
Measurements at Cigar Smoking Socials .................................. 170
Discussion ........................................................................... 175
Conclusions ......................................................................... 177
References ........................................................................... 178
Table of Contents

xv
Smoking and Tobacco Control Monograph No. 9
Chapter 6. Pharmacology and ................................................. 181
Abuse Potential of Cigars
Introduction ......................................................................... 181
Early Observations of Addictive Effects .................................. 181
Nicotine Dosing Capability of Cigars ...................................... 182
Inhalation of Cigar Smoke ..................................................... 183
Rate of Nicotine Absorption ................................................... 185
Nicotine Dependence ............................................................ 187
Factors Influencing Nicotine Dependence ................................ 189
Conclusions ......................................................................... 191
References ........................................................................... 192
Chapter 7. Marketing and Promotion of Cigars.................... 195
Introduction ......................................................................... 195
Sales Patterns ....................................................................... 195
Advertising .......................................................................... 198
Promotion ............................................................................ 203
Availability .......................................................................... 215
Discussion ........................................................................... 215
Conclusions ......................................................................... 217
References ........................................................................... 217
Chapter 8. Policies Regulating Cigars .................................... 221
Regulation of Cigar Products .................................................. 221
Health Warnings ................................................................... 223
Disclosure of Cigar or Smoke Product Constituents ................... 223
Advertising Restrictions ........................................................ 224
Regulation of Cigar Smoking in Public Places .......................... 225
Litigation ............................................................................. 225
Restrictions on Youth Access to Cigars .................................... 226
Taxation .............................................................................. 226
Conclusions ......................................................................... 232
References ........................................................................... 232

1
Smoking and Tobacco Control Monograph No. 9
Cigar Smoking: Overview and
Current State of the Science
David M. Burns
Cigars were one form of Native American tobacco use observed by
Columbus and early European settlers. A long, thick bundle of twisted
tobacco leaves wrapped in a dried palm or maize leaf was used by Native
Americans as a primitive cigar. Smoking of cigars is recorded on artifacts of
the Mayas of the Yucatan region of Mexico, and the Mayan verb “sikar,”
meaning to smoke, became the Spanish noun “cigarro.”
Among early English colonists of the 1600’s, tobacco was used
predominantly in the form of smokeless tobacco or smoked in pipes,
although tobacco was also smoked as cigars at this time. Records dating
from the late 1700’s suggest that most cigars were imported from the West
Indies and Cuba during the Colonial period.
The first U.S. cigar factory was established in Connecticut in 1810. Cigar
manufacturing spread to other parts of the U.S. as cigar use slowly gained in
popularity. Through the 1880’s and early 1900’s, cigars remained a popular
form of tobacco use, with most cigars made of locally grown tobacco and
marketed locally. By 1900, tobacco used in the form of cigars accounted for
2.0 of the 7.5 pounds of tobacco consumed per adult in the U.S., second only
to chewing tobacco’s 3.5 pounds per adult (USDA 1997, Burns et al 1997).
However, the amount of tobacco consumed as cigars declined as the
popularity of cigarettes increased around the time of World War I.
Tobacco used to manufacture cigars is different from that used in
cigarettes and other tobacco products. Tobacco contained in cigar filler,
binder and wrappers is predominantly air-cured tobacco in contrast to the
flue-cured tobacco common in cigarettes. Cigar tobacco is then aged and
subjected to a multi-step fermentation process that can last several months,
and this process is largely responsible for the flavor and aroma characteristic
of cigars. Small cigars on the U.S. market have straight bodies and weigh
between 1.3 and 2.5 grams each. Large cigars vary markedly in size and
shape, with the most common dimensions being 110-150 mm long and up to
17 mm in diameter, and they contain between 5 and 17 grams of tobacco
(Chapter 3). By contrast, the most popular brands of cigarettes are 85 mm
long and contain less than one gram of tobacco.
TRENDS IN Since 1993, cigar sales in the U.S. have increased by almost 50%,
CONSUMPTION with the largest increase occurring in sales of large cigars (USDA,
1997). Figure 1 presents U.S. cigar consumption from 1880 through 1997
and shows that cigar consumption declined following the introduction and
marketing of modern blended cigarettes in 1913, and this decline was
accelerated by the Great Depression beginning in 1929. Cigar consumption
remained below that found at the turn of the century until 1964 when it
increased dramatically, possibly as a response to the publication of the first
Surgeon General’s report with its warning about the disease risks of smoking
cigarettes.

Chapter 1
2
Figure 1
Total U.S. cigar consumption 1880-1997 and significant events in the use of cigars
0
1875
U.S. Cigar Consumption (Billions)
2
4
6
8
10
12
14
1895
1915
1935
Year
1955
1975
1995
Modern blended
cigarettes introduced
First Surgeon General’s Report
Advertising of little
cigars begins on TV
Great
Depression
Cigar Aficionado begins publishing
Ban on TV Advertising
of little cigars

3
Smoking and Tobacco Control Monograph No. 9
A loop-hole in the 1969 law banning advertising of cigarettes on
television and radio allowed the introduction and television advertising
of small cigars, which look and smoke much like cigarettes. Small cigar
consumption increased rapidly until these ads were also banned from
television and radio in 1973, and cigar consumption then began a steady
decline lasting almost 20 years. Marketing approaches to cigar sales linking
cigar smoking to wealth and success as portrayed in magazines such as Cigar
Aficionado, and utilizing events such as cigar nights at popular restaurants,
gained widespread prominence beginning in 1992. Sales of cigars, particularly
large cigars, have increased substantially since that time. Accompanying this
marketing has been the suggestion that cigars, particularly premium cigars,
have minimal if any disease risk associated with their use as long as they are
used in “moderation” (Shanken, 1997).
The recent change in tobacco use raises a number of important public
health questions. What are the disease consequences of cigar smoking? What
is the risk of addiction to nicotine from this form of tobacco use? Are the
marketing practices that underlie this change in cigar consumption resulting
in adolescent use of cigars? What are the risks of environmental tobacco
smoke exposure from cigar smoking?
DISEASE RISKS The smoke from both cigars and cigarettes is formed largely from the
incomplete combustion of tobacco, and therefore it comes as no surprise
that cigar smoke is composed of the same toxic and carcinogenic constituents
found in cigarette smoke (Chapter 3). Cigars have more tobacco per unit;
and correspondingly, take longer to smoke and generate more smoke per unit.
Additionally, the lower porosity of cigar wrappers results in more of carbon
monoxide per gram of tobacco burned; and the higher nitrate content of cigar
tobacco results in higher concentrations of nitrogen oxides, carcinogenic
N-nitrosamines and ammonia. When bioassayed in animals, the tar of cigar
smoke is more carcinogenic than cigarette smoke tar (Davies and Day, 1969).
There is little evidence from what is known about the tobacco content and
manufacture of premium cigars to suggest that they are less hazardous than
other cigars. Clearly, cigar smoke is as, or more, toxic and carcinogenic than
cigarette smoke; and differences in disease risks produced by using cigarettes
and cigars relate more to differences in patterns of use, and differences in
inhalation, deposition and retention of cigarette and cigar smoke than to
the differences in smoke composition.
The similarities of cigar and cigarette smoke suggest that similar patterns
of diseases should occur among individuals with similar intensities and
durations of smoke exposure. When cigar smokers who have never used
other tobacco products are compared to individuals who have never used
any tobacco product, a clear pattern of excess disease emerges that can be
related to the frequency of cigar use and the pattern of inhalation (Chapter 4).
Demonstration of a close association between the intensity of cigar smoke
exposure and rates of excess disease provide compelling evidence for
a causal association between cigar smoking and disease occurrence. Most
of the cancers caused by cigarette smoking occur at increased rates among

Chapter 1
4
regular cigar smokers. Cigar smokers who inhale deeply, particularly those
who smoke several cigars per day, have higher rates of coronary heart disease
and chronic obstructive pulmonary disease (COPD).
Figure 2 presents mortality ratios (ratio of the death rate in smokers
compared to never smokers) among male cigar and cigarette smokers for some
of the diseases associated with cigarette smoking. The ratios presented are for
smokers of all numbers of cigarettes or cigars combined. The mortality data
were derived from the American Cancer Society Cancer Prevention Study I
(CPS-I) a twelve year follow-up of over 1 million men and women (Garfinkel,
1985). These data were provided by the American Cancer Society and define
relative risks for those who have smoked exclusively cigars and those who have
smoked exclusively cigarettes, with each group of smokers being compared to
those who have never smoked any tobacco product. All of these mortality
ratios, except those for COPD, are statistically significantly increased among
cigar smokers (Chapter 4). The figure demonstrates that tobacco smoke
generated by cigars can lead to many of the same diseases produced by tobacco
smoke from cigarettes.
However, the pattern of excess disease risk among cigar smokers is not
identical to that observed in cigarette smokers. Mortality ratios among
cigarette smokers are much higher than those among cigar smokers for
coronary heart disease, COPD and lung cancer. In contrast, mortality ratios
for oral and esophageal cancer are similar among cigarette and cigar smokers.
The mortality ratio for laryngeal cancer is intermediate between these two
patterns. Table 1 presents mortality ratios, and their 95 percent confidence
intervals, for the major causes of excess mortality among cigar smokers. The
risk ratios are presented by number of cigars smoked per day and depth of
inhalation to demonstrate the dose-response relationships evident for cigar
smoking and these diseases; and similar data are presented for cigarette
smokers to allow comparison of the magnitude of the effects.
INHALATION An explanation for the difference in mortality pattern between cigarette
smokers and cigar smokers lies in differences in the depth and likelihood of
inhalation of tobacco smoke between these two groups of smokers. Most
cigarette smokers report inhaling the smoke into their lungs, while over three-
quarters of the males in CPS-I who have only smoked cigars report that they
never inhale (Chapter 4). This difference in inhalation is likely due to the
more acidic pH of cigarette smoke. The smoke of most cigars has an alkaline
pH; and as a result, nicotine contained in the smoke can be readily absorbed
across the oral mucosa without inhalation into the lung (Chapter 3). The
more acidic pH of cigarette smoke produces a protonated form of nicotine
which is much less readily absorbed by the oral mucosa, and the larger
absorptive surface of the lung is required for the smoker to receive his or her
desired dose of nicotine. As a result, cigarette smokers must inhale to ingest
substantial quantities of nicotine, the active agent in smoke, whereas cigar
smokers can ingest substantial quantities of nicotine without inhaling.
Inhalation substantially increases the exposure of lung tissue to tobacco smoke
and increases absorption of many smoke constituents, most notably carbon
monoxide (Turner et al., 1977; Wald et al., 1981).

5
Smoking and Tobacco Control Monograph No. 9
Figure 2
Mortality ratios for tobacco induced diseases among male cigar and cigarette smokers in
comparison with never smokers
1
Coronary
Heart
Disease
3
5
7
15
17
19
9
11
13
21
COPD Lung
Cancer
Laryngeal
Cancer
Oral
Cancer
Esophageal
Cancer
Mortality Ratio
Cigarette Smokers
Data from the 12 year follow-up of CPS I
Primary Cigar Smokers
The oral mucosa is exposed to similar amounts of smoke by those who
do and those who do not inhale deeper into the respiratory tract. In contrast,
the lung is much more heavily exposed in those who inhale; and absorption
of many smoke constituents into the blood is greater among those who
inhale. This difference in exposure to smoke by different tissues is the most
likely explanation for the differences in mortality pattern among cigar and
cigarette smokers. Cigar smokers who do not inhale receive a high smoke
exposure to the mouth and tongue, and smoke constituents in their saliva
are swallowed down their esophagus, producing the observed increased
risks of oral and esophageal cancers. The lung and systemic organs such
as the heart receive much less exposure to smoke constituents in those cigar

Chapter 1
6
Table 1
Mortality ratios, and 95% confidence intervals, for select causes of death in male cigar only vs cigarette only smokers by amount
smoked daily and depth of inhalation Cancer Prevention Study I, 12 year follow-up
Amount Smoked Daily
Cigars per Day Cigarettes per Day
Cause of death Nonsmoker 1-2 cigars 3-4 cigars 5+ cigars <1 pack 1 pack >1 pack
All causes of death 1.0 1.02 1.08 1.17 1.46 1.69 1.88
(.97-1.07) (1.02-1.15) (1.10-1.24) (1.43-1.49) (1.66-1.71) (1.85-1.91)
Cancer of buccal cavity 1.0 2.12 8.51 15.94 5.93 6.85 12.04
& pharynx combined* (0.43-6.18) (3.66-16.77) (8.71-26.75) (4.28-8.02) (5.37-8.62) (9.81-14.63)
Cancer of esophagus 1.0 2.28 3.93 5.19 2.41 4.3 5.6
(0.74-5.33) (1.43-8.55) (2.23-10.22) (1.61-3.46) (3.32-5.48) (4.35-7.10)
Cancer of larynx 1.0 6.46 — 26.03 8.7 25.69 23.59
(0.72-23.27) (8.39-60.74) (4.75-14.59) (18.66-34.48) (17.33-31.37)
Cancer of lung 1.0 0.99 2.36 3.40 6.75 12.86 20.23
(0.54-1.66) (1.49-3.54) (2.34-4.77) (6.18-7.37) (12.14-13.60) (19.20-21.30)
Cancer of pancreas 1.0 1.18 1.51 2.21 1.69 2.17 2.41
(0.69-1.89) (0.86-2.45) (1.40-3.32) (1.41-2.00) (1.89-2.47) (2.08-2.77)
COPD 1.0 1.39 1.78 1.03 8.86 12.51 15.04
(0.74-2.38) (0.89-3.18) (0.37-2.23) (7.96-9.84) (11.48-13.60) (13.73-16.45)
Coronary heart disease 1.0 0.98 1.06 1.14 1.4 1.58 1.65
(0.91-1.07) (0.96-1.16) (1.03-1.24) (1.36-1.45) (1.54-1.62) (1.60-1.69)

7
Smoking and Tobacco Control Monograph No. 9
Table 1
(continued)
Self-Reported Depth of Inhalation
Cigars Cigarettes
Cause of death Nonsmoker None Slight Moderate to Deep None, Slight Moderate Deep
All causes of death 1.0 1.04 1.19 1.6 1.54 1.65 1.9
(1.00-1.08) (1.09-1.30) (1.38-1.84) (1.50-1.57) (1.63-1.67) (1.86-1.94)
Cancer of buccal cavity 1.0 6.98 7.83 27.88 6.26 8.43 12.48
& pharynx combined* (4.13-11.03) (1.57-22.88) (5.60-81.46) (4.47-8.53) (7.00-10.06) (9.61-15.94)
Cancer of esophagus 1.0 3.4 1.9 14.84 2.94 4.06 4.95
(1.90-5.61) (0.02-10.58) (2.98-43.37) (1.97-4.23) (3.30-4.94) (3.55-6.72)
Cancer of larynx 1.0 10.6 — 53.26 22.19 13.49 27.54
(3.87-23.07) (0.70-296.32) (14.74-32.07) (10.01-17.78) (18.44-39.56)
Cancer of lung 1.0 1.97 1.89 4.93 9.33 13.13 17.11
(1.48-2.57) (0.81-3.72) (1.80-10.72) (8.61-10.10) (12.53-13.75) (16.00-18.28)
Cancer of pancreas 1.0 1.55 2.16 2.26 1.99 2.01 2.38
(1.12-2.07) (0.99-4.10) (0.45-6.60) (1.66-2.36) (1.79-2.25) (1.98-2.83)
COPD 1.0 1.09 2.05 4.52 8.8 12.28 16.07
(0.66-1.70) (0.66-4.77) (0.91-13.22) (7.85-9.85) (11.42-13.18) (14.49-17.78)
Coronary heart disease 1.0 1.01 1.23 1.37 1.45 1.52 1.71
(0.96-1.07) (1.07-1.41) (1.07-1.75) (1.41-1.50) (1.49-1.55) (1.66-1.76)
*excludes salivary gland

Chapter 1
8
smokers who do not inhale; and correspondingly, non-inhaling cigar
smokers have lower rates of coronary heart disease, COPD and lung cancer
than inhaling cigar smokers or cigarette smokers. The larynx, which
connects the lung and oral cavity, has a pattern of disease intermediate
between that of the lung and the mouth.
The importance of dose and inhalation for lung cancer risk among cigar
smokers are presented in Figure 3 where modeled lung cancer risk data from
CPS-I for cigar smokers of different numbers of cigars per day and different
patterns of inhalation are compared to the risks for a one pack per day
cigarette smoker (Chapter 4). When cigar smokers don’t inhale or smoke
few cigars per day, the risks are only slightly above those of never smokers.
Risks of lung cancer increase with increasing inhalation and with increasing
number of cigars smoked per day, but the effect of inhalation is more
powerful than that for number of cigars per day. When 5 or more cigars
are smoked per day and there is moderate inhalation, the lung cancer risks
of cigar smoking approximate those of a one pack per day cigarette smoker.
As the tobacco smoke exposure of the lung in cigar smokers increases to
approximate the frequency of smoking and depth of inhalation found in
cigarette smokers, the difference in lung cancer risks produced by these
two behaviors disappears.
The claim has been made that cigar smokers who smoke few cigars or
do not inhale have no increased risk of disease (Shanken, 1997). A more
accurate statement would be that the risks experienced by cigar smokers
are proportionate to their exposure to tobacco smoke.
Among regular cigar smokers who had never smoked cigarettes in the
CPS-I study and who did not inhale, statistically significant increased risks
for cancers of the lung, oral cavity, larynx, pancreas and esophagus are
observed (Chapter 4). Risks for coronary heart disease are significantly
elevated only for smokers of 3 or more cigars per day or those who inhale.
Relative risks for COPD increase with increasing inhalation, but the risks
do not reach statistical significance for the CPS-I data. It should also be
noted that increased risks of lung cancer and heart disease have been
reported for nonsmokers at levels of tobacco smoke that occur with
environmental tobacco smoke exposure (EPA, 1992; Cal EPA, 1997).
Risks among occasional cigar smokers are difficult to measure because
of the wide variability in frequency of smoking among occasional cigar
smokers and the marked variation in the amounts of tobacco contained
in different cigars. However, it is reasonable to assume that the risks for
occasional cigar smokers lie somewhere between those for individuals whose
only exposure to tobacco smoke is environmental tobacco smoke and those
of regular cigar smokers. As occasional cigar smokers smoke more frequently
or inhale more deeply, their exposure to tobacco smoke increases, and with
that increased exposure comes a proportionate increase in disease risks.

9
Smoking and Tobacco Control Monograph No. 9
Figure 3
Lung cancer death rates for cigar smokers with different patterns of inhalation and number of cigars per day compared with one
pack per day cigarette smokers
200
400
600
800
1,000
Lung Cancer Death Rate per 100,000
PYO
1,200
20 cigarettes/day, initiation at age 18
0
45
50
55
60
65
Age
70
75
80
85
5+ cigars/day, moderate inhalation
3-4 cigars/day, moderate inhalation
5+ cigars/day, no inhalation
never smoker

Chapter 1
10
The relationship of cigar smoking and alcohol consumption, particularly
for oral cancers, has not been evaluated; but the established interaction
between cigarette smoking and alcohol consumption for oral cancers and
the frequent association of cigar smoking with alcohol consumption raise
the question of an increased risk from the combination of these two
behaviors.
Cigarette Smokers As described earlier, a number of cigarette smokers may have
Who Switch to switched to cigars in response to health warnings following
Cigars release of the first Surgeon General’s Report in the belief that
smoking cigars resulted in a lower disease risk (Chapter 2). Data from the
CPS-I study demonstrate the limitations of this approach to risk reduction.
Cigar smokers who have previously been cigarette smokers report higher
rates of inhalation of tobacco smoke than do cigar smokers who have never
smoked cigarettes (Chapter 4). These former cigarette smokers also have
higher rates of most smoking induced diseases in CPS-I than do cigar smokers
who have never smoked cigarettes, and their rates remain above those for
smokers who stop using all tobacco products (Higgins et al., 1988). It is not
possible to define the independent contributions of their past cigarette
smoking and current cigar smoking behaviors with regard to these disease
risks, but it is clear that the risks remain above those for cigar smokers who
have never smoked cigarettes. Existing data suggest that any reductions in
disease risks that accompany switching from smoking cigarettes to smoking
cigars are conditional on a reduction in exposure to tobacco smoke with
the change in tobacco product smoked. Individuals who have previously
smoked cigarettes are more likely to inhale cigar smoke when they switch to
smoking cigars, and this increased inhalation may reduce or eliminate any
risk reduction with the change from cigarettes to cigars, particularly if cigars
are smoked daily or as a means of satisfying an addiction to nicotine.
Risks Among Almost all of the disease risk data for cigar smoking are based on
Women observations among males, but it is reasonable to assume that risks
among females would also be proportionate to the intensity and duration
of their exposure. In several European countries where women have smoked
cigars for many years, it appears that the risks for smoking related diseases
are similar for male and female cigar smokers. The lower prevalence and
frequency of use among females in the U.S. would be expected to translate
into lower rates of chronic disease due to cigar smoking in the female
population, particularly given the long duration of use required to produce
these diseases. However, cigarette smoking among women has been shown to
increase the fetal and maternal complications of pregnancy (USDHHS, 1990),
and these complications result from smoking during the comparatively short
duration of the pregnancy. Data on the risks of cigar smoking during
pregnancy are not sufficient to define the risks, but there is no reason to
expect that cigar smoke would be any less toxic for the mother or fetus.
Regular cigar smoking, particularly with inhalation, should be presumed to
have risks similar to that of cigarette smoking for the pregnant smoker.

11
Smoking and Tobacco Control Monograph No. 9
NICOTINE Cigars can deliver nicotine to the smoker in concentrations comparable
ADDICTION to those delivered by cigarettes and smokeless tobacco (Chapter 6).
However, the alkaline pH of cigar smoke, and the tendency of cigar smokers
not to inhale, result in the nicotine being absorbed predominantly across the
oral mucosa rather than in the lung. This route of absorption leads to a slower
rise and lower peak of the arterial levels of nicotine delivered to the brain
compared to the absorption that occurs across the alveolar-capillary surface of
the lung in most cigarette smokers. The rapidity of absorption and rate of rise
in arterial nicotine levels may be important determinants of the potential for
nicotine ingestion to lead to addiction (Jasinski et al., 1984). However, nicotine
absorbed across the oral mucosa is capable of forming a powerful addiction
as demonstrated by the large number of individuals addicted to smokeless
tobacco (USDHHS 1988); and cigar smoke can be inhaled into the lung where
it would be absorbed as readily as cigarette smoke
ADULT USE The pattern of use of cigars also sheds some light on the addictive nature
of cigar smoking in comparison with other forms of tobacco use, at least for
adults. The fraction of adult cigar smokers who smoke cigars every day is
much smaller than the fraction of cigarette or smokeless tobacco users who
use every day (Chapter 2). This suggests that cigar smoking among adults,
while probably able to cause addiction to nicotine, is less likely to do so than
cigarette smoking or smokeless tobacco use. Data from California, which
show that the recent change in cigar use among adults is largely an increase
in occasional use, also suggests that the addictive potential of cigars is lower
than that for cigarettes (Gerlach et al., 1998).
Whatever reassurance is provided by the largely occasional use of cigars
among adults must be tempered by spread of this behavior among groups
who have traditionally had low rates of cigarette use. The prevalence of
current cigar and cigarette smoking by income level for adult males in
California is presented in Figure 4, and it is apparent that the recent increase
in cigar smoking is largely among the affluent in contrast to the marked
decline in cigarette smoking that occurs with increasing income (Chapter 2).
A similar picture is evident with educational attainment, with the highest rates
of cigar use and lowest rates of cigarette use occurring among those with the
highest educational attainment. Increasing numbers of women, who
historically have had very low rates of cigar use, are also currently smoking
cigars.
The spread of cigar smoking into groups with low rates of cigarette use
is accompanied by a dramatic increase in cigar use among never smokers.
Among adult California males in 1996, forty percent of current cigar smokers
have smoked less than 100 cigarettes in their entire life which is the definition
typically used to define a never smoker.
Increasing cigar use among upper income and educational level adults
raises concern that the success in reducing smoking among these groups may
be at risk of reversal. This may be particularly true if the use of cigars by these
groups enhances the norms created by cigar marketers that portray cigar use as
a socially acceptable, sophisticated and relatively safe behavior. Anecdotal

Chapter 1
12
Figure 4
Prevalence of current cigarette and cigar smoking among California males of different
incomes, 1996
0
<=10,000
5
10
15
20
25
30
10,001-
20,000
20,001-
30,000
30,001-
50,000
Income
50,001-
75,000
75,000+
Percent
Cigars
Cigarettes
observation suggests that cigars are currently smoked in situations where
cigarette smokers are reluctant to light up, a marked reversal of the norm
banning cigar smoking even in environments where cigarette smoking was
allowed.
Use of cigars by adults who have never used cigarettes, or by former
cigarette smokers, raises a concern that use of cigars and the nicotine
ingestion that accompanies cigar smoking may lead to cigar smokers
initiating or relapsing to cigarette smoking. The fraction of tobacco used as
cigarettes expanded rapidly in the early years of this century at the expense
of pipes, cigars and smokeless tobacco, in part because cigarettes were a
convenient method of getting a rapid intense dose of nicotine in a short
interval of time (Burns et al., 1997). The potential for current cigar smokers
to begin seeking the psychoactive effects of nicotine on a more regular basis
through the more convenient form of a cigarette is a real risk based on our

13
Smoking and Tobacco Control Monograph No. 9
historical experience with these two tobacco products. Concern about relapse
to cigarette smoking by former cigarette smokers who start smoking cigars is
heightened by the observation in California adults that among those who
were former cigarette smokers one year ago, cigar smokers are twice as likely
to have relapsed to smoking cigarettes as former cigarette smokers who do not
use cigars (Chapter 2). This observation does not separate the likelihood that
cigar smoking leads to relapse of cigarette smoking from the possibility that
relapsing cigarette smokers take up smoking cigars as well, but it raises
a concern that cigar use may place former cigarette smokers at risk of relapse.
Of equal concern is the observation that the fraction of male adult
never smokers who began smoking cigarettes in the last two years is over
two times higher among current cigar smokers than among those who don’t
smoke cigars (Chapter 2). Again, it is impossible to separate the likelihood of
cigar smoking leading to initiation of cigarette smoking from the possibility
that those who initiate cigarette smoking are also likely to smoke cigars; but
the commonality in both of these behaviors is nicotine ingestion, and it
would not be surprising if use of cigars predisposed an individual to the use of
cigarettes.
ADOLESCENT Data on cigar use among adolescents is also alarming (Chapter 2).
USE Few data on past adolescent cigar use are available, largely because
it was a behavior felt to be uncommon enough not to be worthy of
examination until recently. However, several recent surveys of adolescents
show a substantial fraction of both male and female adolescents who report
both ever and current use of cigars (CDC, 1997a; Chapter 2). Male cigar
smoking prevalence still exceeds that for females among adolescents, but the
gender difference is less than for adults. Table 2 presents the prevalence of
cigar use among adolescents in Massachusetts by educational grade level,
and it is clear that there is a substantial level of cigar use, even prior to high
school.
Addiction to nicotine is a process that occurs almost exclusively during
adolescence and young adulthood (USDHHS, 1994). The age of initiation of
cigar smoking, prior to the recent increase in cigar use, was much older than
that for cigarette smoking (Chapter 2); and this difference in age of initiation
may be partially responsible for the lower addictive potential of cigars, as
manifest by the high rate of occasional, as compared to daily, cigar smoking
among adults. Now that initiation of cigar smoking is common among
adolescents, whatever resistance to addiction is offered by an older age of
initiation would be expected to disappear. The reassurance provided by the
low rate of daily cigar smoking among adults may be illusionary now that
initiation of cigar smoking is extending into those age groups where
development of addiction to nicotine is common. Several generations of
adolescents have become addicted to tobacco products that allow nicotine
to be absorbed through the lung (cigarettes) and to tobacco products that
allow nicotine to be absorbed through the oral mucosa (smokeless tobacco).
Cigars can deliver nicotine through both of these routes, and large numbers
of adolescents are currently being exposed to nicotine through use of cigars.
It is premature to conclude that current generations of adolescents who are

Chapter 1
14
Table 2
Prevalence of cigar use in the last year, and all forms of tobacco use in the last 30 days by
school grade, Massachusetts, 1996
Grade
6 7 8 9 10 11 12
Past Year Use 5.0 8.3 20.3 20.6 29.6 31.8 31.3
of Cigars (4.2-5.8) (6.6-10.0) (17.7-22.9) (18.1-23.1) (26.9-32.3) (28.7-34.8) (28.2-34.4)
Past 30-Day Use 2.0 4.4 10.9 10.4 16.0 18.4 13.4
of Cigars (1.1-2.9) (1.3-7.5) (8.9-12.9) (8.5-12.3) (13.8-18.2) (15.9-20.9) (11.0-15.8)
Males
Cigarettes 10.7 13.7 24.6 27.2 32.2 35.5 45.1
(8.0-13.4) (10.7-16.7) (20.8-28.4) (23.2-31.2) (28.3-36.1) (31.0-40.0) (40.3-49.9)
Smokeless 2.6 2.5 5.7 4.4 10.9 14.3 13.6
(1.2-4.0) (1.2-3.8) (3.7-7.7) (2.5-6.3) (8.3-13.5) (11.0-17.6) (10.3-16.9)
Cigars 3.2 4.3 13.0 14.9 24.9 30.3 23.7
(1.6-4.8) (2.6-6.0) (10.0-16.0) (11.7-18.1) (21.3-28.5) (25.9-34.7) (19.6-27.8)
Females
Cigarettes 5.7 19.0 27.5 33.0 35.3 42.0 36.6
(3.7-7.7) (15.5-22.5) (23.3-31.7) (29.1-36.9) (31.1-39.5) (37.6-46.4) (32.2-41.0)
Smokeless 0.1 0.2 0.8 1.3 1.2 0.5 0.6
(-0.8-1.0) -0.2-0.6) (0.0-1.6) (0.4-2.2) (0.2-2.2) (-0.1-1.1) (-0.1-1.3)
Cigars 0.8 4.6 8.4 6.6 6.1 7.7 4.1
(-1.5-3.1) (2.7-6.5) (5.8-11.0) (4.5-8.7) (4.0-8.2) (5.3-10.1) (2.3-5.9)
ingesting nicotine from cigars will not become addicted simply because older
generations of cigar smokers, who began smoking as adults, were less likely to
become addicted.
Current cigarette smoking prevalence rates among adults have remained
relatively unchanged over the last few years (CDC, 1997b), ending four
decades of decline in prevalence; and the prevalence of cigarette smoking
among adolescents has increased recently (CDC, 1996). The contribution
of increasing cigar use among both adults and adolescents to these trends
remains unexplored, but the temporal association of these two phenomena
suggests that it should be a high priority for future investigation.
MARKETING Recent marketing efforts have promoted cigars as symbols of a luxuriant
and successful lifestyle. Endorsements by celebrities including athletes,
elaborate cigar smoking events and the resurgence of cigar smoking in movies
have all contributed to the increased visibility of cigar smoking in society
and probably have lowered barriers to cigar use in public. Publication of cigar
lifestyle magazines such as “Cigar Aficionado”, which began in 1992, antedate

15
Smoking and Tobacco Control Monograph No. 9
the increase in cigar consumption which began in 1993. Linkage of cigar
smoking to an opulent and powerful lifestyle, and the featuring of highly
visible women smoking cigars, is a core element of cigar promotion; and
it has been successful in increasing cigar consumption among men and
initiating cigar smoking as a behavior among women (Chapter 7).
Evaluation of the effects of cigar promotional efforts on adolescent cigar
smoking is only just beginning due to the recent nature of this phenomenon,
but cigars are not the first tobacco product to be heavily promoted in ways
likely to influence adolescent use. Celebrity endorsements by popular
heroes, including athletes, were a prominent part of the mass marketing
of cigarettes during the first half of this century (Kluger, 1996).
By the late 1940’s and early 1950’s, print and television advertising
commonly featured athletes and movie stars describing the pleasures of
smoking individual brands of cigarettes (Figure 5). The individuals portrayed
here are only a tiny fraction of those who endorsed cigarette smoking. In
response to the concern about the disease consequences of smoking, the
tobacco industry adopted a voluntary code of advertising during the mid
1960’s that prohibited the use of endorsements by athletes and other
celebrities perceived to appeal to youth (USDHHS, 1994). Denied celebrity
Figure 5
Popular sport figures in tobacco advertisements circa 1940’s-1960’s

Chapter 1
16
endorsement in their advertising, the cigarette companies developed lifestyle
and image related advertising, most notably the Marlboro cowboy and
“Smooth Joe Camel” ads that have allowed these two brands to capture the
majority of adolescent smokers (CDC, 1994). Virginia Slims advertisements
linked cigarette smoking to independence and power as well as to thinness.
Cigarette promotion through events like the Cool Jazz Festival and Formula
One auto racing linked cigarettes to a glamorous and exciting lifestyle, while
sponsorship of cultural events linked cigarettes to sophistication and
provided borrowed credibility. One outcome of these marketing approaches
is that the overwhelming majority of cigarette smokers begin smoking, and
become addicted, during adolescence (USDHHS, 1994).
Intensive marketing of smokeless tobacco began in the 1970’s and
was followed by a dramatic rise in use of these products (USDHHS, 1993).
Smokeless tobacco products were marketed then, as cigars are being marketed
now, despite strong scientific evidence that they cause disease. The
difference in risk between the enormous risks of cigarette smoking and the
more moderate risks of smokeless tobacco and
cigar use is touted to reassure the users that the
products “used in moderation” have little risk. At
the same time, advertising in the print media and
on television (where cigarette advertising was
banned) featured endorsements by celebrities and
athletes, and smokeless tobacco promoted lifestyle
and image related events that linked smokeless
tobacco use with rodeo and auto racing. Once
again, adolescent males responded to these
promotional approaches; and it was
only after a generation of young males became
addicted to smokeless tobacco that endorsement
by athletes was discontinued because of its appeal
to youth. Again, the advertisement for smokeless
tobacco portrayed here (Figure 6) represents only
a few of the athletes that promoted smokeless tobacco use.
Having twice demonstrated that image related advertising
and celebrity endorsement could create a new market for little
used tobacco products, it should not be surprising that those
involved in the cigar trade would utilize the same approaches.
The use of celebrities like Demi Moore and Arnold
Schwarzenegger (Figure 7) to endorse cigar smoking along
with the images of Michael Jordan and Madonna smoking
cigars are an important part of creating a lifestyle image for
cigar use (Chapter 7). Athletes are also once again endorsing
cigar use including such prominent super stars as Wayne
Gretzky (Figure 8). Having demonstrated the success of this
approach in influencing adolescent tobacco use twice in this
century, we should not be surprised by the current high rates
of cigar use among adolescent males and females.
Figure 7
Figure 6

17
Smoking and Tobacco Control Monograph No. 9
The use of endorsements to allay health fears associated
with cigar smoking is also as old as the Camel Campaign that
touted “More doctors smoke Camels”. The eerie similarity of
two quotes sixty years apart in time make the point that the
message of reassurance is the same, it is only the product that is
different.
“For a good sense of deep-down contentment – just give
me Camels. After a good man-sized meal, that little phrase
‘Camels set you right’ covers the way I feel. Camels set me
right whether I’m eating, working – or just enjoying life. All
the years I’ve been playing, I’ve been careful about my physical
condition. Smoke? I smoke and enjoy it. My cigarette is a
Camel.”
Baseball Legend Lou Gehrig, The Saturday Evening Post of April 24, 1937
“The enjoyment of a cigar after a hard week gives me a feeling
of well-being and relaxation that a Valium could not match.
While there may be a more ideal form of stress reduction, I haven’t
yet discovered anything else as effective and easy”
Ear Nose and Throat Surgeon M. Hal Pearlman, M.D., Cigar Aficionado,
Spring 1993
Marketing a product is intended to increase the use of the
product, and it is probably naïve to assume that cigar manufacturers
would not adopt marketing approaches proven to increase the use
of other tobacco products, absent a regulatory prohibition. The
“intent” of the marketers may be to reach adults, but it is hard to
ignore the fact that twice before in this century this same “intent”
to reach adults has grabbed children.
ENVIRONMENTAL One highly visible approach to cigar marketing has been the
TOBACCO SMOKE cigar smoking event. These events commonly include meals
and entertainment, and are marketed as a means of experiencing fine cigars
(Chapter 7). Individuals attending these events may smoke cigars only at the
event and may smoke only a few cigars per year. However, employees who
work these events, and who are exposed to the environmental tobacco smoke
generated at them, may have much more frequent exposure. These events,
and the re-emergence of cigar smoking in public areas frequented by
nonsmokers, raise the question of the contribution of cigar smoking to
environmental tobacco smoke (ETS) exposure.
Comparison of the contribution of cigarettes and cigars to ETS requires
consideration of three issues: Differences in the composition of cigarette and
cigar smoke, differences in the emission rates per minute between cigarettes
and cigars, and differences in the mass of tobacco burned (and corresponding
duration of smoking) between cigars and cigarettes. Tobacco smoke produced
by cigars contains most of the same toxic and carcinogenic constituents found
in cigarette smoke (Chapter 3). There is marked variation in the relative
Figure 8

Chapter 1
18
concentrations of these constituents present in cigar smoke across different
types and sizes of cigars. In general however, large cigars produce more
carbon monoxide, as well as higher amounts of nitrogen oxides and
carcinogenic N-nitrosamines, per gram of tobacco burned, and the free
ammonia in tobacco smoke is higher due to the more alkaline pH of the
smoke (Chapter 3). It is likely this difference in free ammonia that results
in the more pungent smell of cigar smoke.
Cigars generate slightly lower amounts of respirable suspended
particulates (RSP) per minute compared to cigarettes (Chapter 5), but
somewhat higher amounts of carbon monoxide (CO). The major difference
between cigarettes and cigars is the amount of tobacco contained in each
product. Cigarettes generally contain less than one gram of tobacco and are
smoked for about 7-8 minutes, with a substantial interval between cigarettes.
Large cigars commonly contain 5-17 grams of tobacco, and are smoked over
intervals as long as 60-90 minutes. Thus cigars, while generating similar
amounts of ETS per minute compared to cigarettes, continue generating
smoke for a much longer period of time; and therefore, the total amount of
ETS generated by a single large cigar is much greater than that by a single
cigarette.
Continued generation of ETS by cigar smoking may be of particular
importance at cigar smoking events where most of the attendees smoke
cigars. It is likely that the number of individuals generating ETS at any point
in time would be higher at these events because of the longer time required
to finish a cigar. The shorter time required to finish a cigarette, and the
interval between cigarettes, would result in fewer individuals smoking at any
point in time.
Concern about increased generation of smoke at cigar events is born out
by measurements of smoke constituents at these events. Levels of CO in the
air at these events are similar to those on a crowded California freeway
(Repace et al., 1998). These data confirm the belief that cigars can contribute
substantial amounts of tobacco smoke to the indoor environment; and,
when large numbers of cigar smokers congregate together in a cigar smoking
event, the amount of ETS produced is sufficient to be a health concern for
those regularly required to work in those environments (Chapter 5).
REGULATION Cigars are treated separately from cigarettes and smokeless tobacco
AND TAXATION for purposes of taxation and often for purposes of regulation.
Traditionally they have been taxed at lower rates, and are not covered by
the currently proposed FDA regulations for tobacco (Chapter 8). In contrast,
cigar smoking was eliminated in airplanes and other locations well ahead
of the time that cigarette smoking was eliminated. More recently, a number
of States have increased the taxes on cigars; but the norms against cigar
smoking in public locations seem to be changing in favor of allowing cigar
smoking in more areas, including areas where cigarette smoking is not
considered acceptable.

19
Smoking and Tobacco Control Monograph No. 9
OVERALL CONCLUSIONS
1. Cigar smoking can cause oral, esophageal, laryngeal and lung cancers.
Regular cigar smokers who inhale, particularly those who smoke several
cigars per day, have an increased risk of coronary heart disease and
chronic obstructive pulmonary disease.
2. Regular cigar smokers have risks of oral and esophageal cancers similar to
those of cigarette smokers, but they have lower risks of lung and laryngeal
cancer, coronary heart disease and chronic obstructive pulmonary
disease.
3. Cigar use in the U.S. has increased dramatically since 1993. Adult
prevalence of cigar use in California has increased predominantly among
occasional cigar smokers. A substantial number of former and never
smokers of cigarettes are currently smoking cigars. In contrast to
cigarettes, much of the increased use of cigars appears to be occurring
among those with higher incomes and greater educational attainment.
4. Adolescent cigar use is occurring at a substantial level and is currently
higher that that recorded for young adults prior to 1993. Currently, cigar
use among adolescent males exceeds the use of smokeless tobacco in
several states. This use is occurring among both males and females.
REFERENCES
Burns D., Lee L., Shen Z., Gilpin B., Tolley D.,
Vaughn J. and Shanks T. Cigarette Smoking Behavior
in the United States (Chapter 2). In: Changes in
Cigarette-Related Disease Risks and Their
Implication for Prevention and Control,
Monograph No. 8, Burns D., Garfinkel L. and
Samet J., Editors, USDHHS NIH NCI, Bethesda, MD,
U.S. Department of Health and Human Services,
National Institutes of Health, NIH Publication
#97-4213, pp␣ 13-112, 1997.
California Environmental Protection Agency.
Health Effects of Exposure to Environmental
Tobacco Smoke. California Environmental
Protection Agency, 1997.
CDC Changes in the Cigarette Brand Preferences of
Adolescent Smokers — United States, 1989— 1993.
MMWR 1994 43(32): 577-581, 1994.
CDC Tobacco Use and Usual Source of Cigarettes
Among High School Students — United States,
1995. MMWR, 45(20): 413-418, 1996.
CDC Cigar smoking among teenagers—United States,
Massachusetts and New York, 1996. MMWR
46(20): 433-440, 1997a.
CDC Cigarette Smoking Among Adults—United
States, 1995. MMWR, 46(51): 1217-1220, 1997b.
Connolly, G.N. Policies Regulating Cigars (Chapter 8).
In: Cigars: Health Effects and Trends, Monograph
No. 9. Burns D., Cummings, K. M., Hoffmann, D.,
Editors, USDHHS NIH NCI, Bethesda, MD, U.S.
Department of Health and Human Services,
National Institutes of Health, 1998.
Davies, R.F., Day. T.D. A study of the comparative
carcinogenicity of cigarette and cigar smoke
condensate on mouse skin. British Journal of Cancer
23:363-368, 1969.
Environmental Protection Agency. Respiratory
Health Effects of Passive Smoking: lung cancer and
other disorders. Environmental Protection Agency
EPA/600/6-90/006F, 1992.
Fant, R.V., Henningfield, J.E. Pharmacology and Abuse
Potential of Cigars (Chapter 6). In: Cigars: Health
Effects and Trends, Monograph No. 9. Burns D.,
Cummings, K. M., Hoffmann, D., Editors,
USDHHS NIH NCI, Bethesda, MD, U.S.
Department of Health and Human Services,
National Institutes of Health, NIH Publication,
1998.
Garfinkel, L. Selection, Follow-up, and Analysis in
the American Cancer Society Prospective Studies.
National Cancer Institute Monograph 67:49–52,
1985.
Gerlach, K.K., Cummings, K.M., Hyland, A., Gilpin,
E. A., Johnson, M. D., Pierce, J. P. Trends -in Cigar
Consumption and Smoking Prevalence
(Chapter 2). In: Cigars: Health Effects and Trends,
Monograph No. 9. Burns D., Cummings, K. M.,
Hoffmann, D., Editors, USDHHS NIH NCI,
Bethesda, MD, U.S. Department of Health and
Human Services, National Institutes of Health,
NIH Publication, 1998.

Chapter 1
20
Higgins, I.T.T., Mahan, C.M., Wynder, E.L. Lung
cancer among cigar and pipe smokers. Preventive
Medicine 17:116-128, 1998.
Hoffmann, D., Hoffmann, I. Chemistry and Toxicology
(Chapter 3). In: Cigars: Health Effects and Trends,
Monograph No. 9. Burns D., Cummings, K. M.,
Hoffmann, D., Editors, USDHHS NIH NCI, Bethesda,
MD, U.S. Department of Health and Human
Services, National Institutes of Health, NIH
Publication, 1998.
Jasinski, D. R., Johnson, R. E., Henningfield, J. E. Abuse
liability assessment in human subjects. Trends in
Pharmacological Science, 5: 196-200, 1984.
Kluger, R. Ashes to ashes: America’s hundred-year
cigarette war, the public health, and the unabashed
triumph of Philip Morris. New York: Alfred A.
Knopf, 1996.
Repace, J.L., Ott, W.R., Klepeis, N.E. Indoor Air Pollution
from Cigar Smoke (Chapter 5). In: Cigars: Health
Effects and Trends, Monograph No. 9. Burns, D.,
Cummings, K. M., Hoffmann, D., Editors, USDHHS
NIH NCI, Bethesda, MD, U.S. Department of Health
and Human Services, National Institutes of Health,
NIH Publication, 1998.
Shanken M.R. Scare Tactics. Cigar Aficionado 5 (4):19,
1997.
Shanks T, Burns D. Disease Consequences of Cigar
Smoking (Chapter 4). In: Cigars: Health Effects and
Trends, Monograph No. 9. Burns D., Cummings, K.
M., Hoffmann, D., Editors, USDHHS NIH NCI,
Bethesda, MD, U.S. Department of Health and
Human Services, National Institutes of Health,
NIH Publication, 1998.
Slade, J. Marketing and Promotion of Cigars (Chapter 7).
In: Cigars: Health Effects and Trends, Monograph
No. 9. Burns D., Cummings, K. M., Hoffmann, D.,
Editors, USDHHS NIH NCI, Bethesda, MD, U.S.
Department of Health and Human Services,
National Institutes of Health, NIH Publication,
1998.
Turner, J.A., Sillett, R.W., McNicol, M.W.
Effect of cigar smoking on carboxyhemoglobin and
plasma nicotine concentrations in primary pipe and
cigar smokers and in cigarette smokers. British
Medical Journal 2:1387-1389, 1997.
U.S. Department of Agriculture. Tobacco Situation
and Outlook Report. U.S. Department of
Agriculture, Economic Research Service, series
TBS-239, September 1997.
USDHHS The Health Consequences of Smoking:
Nicotine Addiction: A Report of the Surgeon
General, U.S. Department of Health and Human
Services, Public Health Service, Centers for Disease
Control, Office on Smoking and Health. (DHHS
publication No. [CDC] 88-8406). Washington DC:
U.S. Government Printing Office, 1988.
USDHHS Smokeless Tobacco or Health, Smoking and
Tobacco Control Monograph No. 2, Stotts R.C.,
Schroeder K.L., D., and Burns D., Editors, USDHHS
NIH NCI, Bethesda, MD, U.S. Department of Health
and Human Services, National Institutes of Health,
NIH Publication No. 93-3461, 1993.
USDHHS The Health Benefits of Smoking Cessation.
US Dept of Health and Human Services, Public
Health Service, Centers for Disease Control, Office
on Smoking and Health. DHHS Publication No
(CDC) 90-8416, 1990.
USDHHS Preventing Tobacco Use Among Young
People: A Report of the Surgeon General. Atlanta,
GA: US Department of Health and Human Services,
Public Health Service, Centers for Disease Control
and Prevention, National Center for Chronic
Disease Prevention and Health Promotion, Office
on Smoking and Health, 1994.
Wald, N.J., Idle, M., Boreham, J., Bailey, A.
Carbon monoxide in breath in relation to smoking
and carboxyhemoglobin levels. Thorax 36:366-369,
1981.

21
Trends in Cigar Consumption and Smoking Prevalence
Trends in Cigar Consumption
and Smoking Prevalence
Karen K. Gerlach, K. Michael Cummings, Andrew Hyland, Elizabeth A. Gilpin,
Michael D. Johnson, and John P. Pierce
INTRODUCTION The use of cigars appears to be on the increase in the United States
based on reports in the popular press and the emergence of cigar bars and cigar
events (Chapter 7). This chapter examines trends in cigar smoking prevalence
and patterns of cigar use. Data on cigar sales are examined to assess overall
trends in cigar use, while national and regional survey data on self-reported cigar
use are used to evaluate changing patterns of cigar use among different age,
gender, and racial groups.
Trends in Cigar Figure 1 depicts tobacco consumption in the United States by major
Production, Sales, product category for the period 1880 through 1997 (Milmore and
and Consumption Conover, 1956; U.S. Department of Agriculture, 1996, 1997). These
data are expressed in pounds of tobacco consumed per adult rather than in
individual units such as cigars or cigarettes, so that direct comparisons between
product categories can be made. Cigars accounted for a larger percentage of
overall tobacco consumption in the early decades of the twentieth century than
they do currently. By the mid-1920’s, cigar consumption began to decline as
cigarettes became the predominant form of tobacco consumed. Cigar
consumption increased slightly in the early 1950’s and again in the mid-1960’s,
possibly as a result of male cigarette smokers switching to cigars in response to
publicity about the health dangers of cigarettes.
From 1964 until 1993, cigar consumption declined by 66 percent in the
United States (U.S. Department of Agriculture, December 1996), however
between 1993 and 1997, overall cigar consumption increased nearly 50 percent.
The recent upturn in cigar smoking since 1993 is due mainly to an increase in the
sale of large cigars, which increased by 68 percent from 1993 to 1997 (Table 1).
Despite the recent growth in cigar sales, cigars still constitute only a small
fraction of the tobacco market in comparison with other tobacco products.
Figure 2 summarizes consumption data for United States of large cigars and
cigarillos and small cigars between 1950 and 1997 (U.S. Department of
Agriculture, September 1997). Before 1971, small cigars made up only a tiny
fraction of cigar sales. However, the sale of small cigars increased by 254 percent
between 1971 and 1972 (U.S. Department of Agriculture, December 1996) in
conjunction with an increase in television advertising. The increased television
advertising resulted from a loophole in the federal law (The Public Health
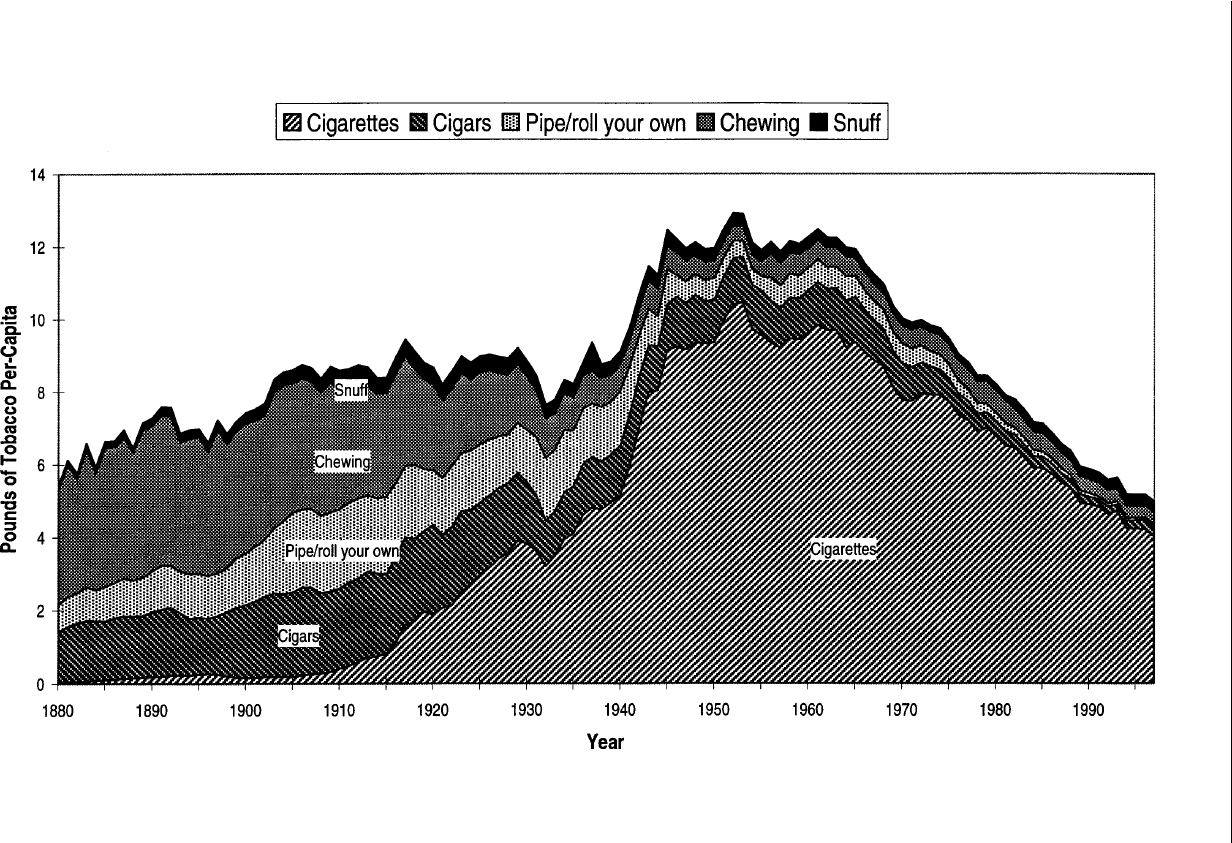
Chapter 2
22
Figure 1
Per-capita consumption of different forms of tobacco in the US 1880-1997

23
Trends in Cigar Consumption and Smoking Prevalence
Figure 2
U.S. estimated consumption of cigars 1950 to 1997
Chapter 2
24
Cigarette Smoking Act of 1969) that prohibited cigarette advertising on radio and
television, but which did not prohibit the advertising of cigars (U.S. Department
of Health and Human Services, 1989). Television advertising by manufacturers of
small cigars increased dramatically in 1972 and 1973 filling the void left by
cigarette advertisers, and sales of small cigars soared. In September 1973, Congress
passed a law banning the broadcast advertising of small cigars (The Little Cigar
Act - PL93-109) (U.S. Department of Health and Human Services, 1989); and the
consumption of small cigars dropped steadily until the early 1990’s when it
rebounded slightly.
As seen in Figure 2, the consumption of large cigars and cigarillos enjoyed a
resurgence in 1964, possibly due to cigarette smokers switching from cigarettes to
cigars following the first report to the U.S. Surgeon General on smoking and
health (U.S. Public Health Service, 1964). After 1965, consumption of large cigars
and cigarillos steadily declined until 1992. Since 1993, consumption of cigars of
all types (i.e., small, large, and large premium cigars) has increased (Maxwell,
1997); but by far the largest percentage increase has been in the consumption of
premium cigars. Between 1993 and 1996, sales of premium cigars increased by
nearly 154 percent.
Recent Trends in The recent upward trend in cigar sales in the United States may
Self-reported Use signal an increase in the prevalence of cigar smoking, an increase
in the number of cigars smoked among current users, or some combination. This
chapter examines national and regional survey data on self-reported cigar use in
an attempt to evaluate trends in the patterns of cigar use among different age,
gender, and racial groups.
Table 1.
Cigar consumption in the United States, 1993-1997
Cigar type millions of cigars millions of cigars % change
consumed consumed (1993-1997)
(1993) (1997)
large 2,138 3,589 67.9
small 1,280 1,447 13.0
total 3,418 5,036 47.3
Source: U.S. Department of Agriculture
Tobacco Situation and Outlook Report,
December 1997, TSB-240.
Data Sources The principal sources of nationally representative survey data to estimate
trends in cigar use by adults are the 1970, 1987, 1991, and 1992 National Health
Interview Surveys (NHIS), the 1986 Adult Use of Tobacco Survey (AUTS), and the
1992/93 and 1995/96 Current Population Surveys (Table 2a). Additionally, some
non-national surveys have included questions that can be used to estimate recent
trends in cigar smoking prevalence among adults. These surveys include the

25
Trends in Cigar Consumption and Smoking Prevalence
Table 2a
Data sources for adult cigar smoking prevalence

Chapter 2
26
Table 2a (
Continued
)
Data sources for adult cigar smoking prevalence

27
Trends in Cigar Consumption and Smoking Prevalence
1990 and 1996 California Adult Tobacco Use survey, and the cross-sectional and
cohort surveys conducted in 22 North American communities in 1989 and 1993
as part of the National Cancer Institute’s Community Intervention Trial for
Smoking Cessation (COMMIT) project (U.S. Public Health Service, 1995; Hyland
et.al, 1997) (Table 2a). Surveys that examine cigar smoking among adolescents
are included in Table 2b. It is important to note that differences in survey
methodology and the measures used to define cigar use make it difficult to
reliably compare trends in cigar use behavior between surveys. For example,
some surveys have restricted their definition of current cigar use to individuals
who report having smoked at least 50 cigars in their lifetime. Other surveys have
asked about “regular” use of cigars without defining the frequency of cigar
smoking. Few surveys have questioned cigar smokers about the quantity and
type of cigars typically consumed.
Prevalence of Ever Smoking Prevalence of ever smoking cigars was assessed by each of
Cigars Among Adults the national adult surveys (Table 3). Cigar smoking is
predominantly a male behavior. The overall male ever cigar smoking prevalence
declined slightly from 1986 to 1991, and then increased slightly in 1992. This
change in prevalence may also have occurred among females, but the prevalence
among females is so low that it is difficult to define a change with confidence.
Table 2a (
Continued
)
Data sources for adult cigar smoking prevalence

Chapter 2
28
Table 2b
Data sources for adolescent cigar smoking prevalence
The prevalence estimates from the Current Population Surveys are
significantly lower than those from the other national surveys, and this may be
due to differences in wording of the questions on cigar smoking in these surveys.
Respondents to the Current Population Survey were asked whether they had
“ever regularly used” cigars, but respondents in the Adult Use of Tobacco Survey
(AUTS) and in the NHIS were asked whether they had “ever smoked” cigars. Use
of the words “regular use” on the Current Population Survey may have implied a
more frequent use of cigars, and, therefore, those respondents who had smoked
cigars infrequently may have been less likely to respond affirmatively to this
question.

29
Trends in Cigar Consumption and Smoking Prevalence
Table 3
Cigar ever smoking prevalence from national surveys
1986 AUTS 1987 NHIS 1991 NHIS 1992 NHIS 1992-93 CPS 1995-96 CPS
Total Male 43.0±1.5 38.0±1.0 35.5±1.0 40.2±1.8 7.9±0.2 7.3±0.2
Age
18–24 31.5±4.2 24.7±2.0 22.3±2.3 29.5±4.8 2.3±0.3 3.0±0.3
25–34 37.9±3.2 30.0±1.5 25.8±1.5 34.4±3.2 3.3±0.3 3.4±0.3
35–44 46.3±3.3 39.4±2.0 36.5±1.8 39.1±3.3 6.5±0.4 5.4±0.3
45–64 11.3±0.4 9.7±0.4
45-54 52.8±4.1 44.5±2.3 45.3±2.3 45.8±4.2
55–64 50.5±4.1 48.3±2.4 45.7±2.4 49.6±4.7
65+ 49.8±4.3 49.5±2.0 44.4±2.1 48.4±4.1 17.0±0.7 15.2±0.07
Hispanic Origin*
Hispanic 34.7±6.5 22.5±2.6 21.3±3.0 25.5±4.7 3.5±0.4 3.0±0.4
Non-Hispanic White 43.6±1.6 39.2±1.1 36.8±1.0 41.5±1.8 9.0±0.2 8.4±0.2
Race
White 45.3±1.6 39.9±2.4 37.5±1.1 42.2±1.9
Black 29.7±5.1 26.6±3.3 25.2±2.5 32.0±4.7 5.6±0.5 4.8±0.5
Asian or PI 21.4±9.3 15.5±3.7 17.0±4.7 15.2±6.5 2.4±0.6 1.9±0.5
Other** 40.5±12.0 41.4±7.2 25.4±6.2 32.4±12.8 7.8±2.2 8.8±2.3
Educational Level
<12 44.6±3.5 42.5±2.1 37.6±2.1 38.9±3.4 9.6±0.5 7.9±0.5
12 43.7±2.6 37.9±1.4 35.4±1.5 41.1±2.9 7.8±0.3 7.3±0.3
13–15 41.3±3.1 35.4±1.8 33.7±2.2 41.6±3.3 7.2±0.4 7.0±0.4
16+ 41.6±3.1 36.2±1.7 35.3±1.7 38.6±3.2 7.7±0.4 7.1±0.4
1986 AUTS 1987 NHIS 1991 NHIS 1992 NHIS 1992-93 CPS 1995-96 CPS
Total Female 3.5±0.6 3.8±0.3 3.1±0.2 3.7±0.5 0.29±0.04 0.28±0.04
Age
18–24 2.2±1.3 4.5±0.9 2.7±0.7 5.0±1.7 0.16±0.07 0.16±0.08
25–34 4.2±1.2 4.7±0.6 3.0±0.6 4.7±1.2 0.23±0.07 0.26±0.08
35–44 5.1±1.4 4.2±0.6 4.3±0.6 3.2±0.9 0.36±0.09 0.35±0.09
45–64 0.42±0.09 0.35±0.08
45–54 4.4±1.7 4.3±0.9 3.5±0.6 4.1±1.5
55–64 2.9±1.4 3.0±0.6 3.3±0.7 3.2±1.3
65+ 2.0±1.1 1.7±0.4 1.6±0.5 2.2±0.9 0.21±0.07 0.21±0.07
Hispanic Origin*
Hispanic 6.6±3.6 2.7±0.9 1.7±0.6 2.9±1.3 0.23±0.11 0.18±0.10
Non-Hispanic White 3.3±0.6 3.9±0.3 3.2±0.3 3.8±0.5 0.32±0.04 0.30±0.04
Race
White 3.7±0.6 3.9±0.4 3.3±0.3 4.1±3.5
Black 1.9±1.3 2.9±0.6 1.6±0.4 1.8±0.9 0.23±0.09 0.21±0.09
Asian or PI 7.2±7.3 2.0±1.8 1.6±1.4 1.1±1.6 0.05±0.09 0.19±0.16
Other** 6.5±6.3 5.5±4.3 7.3±5.8 7.1±6.2 0.78±0.67 1.40±0.85
Educational Level
<12 3.4±1.3 3.6±0.5 2.7±0.5 3.2±1.0 0.38±0.10 0.32±0.09
12 3.3±0.9 3.6±0.4 3.1±0.4 3.2±0.8 0.25±0.05 0.24±0.05
13–15 3.9±1.1 4.7±0.6 3.2±0.5 4.7±1.4 0.30±0.07 0.28±0.07
16+ 3.9±1.4 3.6±0.6 3.3±0.6 4.3±1.0 0.31±0.09 0.32±0.08
*The White and Black categories in NHIS included those of Hispanic origin whereas in the CPS, all Hispanics are included in the Hispanic
category.
**The 1995/96 CPS category “Other” contains only American Indians. All other respondents were assigned to existing categories.

Chapter 2
30
The prevalence of cigar smoking by age and gender shows that, in surveys
conducted between 1986-1992, older males were more likely than younger males
to have ever smoked cigars. Ever cigar smoking did not vary by age among
females. The prevalence of ever smoking was lower in every age group in the
Current Population Surveys, but the pattern of ever cigar smoking by age group
among males in the Current Population Surveys was similar to that seen with the
other national surveys. Older males showed a significant decline in ever smoking
prevalence between 1992/93 and 1995/96 in the Current Population Surveys.
However, this decline was not evident among younger males, and there was a
small but statistically significant increase among males 18-24 years of age.
Non-Hispanic males were more likely than Hispanic males to have ever
smoked cigars. This pattern was seen on all national surveys. There were no
differences between Hispanic and non-Hispanic females. White males were more
likely than black males to report ever having smoked cigars. Rates for white and
black males decreased slightly from 1986 to 1991, but then rose again in 1992.
White females were somewhat more likely than black females to have ever
smoked cigars, but the rates for females did not vary by race from 1986 to 1992.
In 1987, males with fewer than 12 years of education were more likely than
males with greater than 12 years of education to report ever smoking cigars. This
difference by education is the opposite of that seen in more recent surveys.
There were no differences in ever cigar smoking rates by education among
women.
Data for the state of California can also be used to compare cigar smoking in
1990 with that in 1996. Table 4 presents the ever cigar smoking prevalence for
the State of California in 1990 and 1996 and shows an overall decline in ever
smoking prevalence among males, with no change among females. The
prevalence of ever smoking among males in California increased substantially
with age in the 1990 survey; but, between 1990 and 1996, the prevalence of ever
smoking declined among older age groups and increased in the 18-24 year old
group, resulting in a flattening in the gradient of ever smoking with age. Ever
smoking prevalence among women showed little change with age in 1990; but in
1996, there was a decline in ever smoking prevalence among older age groups
and an increase in the 18-24 year old group sufficient to produce an inverse
gradient with age.
Prevalence of Current Figure 3 shows changes in the percentage of adult current
Cigar Smoking cigar users among males and females in the United States between
1970 and 1992 using data collected from the NHIS. These data reveal that cigar
use has always been predominantly a male behavior. Between 1970 and 1992,
the prevalence of cigar use among adult males declined by 80 percent. The
decline in cigar use by males was evident in all age and racial groups (data not
shown). The highest prevalence of cigar use was among males between the ages
of 35 and 64 years. Male and female prevalence of current cigar smoking among
adults nationally also declined between 1986-1992 for all races (Table 5). Except
for 1987, there were no significant differences among the races in current cigar
smoking prevalence. By 1992, cigar use was a behavior rarely seen among

31
Trends in Cigar Consumption and Smoking Prevalence
Table 4
Current and ever cigar smoking prevalence among California adults, 1990 and 1996

Chapter 2
32
Figure 3
Percentage of adults (18+ years of age) who currently use cigars* by sex,
National Health Interview Surveys, 1970, 1987, 1991, and 1992
females of any age or among men under the age of 25 years.Data from the 1992/
93 and 1995/96 Current Population Surveys confirm the overall low prevalence
of cigar use among both men and women. In 1992/93, only 1.7 percent of males
and 0.5 percent of females reported current regular use of cigars. However, the
reported regular use of cigars increased slightly among males (i.e., to 2 percent)
and females (i.e., to 0.6 percent) in 1995/96 suggesting a reversal in the 2-decade
long decline in cigar use among adults in the United States.
Data from the longitudinal tracking survey of adults conducted between
1989 and 1993 in 22 North American communities as part of the NCI’s COMMIT
project also point to an increase in cigar use (Hyland et.al, in press). The 1989
and 1993 surveys asked whether the respondent regularly smoked cigars or
cigarillos (regular was defined as 3-4 times/week). Averaged across the 22
communities, the prevalence rate of regular cigar use increased 133 percent from
0.9 percent in 1989 to 2.1 percent in 1993. The reported increase in regular cigar
use was observed in all 22 communities and seen in every gender, age, race,
income, and smoking status category. The 1993 data show that both regular and
occasional cigar use were more frequently reported by younger respondents and
current cigarette smokers. The higher prevalence of cigar use among younger
adults represents a dramatic change from earlier surveys of cigar users.
* Current use identified those persons who had smoked 50+ cigars in their lifetime who currently smoke cigars

33
Trends in Cigar Consumption and Smoking Prevalence
Table 5
Cigar current smoking prevalence from national surveys
*The White and Black categories in NHIS included those of Hispanic origin whereas in the CPS, all Hispanics are included in the Hispanic
category.
**The 1995/96 CPS category “Other” contains only American Indians. All other respondents were assigned to existing categories.

Chapter 2
34
The 1990 and 1996 California Adult Tobacco Use Surveys are perhaps the
best source of data available to estimate recent trends in cigar use behavior.
California adults were asked about their current cigar smoking habits in 1990 and
1996. Over this 6-year interval, cigar smoking increased among both males and
females (Table 4). The rates of cigar smoking increased among males of each
race, but the increase was greatest among white and black males. Current cigar
smoking prevalence remained unchanged among males with less than a high
school education. In contrast, males with higher educational attainment and
income, and younger males, had increases in cigar smoking prevalence. Figure 4
compares current cigar smoking prevalence in 1990 and 1996 for different age
groups of males and clearly demonstrates that the increase in current cigar
smoking prevalence is predominantly occurring among younger age males (18-
44). A similar shift in cigar smoking prevalence is also occurring among young
women, but the prevalence of current cigar smoking remains low among women.
The increase in current cigar smoking prevalence with increasing educational
attainment and income (Table 4) is in marked contrast to the pattern observed
among cigarette smokers. Prevalence of cigarette smoking decreases with
increasing educational attainment and income. Figure 5 contrasts the 1996 data
for current cigarette and cigar smoking among California males by education and
Figure 6 provides the same contrast for income level. Clearly the influence of
these socioeconomic factors on these two tobacco-use behaviors is quite different.
Recent changes in use of cigars may be confined to current cigarette smokers,
or it may also be occurring among those who are not current cigarette smokers.
Table 6 presents data from the 1990 and 1996 California tobacco use surveys that
classify cigar and cigarette smoking by whether only one tobacco product is
currently being used or whether both products are currently being used. In 1996,
60 percent of males who reported currently smoking cigars did not smoke
cigarettes at the time of the survey, and 40 percent had never smoked more than
100 cigarettes in their lifetime (the definition of a never smoker). There was an
increase in male current cigar smoking prevalence between 1990 and 1996 for
current and former cigarette smokers, as well as for never smokers, but the
proportionate increase (278 percent) is greatest among never smokers. The
increase in cigar only use between 1990 and 1996 is also greater for those groups
with higher educational attainment and income.
Prevalence of Former There is little information available on the frequency with which
Cigar Smoking cigar smokers quit smoking cigars. Data from the 1991 NHIS
show that, among those males who had smoked 50 or more lifetime cigars, a
larger percentage of older males were former cigar smokers as compared to
younger males (Table 7). Former cigarette smokers were also more likely than
current or never cigarette smokers to be a former cigar smoker.
The California survey has data on the frequency with which people who
reported ever using cigars responded “not at all” when asked whether they
smoked some days, every day, or not at all. This group can be considered former
cigar smokers and can be further divided by whether the respondent reported

35
Trends in Cigar Consumption and Smoking Prevalence
14.0
12.0
10.0
8.0
6.0
4.0
2.0
0.0
18-24
25-44 45-64
65+
Age Group
Percent
1990
1996
30.0
25.0
20.0
15.0
10.0
5.0
0.0
<12
12 13-15
16+
Level of Education
Percent
Cigarettes
Cigars
Figure 4
Prevalence of current cigar smoking among California males of different ages, 1990 and 1996
Figure 5
Prevalence of current cigarette and cigar smoking among California males of different levels of
education, 1996

Chapter 2
36
Figure 6
Prevalence of current cigarette and cigar smoking among California males of different incomes, 1996
30.0
25.0
20.0
15.0
10.0
5.0
0.0
<-10,000 10,000-
20,000
20,001-
30,000
30,001-
50,000
50,001-
75,000
75,000+
Income
Percent
Cigarettes
Cigars

37
Trends in Cigar Consumption and Smoking Prevalence
Table 6
Prevalence of cigar use in California, alone and in combination with cigarette use,
1990 and 1996
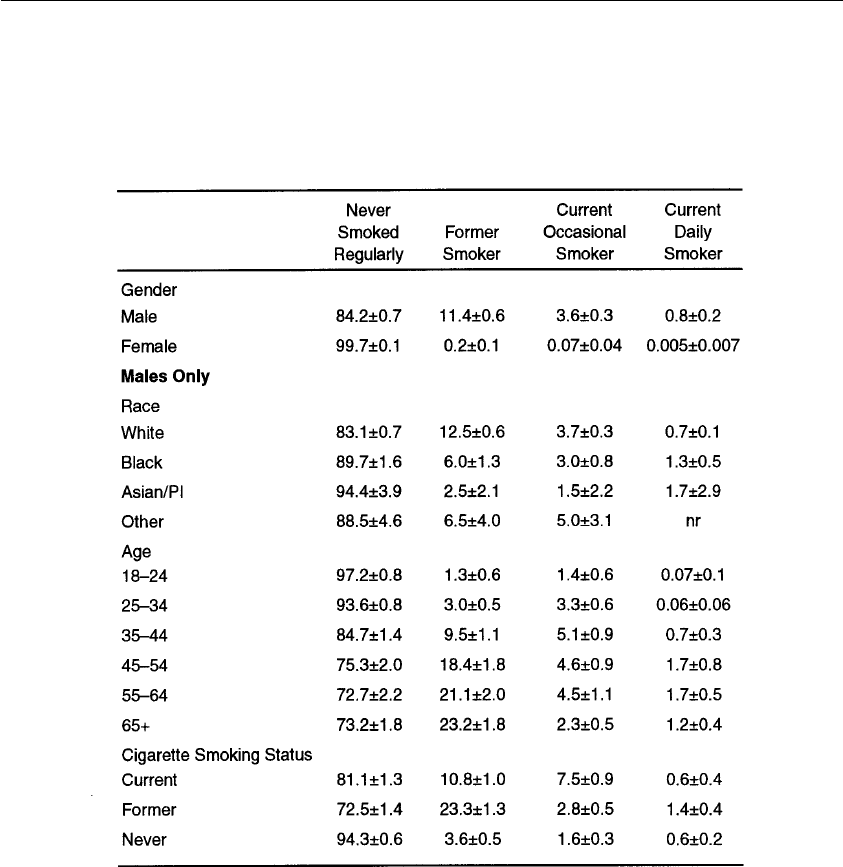
Chapter 2
38
Table 7
Current occasional, current daily and former cigar smoking rates, 1991 NHIS
smoking at least 50 lifetime cigars (Table 8). Among male Californians in 1996,
35.2 percent had ever smoked cigars, 8.8 percent currently smoked cigars and
26.4 percent were former cigar smokers. The prevalence of former cigar smoking
increases with increasing age and level of education. The majority of former
cigar smokers, using this definition of former smoker, had smoked fewer than 50
cigars in their lifetime.
Current daily cigar smoker = smoked
≥
50 cigars in life-time and smoking cigars daily at time of
interview.
Current occasional = smoked
≥
50 cigars in life-time but was not smoking cigars every day at
time of interview.
Former cigar smoker = smoked
≥
50 cigars in life-time but was not smoking at time of interview.
Never smoked regularly = never smoked
≥
50 cigars in life-time.

39
Trends in Cigar Consumption and Smoking Prevalence
Table 8
Detailed cigar smoking status among California adults, 1996

Chapter 2
40
Table 9
Frequency of cigar smoking among current cigar smokers, 1986 AUTS
Smoking Patterns— In 1986, more than half the current cigar smokers smoked less than
Frequency once per week, while 28.7 percent smoked at least once per day
(Table 9). The younger the smoker, the less likely he was to report smoking cigars
daily. Among those who reported that they currently smoke cigars, former and
never cigarette smokers were more likely than current cigarette smokers to smoke
cigars on a daily basis. The predominance of occasional use among cigar smokers
is not a recent phenomenon. Only one quarter of current cigar smokers reported
smoking daily in 1955 (Chaenszel, Shimkin and Miller, 1956).
In the 1991 NHIS, those respondents who had smoked 50 or more lifetime
cigars were asked whether they currently smoked cigars “some days,” “everyday,”
or “not at all.” Less than one percent of males were current daily cigar smokers;
females were even less likely than males to be smoking cigars daily (Table 7).
Black males were somewhat more likely than white males to be daily cigar
smokers. Males between the ages of 45-64 were more likely than younger males
to be smoking cigars daily. Some day smoking also varied with age, with males
aged 35-64 having the highest rates of some day cigar smoking.
Data from California (Table 10) show that between 1990 and 1996 there was
little change in male prevalence of daily cigar smoking, and the increase in cigar

41
Trends in Cigar Consumption and Smoking Prevalence
Table 10
Current cigar smoking prevalence among adult male Californians who have and have not smoked 50 or more cigars in their
lifetime, 1990 and 1996

Chapter 2
42
smoking prevalence was confined largely to the occasional cigar smoking group
(those who reported smoking cigars some days). The largest increase was in those
some day cigar smokers who had not yet smoked 50 cigars in their lifetime, and
the biggest increase among those who had not smoked 50 cigars in their lifetime
was in the youngest age group. These California data suggest that there has been
a dramatic increase in occasional cigar use recently, and that much of the change
that has occurred would have been missed if the evaluation were confined only
to those who had smoked more than 50 cigars in their lifetime.
Smoking Patterns— Among those cigar smokers who reported that they had smoked
Quantity cigars regularly in 1987, 56.4 percent (95 percent CI, 54.3-58.6
percent) reported smoking 1-2 cigars per day; 26.4 percent (95 percent CI, 24.5-
28.3 percent) reported smoking between 3 and 5 cigars per day, and 12.7 percent
(95 percent CI, 11.3-14.0 percent) reported smoking 6 or more cigars per day.
Unfortunately, most recent surveys have not collected information on quantity
of cigars smoked making it impossible to assess trends on this important
exposure variable.
Age of Initiation Among the national surveys, only the 1987 NHIS asked adults
of Cigar Smoking about the age at which they first smoked cigars, and this question
was only asked of those who had smoked more than 50 cigars in their lifetime.
The age of initiation of cigar smoking was older than that for cigarette smoking.
Among cigarette smokers, 60.2 percent had begun smoking regularly prior to age
18, whereas only 24.6 percent of those who had smoked more than 50 cigars in
their lifetime had started prior to age 18 (Table 11). Recent data on adolescent
use suggests that the age of initiation of cigar use currently may be much
younger than in the past.
Adolescent During 1996, four surveys asked teenagers about their cigar smoking.
Cigar Smoking Some surveys defined current smoking as having smoked cigars in the
past 30 days; other surveys used a measure of use in the past year.
A national survey conducted by the Robert Wood Johnson Foundation
(RWJF) found that 26.7 percent (95 percent CI, 25.0-28.4 percent) of 14-19 year
olds had smoked at least one cigar in the past year (Centers for Disease Control
and Prevention (CDC), 1997). Male adolescents (37 percent) were more than
twice as likely as female adolescents (16 percent) to have smoked a cigar in the
last year (Table 12). Those who smoked cigarettes or used smokeless tobacco in
the previous month were more likely to have smoked cigars than those who had
not used other tobacco products. There was a remarkably small difference in
cigar smoking by age, with 14-16-year-old adolescents reporting smoking at a
24.4 percent rate as compared to 27.5 percent of 19-year-old teens.
The adolescent respondents were asked how many cigars they had smoked in
the previous year. Nearly 3.0 percent had smoked more than 50 cigars in the
previous year. Cigarette smokers and smokeless tobacco users were more likely
than nonusers to have smoked 50 or more cigars in the previous year. The
percentage of these teenagers who had consumed 50 or more cigars in one year
was larger than the percentages of young adults who had smoked 50 or more
cigars in their lifetime measured by the earlier NHIS (Figure 7).

43
Trends in Cigar Consumption and Smoking Prevalence
Table 11
Age of initiation of cigarette and cigar smoking for white and black males, 1987 NHIS
Table 12
Cigar use in the past year among adolescents, 1996 RWJF National Survey

Chapter 2
44
Figure 7
Lifetime use of cigars by grade and gender
70
60
50
40
30
20
10
0
6
7 8 9 10 11 12
Percent
Females
Males
Total
Grade
Massachusetts Department of Public Health Survey, 1996

45
Trends in Cigar Consumption and Smoking Prevalence
The Massachusetts Department of Public Health assessed cigar use in grades 6
through 12 (CDC, 1997). The prevalence of ever having smoked a cigar increased
with increasing grade and leveled off at over 40 percent for students in grades 10
through 12 (Figure 7, Table 13). Males in all grades were more likely than
females to have ever smoked a cigar. Lifetime use of cigars by race (Figure 8) in
Massachusetts showed that whites were more likely than other racial groups to
have ever smoked a cigar.
The Massachusetts youth were also asked about past year and past month use
of cigars. Past year use of cigars increased with increasing grade, with the largest
increase between grades 7 and 8 (Table 13). The past year use for students in
grades 9-12 (comparable in age to the students from the RWJF survey) showed
that 28.1 percent had smoked a cigar in the past year, which was similar to the
RWJF estimate of 26.7 percent. Past 30 day cigar use was highest in grade 11 for
both male and female adolescents (Table 13). Cigar use was significantly higher
Table 13
Prevalence of cigar use in the last year, and all forms of tobacco use in the last 30 days, by
school grade, Massachusetts, 1996

Chapter 2
46
than smokeless tobacco use for males in grades 8 through 12 and for females in
grades 7 through 12. White students had the highest rate of past 30 day use,
followed by blacks and Hispanics (Figure 9).
California also surveyed adolescents to estimate their rates of cigar smoking
(Table 14). Males were more likely than females to have ever smoked a cigar.
Older students were more likely than younger students to have ever smoked a
cigar. White students were somewhat more likely than students of other races to
have ever smoked a cigar. The California Tobacco Survey also asked youths
between the ages of 12 and 17 about past 30-day cigar smoking. Males were
more likely than females to be currently smoking cigars. The rates of current
cigar smoking increased with age, and were somewhat higher among white and
Hispanic adolescents.
Rates for ever smoking cigars and past 30-day cigar smoking were lower
among the California teens than among the students in Massachusetts. This may
be due to the different methodologies used in these surveys. The Massachusetts
survey was anonymously conducted in schools; the California survey was a
household survey conducted via the telephone. School based surveys of teens
produce higher prevalence estimates for cigarette smoking than telephone
surveys in the home (U.S. Department of Health and Human Services, 1994). It is
possible that this is also true for cigar smoking behavior.
Figure 8
Ever cigar smoking by race among teenagers
35
30
25
20
15
10
5
0
White
Percent
Black Hispanic Asian Native
American
All Races
Massachusetts — 1996

47
Trends in Cigar Consumption and Smoking Prevalence
12
10
8
6
4
2
0
White
Percent
Black Hispanic
Race
Asian Native
American
Massachusetts, 1996
Figure 9
Past month use of cigars among teenagers by race
Table 14
Ever cigar smoking and current smoking in the last 30 days among California teenagers, 1996

Chapter 2
48
Another school based teen survey was conducted in 1996 among ninth grade
students in two New York counties (CDC, 1997). The median age of these
students was 14. Males were more likely than females to have smoked a cigar in
the previous 30 days (Table 15). As was seen on the RWJF national survey,
cigarette smokers and smokeless tobacco users were substantially more likely
than those who had not used other tobacco products to report having smoked a
cigar in the previous month. As was seen in Massachusetts, smokeless tobacco
use was lower than cigar use among these students (CDC, 1997).
DISCUSSION Data from the U.S. Department of Agriculture clearly demonstrate an
increase in the number of cigars consumed per year since 1993. State and
national surveys of smoking behavior suggest that competing trends in cigar
usage are occurring. Among older males, cigar usage continues to decline.
However, among young and middle-aged males, occasional use of cigars appears
to be increasing dramatically. Adolescents of both genders are also using cigars,
and some surveys show that their rates of use meet or exceed those of adults prior
to 1993.
The only national adult data on cigar smoking collected after 1992 is from
the Current Population Surveys, and these surveys show a low prevalence of cigar
smoking and very little change between 1992-3 and 1995-6. Part of the
explanation for the apparent difference between the consumption trends and the
prevalence trends may lie in the wording of the questions used in the Current
Population Surveys. The questions on this survey asked whether cigars were
currently, or had ever been, “regularly used.” This is in contrast to the NHIS
Table 15
Prevalence of adolescent cigar smoking in the past 30 days by various characteristics,
New York, 1996
Gender
Cigarette Smoking Status
Smokeless Tobacco Use Status

49
Trends in Cigar Consumption and Smoking Prevalence
which asked whether the respondent had ever smoked cigars or currently smoked
cigars. The difference in questions probably leads to a different subset of cigar
smokers who answer positively. Occasional cigar smokers and those who have
smoked fewer than 50 cigars in their lifetime may be more likely to answer no to
the Current Population Survey “use regularly” question, but respond yes to the
NHIS “smoke” question. Support for this explanation of the differences between
survey results is provided by survey data from California, where the prevalence of
male daily cigar smoking did not change between 1990 and 1996, and where
much of the change in cigar use was among those who have not yet smoked 50
cigars in their lifetime.
Changes in prevalence of occasional smoking in California between 1990 and
1996 are larger among well-educated and upper-income males and females. This
pattern is markedly different from that seen with cigarette smoking. Cigar
smoking increased among never smokers as well as among former cigarette
smokers. Initiation of tobacco use with cigars after becoming an adult is markedly
different from the predominantly adolescent initiation seen with cigarette
smoking.
Among California males who were never cigarette smokers 2 years prior to the
1996 survey, by 1996 4.16 percent (+/- 2.08 percent) of those who smoked cigars
were currently smoking cigarettes (new initiation) in contrast to 1.70 percent (+/-
0.45 percent) of those who did not smoke cigars. It is impossible to separate the
likelihood of cigar smoking leading to initiation of cigarette smoking from the
possibility that those who initiated cigarette smoking were also likely to smoke
cigars; but the commonality in both of these behaviors is nicotine ingestion, and it
would not be surprising if use of cigars predisposed an individual to the use of
cigarettes. It remains to be seen whether those who have never used tobacco
products prior to using cigars as adults will be able to remain occasional tobacco
users or will shift either to regular cigar use or begin smoking cigarettes.
Another concern is former cigarette smokers who are currently smoking cigars
occasionally. This group presumably includes a substantial number of individuals
who were nicotine-addicted while they were smoking cigarettes, and who may be
at increased risk of re-initiating their nicotine addiction due to their exposure to
the nicotine in cigars. Among California males who were former cigarette smokers
1 year ago, cigar smokers reported a current cigarette smoking (relapse) rate of
16.35 percent (+/- 6.50 percent) in contrast to the 7.06 percent (+/- 1.83 percent)
rate of current cigarette smoking among those who did not smoke cigars. This
observation does not separate the likelihood that cigar smoking leads to relapse of
cigarette smoking from the possibility that relapsing cigarette smokers take up
smoking cigars as well, but it raises a concern that cigar use may place former
cigarette smokers at increased risk of relapse.
Non daily smoking is also the predominant mode of cigar use among
adolescents, but this pattern of use is of much greater concern for this group
because the use of cigarettes and smokeless tobacco, two powerfully addictive
forms of tobacco, are also largely used occasionally during adolescence (U.S.
Department of Health and Human Services, 1994). Data from California
(Table␣ 16) show that a small number of male adolescents may have smoked cigars

Chapter 2
50
Table 16
Use of cigars by adolescents in California, 1996

51
Trends in Cigar Consumption and Smoking Prevalence
on 10 or more of the last 30 days. This frequency of use suggests that cigar
smoking among adolescent males is more than simple one-time experimentation.
The major concern is that this frequent use of a product that can provide
nicotine in substantial doses (Henningfield et. al, 1996) will lead to addiction
among those adolescents currently using cigars with some regularity (Chapter 6).
A second concern is the use of cigars by adolescents who have never used
other tobacco products. Table 17 shows an increased prevalence of cigar use
among male adolescents who use cigarettes or smokeless tobacco, a finding
present in most other recent surveys of adolescent use (CDC, 1997). Only 0.4
percent of those who have never used either cigarettes or smokeless tobacco are
currently smoking cigars, and only 3.6 percent have ever smoked cigars.
MONITORING If the emerging public health problem of cigar smoking is to be
RECOMMENDATIONS tracked successfully, tools for monitoring it must be designed to
measure the variable of interest in the most efficient manner possible. Questions
on cigar use should be included in surveys designed to measure tobacco use, and
the questions about cigar use should be standardized so that there is uniformity
of data collection. This will require researchers in the field of tobacco control to
establish standard definitions similar to those developed for cigarette smoking
(CDC, 1994).
It is recommended that (1) no threshold level of cigar smoking be required
before a respondent is asked about current cigar smoking status; (2) duration of
cigar smoking be asked of all respondents who ever smoked cigars whether or not
they are current cigar smokers; (3) age of initiation be asked of all respondents
who have ever smoked a cigar; and (4) some measure of frequency and type of
cigar smoked and of the quantity of cigars smoked be asked of all who have ever
smoked cigars.
Table 17
Prevalence of cigar smoking among adolescent males in California by the status of their use of
other tobacco products

Chapter 2
52
CONCLUSIONS
1. U.S. consumption of cigars has increased dramatically since 1993, reversing a
decline in cigar consumption that had persisted for most of this century.
2. In 1996, large inexpensive cigars (<$1 retail) and cigarillos accounted for the
greatest share of cigar sales (60.3 percent) followed by small cigars (33.2
percent), and large premium cigars (6.5 percent). In recent years, cigar sales
have increased in all three categories, but the fastest growing segment of the
cigar market has been the premium cigar category where sales have increased
by 154 percent since 1993.
3. Limited national data and data from California suggest that the prevalence of
cigar use among adults has increased since 1993. Much of that increase in
California has been in occasional cigar smoking. There has been little change
in the prevalence of daily cigar use among California adults between 1990
and 1996.
4. Among California adults in 1996, the prevalence of occasional cigar smoking
increased with level of education and income, a pattern opposite that seen
with cigarette smoking. This increase in prevalence with increasing level of
education and income is not seen for daily cigar smoking.
5. Males are more likely to smoke cigars than females.
6. The prevalence of current cigar smoking among adults has increased between
1990 and 1996 for both current and former cigarette smokers in California,
but the largest proportionate increase was among those who report never
having smoked cigarettes. This suggests that many adults who have never
smoked cigarettes are initiating tobacco use with cigars at ages when, prior to
1993, there had been little new initiation of tobacco use.
7. Multiple state and national surveys demonstrate a substantial rate of cigar
smoking, both use in the last 30 days and ever use, among adolescents of
both genders.

53
Trends in Cigar Consumption and Smoking Prevalence
Blackard, C.Z. Booming: In anti-tobacco America,
cigars’ sales growth is staggering. Tobacco Reporter
(May): 64, 1996.
Centers for Disease Control and Prevention. Cigarette
smoking among adults—United States, 1992, and
changes in the definition of current cigarette
smoking. MMWR. Morbidity and Mortality Weekly
Report 43: 342-346, 1994.
Centers for Disease Control and Prevention. Cigar
smoking among teenagers—United States,
Massachusetts and New York, 1996. MMWR.
Morbidity and Mortality Weekly Report 46: 433-440,
1997.
Giovino, G.A., Schooley, M.W., Zhu, B., Chrismon,
J.H., Tomar, S.L., Peddicord, J.P., Merritt, R.K.,
Husten, C.G., Eriksen, M.P. Surveillance for
selected tobacco-use behaviors—United States,
1900-1994. MMWR. Morbidity and Mortality Weekly
Report 43: 26, 1994.
Haenzel, W., Shimkin, M.B., Miller, H.P. Tobacco
Smoking Patterns in the United States. Public Health
Monograph No. 45, 1956.
Henningfield, J.E., Hariharan, X., Kozlowski, L.T.
Nicotine content and health risks of cigars. Journal
of the American Medical Association 276: 1857-1858,
1996.
Hyland, A., Cummings, K.M., Shopland, D.R., Lynn,
W.R. Prevalence of cigar use in 1989 and 1993 in
22 North American communities. Accepted for
Publication, American Journal of Public Health,
1998.
Maxwell, J.C., Jr. The Maxwell Consumer Report: The
Cigar Industry in 1996. Richmond, VA: Wheat
First Butcher Singer, March 21, 1997.
Milmore, B.K., Conover, A.G. Tobacco Consumption in
the United States, 1880-1955. In: Tobacco Smoking
Patterns in the United States. W. Haenszel, M.B.
Shimkin, H.P. Miller (Editors). Public Health
Monograph No. 45, pp. 107-111, 1956.
U.S. Code of Federal Regulations. Title 26 [Internal
Revenue Service] Part 270: Manufacture of cigars
and cigarettes. (As adopted at 26 F.R. 8173,
effective October 1, 1961). B (270) 3-B (270) 5,
October 31, 1970.
U.S. Department of Agriculture. Tobacco Situation and Outlook
Report. TBS-237. Washington, DC: U.S. Department of
Agriculture, Commodity Economics Division, Economic
Research Service, 1996.
U.S. Department of Agriculture. Tobacco Situation and
Outlook Report. TBS-239. Washington, DC: U.S.
Department of Agriculture, Commodity Economics
Division, Economic Research Service, 1997.
U.S. Department of Health, Education, and Welfare. The
Health Consequences of Smoking. DHEW Publication No.
73-8704. Rockville, MD: U.S. Department of Health,
Education and Welfare, Public Health Service, p. 175,
1973.
U.S. Department of Health and Human Services. Reducing the
Health Consequences of Smoking: 25 years of Progress: A
Report of the Surgeon General. DHHS Publication No.
(CDC) 89-8411. Atlanta, GA: U.S. Department of Health
and Human Services, Public Health Service, Centers for
Disease Control, Center for Chronic Disease Prevention
and Health Promotion, Office on Smoking and Health,
p. 511, 1989.
U.S. Department of Health and Human Services. Preventing
Tobacco Use Among Young People: A Report of the Surgeon
General. Atlanta, GA: U.S. Department of Health and
Human Services, Public Health Service, Centers for
Disease Control and Prevention, National Center for
Chronic Disease Prevention and Health Promotion,
Office on Smoking and Health, pp. 107-114, 1994.
U.S. Public Health Service. Smoking and Health: Report of the
Advisory Committee to the Surgeon General of the Public
Health Service. PHS Publication No. 1103. Rockville, MD:
US Department of Health Education and Welfare,
Public Health Service, Centers for Disease Control,
1964.
U.S. Public Health Service. Community-based Interventions for
Smokers: The COMMIT Field Experience. NIH Publication
No. 95-4028. Bethesda, MD: U.S. Department of Health
and Human Services, National Institutes of Health,
1995.
U.S. Department of the Treasury. Internal Revenue Cumulative
Bulletin. Revenue Ruling 69-198, p.359, 1969-1.
REFERENCES

55
Smoking and Tobacco Control Monograph No. 9
Chemistry and Toxicology
Dietrich Hoffmann and Ilse Hoffmann
HISTORICAL Early information on the smoking of cigars originates from artifacts of
NOTES the Mayas of the Yucatan region of Mexico. Smoking of tobacco was
part of the religious rituals and political gatherings of the natives of the
Yucatan peninsula as shown in the artwork on a pottery vessel from the 10th
century (Figure 1) where a Maya smokes a string-tied cigar (Kingsborough,
1825). Five hundred years later, in 1492, when Christopher Columbus
landed in America, he was presented with dried leaves of tobacco by
the House of Arawaks. Columbus and his crew were thus the first Europeans
who became acquainted with tobacco smoking. Early in the 16th century,
Cortez confirmed that tobacco smoking was practiced by the Aztecs in
Mexico. In addition, tobacco was grown in Cuba, Haiti, several of the West
Indian Islands, and on the East coast of North America from Florida to
Virginia (Tso, 1990).
The Mayan verb sikar, meaning to “smoke,” became the Spanish noun
cigarro. The form of cigar Columbus had first encountered was a long, thick
bundle of twisted tobacco leaves wrapped in dried leaves of palm or maize.
In 1541, the Cuban cigar appeared in Spain. The first person known to have
grown tobacco in Europe was Jean Nicot, the French ambassador to Portugal.
He introduced tobacco and tobacco smoke at the royal court of Paris, where
Catherine de Medici and her son, King Charles IX, used it to treat migraine
headaches (Jeffers and Gordon, 1996). In 1570, the botanist Jean Liebault
was the first to grow tobacco in France; he gave the plant the scientific name
Herba Nicotiana, in honor of Jean Nicot. However, the name tobacco, which
is derived from the American Indians’ word tobacco, remained in common
use.
In 1828, the chemists, Posselt and Reimann of the University of
Heidelberg, isolated nicotine as the major pharmacoactive ingredient in
tobacco. In 1895, Pinner established the chemical structure of nicotine as
that of 3-(1-methyl-2-pyrrolidinyl)pyridine.
THE CIGAR There are many types of cigars on the market. The U.S. Department of
the Treasury (1996) defines a cigar as “any roll of tobacco wrapped in leaf
Types and tobacco or in any substance containing tobacco,” while a cigarette is
Definitions defined as “any roll of tobacco wrapped in paper or in any substance
not containing tobacco.” In North America, and in many parts of Europe,
there are at least four types of cigars, namely, little cigars, small cigars (also
called cigarillos), regular cigars, and premium cigars (Figure 2). For taxation
purposes, the U.S. Department of the Treasury (1996) differentiates only
between small cigars, weighing not more than three pounds per thousand
(≤ 1.36 g/cigar), and large cigars, weighing more than three pounds per
thousand.

Chapter 3
56
Figure 1
A man smoking a Maya’s string-tied cigar depiected on a pottery vessel,
dated 10th century or earlier, found in Mexico.
Courtesy of the General Research Division, The New York Public Library, Astor, Lenox,
and Tilden Foundaitons.
In general, little cigars contain air-cured and fermented tobaccos. They are
wrapped either in reconstituted tobacco or in cigarette paper that contains
tobacco and/or tobacco extract. Some little cigars marketed in the U.S. have
cellulose acetate filter tips and are shaped like cigarettes (length 70 - 100
mm, weight 0.9 - 1.3 g each; Hoffmann and Wynder, 1972).
The small cigars on the U.S. market have straight bodies, weigh between
1.3 and 2.5 g each, are 70 - 120 mm long, and are open on both ends. To
some extent they are comparable to the stumpen, a form of cigar primarily
smoked in Switzerland and some parts of Germany. In the Far East, small
cigars, called cheroots, are made from heavy-bodied burley-type tobacco.
The Indian cheroots are produced from light, air-cured tobacco (Voges,
1984). In Denmark and some other parts of Scandinavia, similar types of
cigars are also called cheroots but like the small U.S. cigars, they are more
akin to the Swiss stumpen.
Regular cigars appear on the market in various sizes and shapes. In the
U.S., their dimensions are generally 110 - 150 mm in length, up to 17 mm in
diameter, and they weigh between 5 and 17 g. Regular cigars are rolled to a
tip, on at least one end. Some of them carry a ‘banderole,’ or decorative foil
or paper strip, to indicate the brand’s name (Wynder and Hoffmann, 1967;
Brunnemann and Hoffmann, 1974a; Schmeltz et al., 1976a and 1976b;
Voges, 1984). Many of the regular cigars on the U.S. market are machine-
made; others are hand-rolled.

57
Smoking and Tobacco Control Monograph No. 9
Figure 2
Types of cigars on the U.S. Market in 1996: (1) bidi (imported from India), (2)
little cigar with filter tip, (3) small cigar with plastic mouth piece, (4) regular cigar,
(5) and (6) premium cigar.
In recent years the popularity of premium cigars has increased in the
United States. With diameters ranging from 12 to 23 mm and lengths
between 12.7 and 21.4 cm, these cigars carry bands with an imprint of their
brand name and/or manufacturer’s name or logo. They are imported in large
numbers from the Dominican Republic, Honduras, Mexico, Jamaica, and
other countries (O’Hara, 1996). In 1996, the two most popular types of
premium cigars on the U.S. market were the “Coronas” and the “Lonsdales.”
The recorded 96 brands of Coronas were between 12.7 and 15.2 cm (5 - 6
inches) long and ranged in price between $1.10 and $8.60 apiece. The 111
recorded brands of Lonsdales were between 15.2 and 17.8 cm (6 - 7 inches)
long and sold for $1.50 to $11.00 per cigar (Cigar Aficionado, 1996).
Cigar Tobacco Tobacco belongs to the Solanaceae family. Primarily two species,
Nicotiana tabacum and Nicotiana rustica, are used for the manufacture of
chewing tobacco, oral and nasal snuff, cigarettes, cigars, and pipe tobacco.

Chapter 3
58
Most of the tobacco products manufactured in North America, Western
Europe, and Africa are made of N. tabacum. N. rustica is predominately used
in South America, Russia, the former republics of the U.S.S.R., and Poland;
and, to some extent, also in India and Turkey. Within the N. tabacum
species, four types are commonly used: bright (Virginia), burley (Kentucky),
Maryland, and Turkish (oriental) tobaccos. Bright tobaccos are flue-cured by
drying with artificial heat; burley and Maryland tobaccos are air-cured; and
Turkish tobaccos are sun-cured.
Cigars consist of a filler (the inner part of the cigar), a binder, and a
wrapper. The filler, binder, and wrapper of small cigars, regular cigars, and
premium cigars are all made with air-cured and fermented tobaccos (Cornell
et al., 1979). Since the mid-fifties, the binders and/or wrappers of many of
the regular brands (but not of premium brands) are made from reconstituted
cigar tobacco (Moshy, 1967). In general, about 85 percent of the weight of a
cigar is contributed by the filler, 10 percent by the binder, and 5 percent by
the wrapper (Frankenburg and Gottscho, 1952).
The air-curing process of burley and Maryland tobaccos is characterized
by slow, gradual drying of the leaf. Usually, the whole tobacco plant is cut
off at ground level and hung in sheds or barns. However, in the case of
tobaccos used for many regular cigars and premium cigars, the leaves are
primed and hung individually on strings in sheds or barns for air-curing.
It is important to ensure ample air flow through the barns during this
process. Sometimes it is necessary to raise the temperature in the barns using
charcoal fires, thereby creating a relative humidity of 65 - 75 percent. During
air-curing, tobacco leaves normally reach the yellow stage 10 - 12 days after
harvesting, and the brown stage after another 6 or 7 days. To complete the
air-curing process requires 30 - 40 days. During this time, 80 - 85 percent of
the water content of the leaves is lost. The total nitrogen content is reduced
by about 30 percent and the protein-nitrogen content by about 50 percent;
however, the percentage of nitrate nitrogen doubles, and the nicotine
content remains practically unchanged. Following air-curing, the leaves are
aged for up to two years, or even longer. During this time, the nicotine
content is reduced by 30 - 50 percent, whereas protein, ammonia, and nitrate
nitrogen contents generally remain unchanged (Wolf, 1967).
To become cigar tobacco, the leaves need to be fermented. After about 1
year of storage and aging, the leaves are placed in special rooms for
fermentation at about 45°C and a relative humidity of 60 percent. After 3 - 5
weeks, the leaves are removed from the rooms, repacked, and returned. The
repacking process is repeated several times to induce “sweating.” The baled
leaves are occasionally slightly moistened. The temperature in the center of
the bales may reach up to 58°C. During the fermentation, chemical and
bacterial reactions lead to the formation of carbon dioxide, ammonia, water,
and various volatile compounds. Carbohydrates in the leaves are reduced by
50 - 70 percent, organic acids by up to 30 percent, and a major portion of the
polyphenols is degraded. The degradation of polyphenols during curing
causes the browning of the leaves; whereas during fermentation, their

59
Smoking and Tobacco Control Monograph No. 9
degradation ensures the oxygenation of several leaf components. The pH of
the fermented tobacco is slightly alkaline (Wolf, 1967; Wiernik et al., 1995).
During curing and fermentation of air-cured tobacco, nitrate is partially
reduced to nitrite, primarily by microbal action. This contributes to the
N-nitrosation of nicotine, converting it into the highly carcinogenic,
tobacco-specific N-nitrosamines (TSNA), N
’
-nitrosonornicotine (NNN), and
4-(methylnitrosamino)-1-(3-pyridyl)-1-butanone (NNK) (Burton et al., 1992;
Hoffmann et al., 1994; Wiernik et al., 1995).
Manufacture Cigars consist of filler, binder, and wrapper; all of which are air-cured
of Cigars and fermented. In recent decades, some brands of regular cigars
(though not premium cigars) have used reconstituted cigar tobacco as binder,
wrapper, or both (Moshy, 1967; Halter and Ito, 1980). Cigars are either hand-
rolled (Jeffers and Gordon, 1996) or machine-made (Van der Boor, 1996).
The flavor and aroma of cigars and their smoke are, in large measure, the
results of precisely controlled fermentation of the tobacco. Most little cigars
are machine-made, much like cigarettes, except that fermented cigar tobacco,
not blends of cured tobaccos are used (20, 30, or 50 cuts per inch); the little
cigars have wrappers which contain tobacco.
CHEMISTRY OF Processed tobacco contains at least 3,050 different compounds.
CIGAR TOBACCO Table 1 lists the major groups of compounds that have been
identified in tobacco (Roberts, 1988). Most of these are already present in the
green tobacco leaf, others are formed during curing, aging, and fermentation.
Although only a portion of the 3,050 compounds has been identified
specifically in cigar tobacco, one may assume that the full spectrum of
compounds is present in cigar tobacco, albeit in many cases, at different
levels of concentration than are present in cigarette tobaccos. Exceptions to
the qualitatively comparable constituents of cigar and cigarette tobaccos are
agents such as pesticides, that are applied to tobacco during cultivation of the
plant, and agents that are added during the processing of the tobaccos.
In the case of the insect control agents, the last reports on organic
chlorinated hydrocarbons were published in the 1960s. DDT concentration
was significantly higher in cigar tobacco (10.0 - 53.0 µg/g) than in cigarette
tobacco (2.0 - 6.0 µg/g), whereas DDD and endrin concentrations in cigar
tobaccos (10 - 15 µg/g and 0.0 - 0.5 ppm) and cigarette tobaccos (12 - 23 µg/g
and < 0.5 - 2 ppm) were comparable (Lawson et al., 1964). However, in the
seventies, chlorinated pesticides were banned for use on tobacco; thus, their
concentrations in U.S. tobacco declined by > 98 percent by 1994 (Djordjevic
et al., 1995b). An overview of the pesticides currently applied to U.S. tobacco
plants and a discussion of their residues on tobacco was presented by Sheets
(1991).
In general, flavor additives are not applied to cigar tobacco which is quite
different from the treatment of tobacco formulated for cigarettes, especially
in the case of filter cigarettes designed to yield low nicotine emission (Doull
et al., 1994; Hoffmann and Hoffmann, 1997). It is also different from pipe
tobacco formulation (LaVoie et al., 1985) and possibly from the formulation
of tobacco for small cigars. Furthermore, it is unlikely that plasticizers are

Chapter 3
60
Table 1
Compounds identified in tobacco and smoke
No. in No. in No. in
Functional Groups Tobacco Smoke Tobacco and Smoke
Caboxylic Acids 450 69 140
Amino Acids 95 18 16
Lactones 129 135 39
Esters 529 456 314
Amines & Imines 205 227 32
Anhydrides 10 10 4
Aldehydes 111 106 48
Carbohydrates 138 30 12
Nitriles 4 101 4
Ketones 348 461 122
Alcohols 334 157 69
Phenols 58 188 40
Amines 65 150 37
Sulfur Compounds 3 37 2
N-Heterocycles:
Pyridines 63 324 46
Pyrroles & Indoles 9 88 3
Pyrazines 21 55 18
Non-aromatics 13 43 7
Polycyclic Aromatics 1 36 0
Others 4 50 2
Ethers 53 88 15
Hydrocarbons:
Saturated Aliphatics 58 113 44
Unsaturated Aliphatics 338 178 10
Monocyclic Aliphatics 33 138 25
Polycyclic Aliphatics 55 317 35
Miscellaneous 112 110 19
Inorganics & Metals 105 111 69
Source: D.L. Roberts, 1988
used for manufacturing small, regular and premium cigars which do not
contain reconstituted tobacco, whereas plasticizers (e.g., glyceryl triacetate,
triethylene glycol diacetate) are applied to filter tips in the production of little
cigars. When reconstituted tobacco is chosen as a binder and/or wrapper for
regular cigars, such cigars will contain plasticizers and other tobacco
treatment products in addition to humectants, adhesives, and/or inorganic
additives (Moshy, 1967).
Distinct quantitative differences between cigar and cigarette tobaccos
are primarily related to the long aging and fermentation process of cigar
tobacco. Table 2 shows some of the distinct differences for a select number
of compounds as they occur in cigar tobacco and in the four major types
of cigarette tobaccos. Cigar tobacco contains only traces of polyphenols

61
Smoking and Tobacco Control Monograph No. 9
Table 2
Comparison of some selected components in the tobacco of cigars and of four cigarette
Tobacco Types (% of dry weight of tobacco)
Type of Tobacco
Component Cigar Burley Maryland Bright Oriental
Nitrate 1.4 - 2.1 1.4 - 1.7 0.9 < 0.15 < 0.1
pH 6.9 - 7.8 5.2 - 7.5 5.3 - 7.0 4.4 - 5.7 4.9 - 5.3
Reducing Sugars 0.9 - 2.7 1.5 - 3.0 1.2 7.0 - 25.0 5.5
Total Polyphenols < 0.1 2.0 1.6 5.1 4.5
Nicotine 0.6 - 1.7 2.0 - 2.9 1.1 - 1.4 1.2 - 1.9 1.1
Paraffins 0.3 - 0.32 0.34 - 0.39 0.34 - 0.41 0.24 - 0.28 0.37
Neophytadiene 0.4 - 0.8 0.4 0.40 0.3 0.2
Phytosterols 0.14 - 0.16 0.3 - 0.39 0.38 0.3 - 0.45 0.26
Citric Acid 5.5 - 6.0 8.22 2.98 0.78 1.03
Oxalic Acid 3.3 - 3.6 3.04 2.79 0.81 3.16
Maleic Acid 1.5 - 1.8 6.75 2.43 2.83 3.87
References: Wolf, 1967; Hoffmann and Wynder, 1972; Schmeltz et al., 1976a and 1976b; Tso, 1990.
(< 0.1 percent; Table 2) compared to cigarette tobaccos (1.6 - 5.1 percent).
The nitrate content of cigar tobacco is relatively high (1.4 - 2.1 percent
versus. < 0.1 - 1.7 percent in U.S. cigarette tobacco blends) and the amounts
of phytosterols are lower in cigar tobacco (0.14 - 0.16 percent versus. 0.26 -
0.45 percent). In respect to the nitrate content,
the pH of a suspension of tobacco in water, and the percentage of reducing
sugars, cigar tobacco is comparable to the two types of air-cured cigarette
tobaccos, namely, burley and Maryland (Wolf, 1967; Hoffmann and Wynder,
1972; Tso, 1990; Schmeltz et al., 1976a and 1976b).
During the processing of tobacco, especially during air-curing and
aging, nitrate is partially reduced to nitrite (Burton et al., 1992; Hoffmann
et al., 1994; Wiernik et al., 1995). Nitrite is a strong N-nitrosating agent of
secondary and tertiary amines. Consequently, during these stages of tobacco
processing, N-nitrosamines are formed (Hoffmann et al., 1994). In tobacco,
we distinguish between volatile nitrosamines (VA), nonvolatile nitrosamines
(NVA), nitrosamino acids (NA), and tobacco-specific N-nitrosamines
(TSNA). The latter group is of significance for several reasons. TSNA are
formed by N-nitrosation of nicotine and of the minor Nicotiana alkaloids,
nornicotine, anatabine, and anabasine (Figure 3). Among the seven TSNA, 4-
(methylnitrosamino)-1-(3-pyridyl)-1-butanone (NNK), N
’
-nitrosonornicotine
(NNN), and 4-(methylnitrosamino)-1-(3-pyridyl)-1-butanol (NNAL) are
strong carcinogens in mice, rats, hamsters, and mink. N
’
-Nitrosoanabasine
(NAB) is weakly carcinogenic, while N
’
-nitrosoanatabine (NAT),
4-(methylnitrosamino)-4-(3-pyridyl)-1-butanol (iso-NNAL), and
4-(methylnitrosamino)-4-(3-pyridyl)butyric acid (iso-NNAC) are inactive
in carcinogenesis assays (Hoffmann et al., 1994). Furthermore, in the

Chapter 3
62
Figure 3
Formation of tobacco-specific N-nitrosamines. Iso-NNAC, 4-(methylnitrosamino)-4-(3-pyridyl)-
butyric acid; NNA, 4-(methylnitrosamino)-4-(3-pyridyl) butyric aldehyde; NNK, 4-
(methylnitrosamino)-1-(3-pyridyl)-1-butanone; NNN, N’-nitrosonornicotine; NAT, N’-
nitrosoamatabine; NAB, N’-nitrosoanabasine; iso-NNAL, 4-(methylnitrosamino)-4-(3-pyridyl)-
1-butanol; NNA, 4-(methylnitrosamino)-4-(3-pyridyl)-1-(3-pyridyl)-1-(3-pyridyl)-1-butanol
N
Nornicotine
N
H
Demethylation
N
Nicotine
N
CH
3
Enzymatic
Oxidation
N
NNN
N
NO
N
NNK
Reduction
Nitrosation
N
O
NO
N
Anabasine
N
H
N
NAT
N
NO
N
Anatabine
N
H
N
NAB
N
NO
CH
3
N
NNAL
N
H
HO
NO
CH
3
N
NNA
N
CHO
NO
CH
3
N
Iso-NNAL
N
NO
CH
3
CH
2
OH
N
Iso-NNAC
N
COOH
NO
CH
3
N
Cotinine Acid
N
COOH
H
CH
3
Source: Hoffmann et al., 1994.
smoke of a nonfilter cigarette, about 45 percent of NNN originates by transfer
from the tobacco, whereas the remainder is pyrosynthesized during smoking
(Hoffmann et al., 1977). Between 23 percent and 35 percent of the NNK in
smoke originates from the tobacco by transfer (Adams et al., 1983). NNN in
cigar tobacco is present at levels of 3.0 - 10.7 µg/g, in the tobacco of little cigars
at 11.1 - 13.0 µg/g, in tobacco of nonfilter cigarettes at 1.5 - 2.2 µg/g, and in
tobacco of filter cigarettes at 5.0 - 6.6 µg/g. NNK levels in the four tobacco
types are 1.2 - 1.3 µg/g, 3.5 - 4.5 µg/g, 0.5 - 0.8 µg/g, and 0.4 - 1.0 µg/g,
respectively (Brunnemann et al., 1983). During fermentation of cigar tobacco,
a small portion of nicotine is converted into 2,3-dihydronicotine, which easily
forms 4-methylamino-1-(3-pyridyl)-1-butanone (Frankenburg et al., 1958).
The latter, a secondary amine, is rapidly N-nitrosated to NNK. This compound
and the higher nitrate levels in cigars may explain why more NNK is formed in
little and regular cigars than during the processing of cigarette tobacco.
Table 3 presents data obtained in a comparative study of the
concentrations of nicotine, nitrate, volatile nitrosamines (VNA), nonvolatile
nitrosamines (NVNA), and TSNA in cigar and cigarette tobacco (Brunnemann
et al., 1983). All seven of the VNA identified are carcinogenic in mice, rats,
and/or hamsters. The nonvolatile nitrosoproline is neither carcinogenic in rats
nor in hamsters, while N-nitrosodiethanolamine (NDELA) does cause cancer in

63
Smoking and Tobacco Control Monograph No. 9
Table 3
Nicotine nitrate and N-nitrosamines in the tobacco of U.S. cigars little cigars, and nonfilter
and filter cigarettes (ng/g)
Little Nonfilter Filter
Compound Cigars Cigars Cigarettes Cigarettes
Nicotine, % 1.10 1.66 - 1.72 1.81 - 2.05 1.45 - 2.04
Nitrate, % 1.98 0.74 - 0.89 0.7 - 1.08 0.81 - 1.23
Volatile Nitrosamines
Nitrosodimethylamine n.dt. 43 250 - 280 n. dt. - 6.7
Nitrosodiethylamine 3.2 11 n. dt. - 47 n. dt. - 2.0
Nitrosodi-n-propylamine 11.8 nd n. dt. n. dt. - 2.3
Nitrosodi-n-butylamine 0.9 nd n. dt. - 65 n. dt.
Nitrosopiperidine 22 nd 5.5 - 13.3 n. dt. - 7.0
Nitrosopyrrolidine 20 19 n. dt. - 4.9 n. dt. - 9.9
Nitrosomorpholine 44 nd 3.7 - 4.1 n. dt. - 10.0
Non-Volatile Nitrosamines
Nitrosodiethanolamine 108 420 115 194
Nitrosoproline 1130 nd 880 - 1200 1450 - 2300
Tobacco-Specific Nitrosamines
N
1
-Nitrosonornicotine 2940 4500 1830 - 1960 1940 - 3200
Total TSNA 4780 9300 3610 - 4090 3730 - 8900
Abbreviations: nd, not determined; n. dt., not detected.
Source: Brunnemann and Hoffmann, 1981; Brunnemann et al., 1983.
mice, rats, and hamsters. The concentrations of the VNA and TSNA are
somewhat higher in cigar tobaccos than in cigarette tobaccos. Since the
nitrate content of the tobaccos of the little cigars tested was not exceptionally
high (0.74 - 0.89 percent), other factors must be correlated with these high
NDELA and TSNA values.
As already mentioned, tobacco also contains nitrosamino acids. The
noncarcinogenic N-nitrosoproline and N-nitrosopipecolic acid belong to this
group. In addition, cigarette tobaccos were found to contain the carcinogenic
N-nitrososarcosine, 3-(methylnitrosamino)propionic acid, and 4-(methylni-
trosamino)butyric acid (Djordjevic et al., 1989). Cigar tobacco has not yet
been analyzed for these nitrosamino acids.
Cigar tobaccos, like other types of processed tobaccos, contain at least
28 metals and more than ten metalloids (Wynder and Hoffmann, 1967;
Iskander et al., 1986). Their concentrations range from 5,300 to 97,000 µg
calcium/g tobacco to trace amounts, as in the case of mercury (0.05 µg/g
tobacco) (Wynder and Hoffmann, 1967; Andren and Harriss, 1971). Most
of the metals and metalloids are essential elements for the tobacco plant.
Others, such as lead, arsenic, and mercury, are trace contaminants. Small

Chapter 3
64
portions, at most a few percent of the metals and metalloids, transfer from
the tobacco into the smoke. Among those that transfer into the smoke and
are thus inhaled, the International Agency for Research on Cancer (1987)
considers arsenic, beryllium, chromium, nickel, and cadmium as human
carcinogens (IARC, 1993a, 1993b).
Like all types of tobacco, cigar tobacco contains, or may contain,
radioactive elements such as radium-226 and polonium-210 at
concentrations ranging from 0.1 - 0.47 and 0.18 - 0.46 pCi/g cigar tobacco
respectively) (Tso et al., 1966a). Phosphate fertilizers are the major source
of these radioelements (Tso et al., 1966b); minor contributions come from
airborne particles carrying lead-210 and polonium-210. These particles are
trapped by the trichomes on the undersides of the tobacco leaves (Martell,
1974). A minor amount of polonium-210 transfers into the mainstream
smoke and is thus inhaled by the smokers. The U.S. National Council on
Radiation Protection and Measurement (1987) ascribes about 1 percent of the
risk for lung cancer after 50 years of cigarette smoking to the role of
polonium-210 inhaled as a tobacco smoke constituent.
CHEMISTRY AND It is one of the objectives of tobacco-related research to design
ANALYSIS OF smoking devices that can simulate human smoking patterns
MAINSTREAM under reproducible conditions. Smoking instruments that are
CIGAR SMOKE widely accepted today are piston-type machines which generate
puff profiles that simulate the puff profiles of smokers (Wynder
Smoking Conditions and Hoffmann, 1967). For the smoking of cigarettes by
machines, the U.S. Federal Trade Commission (FTC) (Pillsbury et al., 1969)
adopted and modified a method that was initially devised by Bradford et al.
in 1936. This method employs, as standard smoking conditions, one puff per
minute, of two-seconds duration with a volume of 35 ml; the butt length is
23 mm for nonfilter cigarettes and filter length plus overwrap, plus 3 mm,
for filter cigarettes (Table 4). The U.K., Germany, and the Cooperative Center
for Scientific Research Relative to Tobacco (Centre De Cooperation Pour Les
Recherches Scientifiques Relatives Au Tabac, CORESTA) in Paris, France,
developed similar standard smoking parameters (Brunnemann et al., 1976a).
The FTC smoking schedule has also been employed for the determination of
“tar,” nicotine, carbon monoxide, and other smoke constituents in the
mainstream smoke of little cigars (Hoffmann and Wynder, 1972; Schmeltz et
al., 1976a).
In the course of smoke-uptake analyses, it soon became clear that the
employed machine-smoking conditions do not simulate the smoking habits
of consumers of filter cigarettes; most certainly they are not even close
to the average smoking parameters observed for smokers of filter cigarettes
delivering low levels ≤( 1.2 mg/cigarette, according to the FTC method) of
nicotine (Russell, 1980a; Herning et al., 1981; Fagerström, 1982; Haley et al.,
1985). With a recently developed “tobacco smoke inhalation testing
system,” it has been shown that smokers of cigarettes with low nicotine
yields ≤( 1.2 mg/cigarette according to FTC method) titrate nicotine uptake
by taking, on average, 12 ± 2.7 puffs per cigarette (FTC 10) with average puff
1
The scientific definition of "tar" is the total particulate matter collected by a Cambridge filter after subtacting
moisture and nicotine. (SG Report 1972, Chapter 9)

65
Smoking and Tobacco Control Monograph No. 9
Table 4
Standard conditions for machine smoking of cigars, cigarettes, and pipe
Parameters Cigars (CORESTA)
2
Cigarettes (FTC)
1,4
Pipes (CORESTA)
3
Weight 2.5 - 8.0 g 0.9 - 1.1 g 1.2 g (filling)
Puff:
Frequency 1/40 seconds 1/60 seconds 1/20 seconds
Duration (sec.) 1.5 2 2
Volume (ml) 40 35 50
Butt length (mm) 33 23 nonfilter 1.0 g burned
1
Pillsbury et al., 1969;
2
International Committee for Cigar Smoking, 1974;
3
Miller, 1963;
4
Little cigars are smoked as
cigarettes.
volumes of 52 ± 5.7 ml (FTC 35 ml), puff durations of 1.7 ± 0.24 seconds (FTC
2.0 seconds), every 28.5 ± 10.3 seconds (FTC 58 seconds). When operated
with the same parameters that were determined for individual smokers, a
smoking machine produced smoke yields per cigarette of 28 - 40 mg “tar”
(FTC 11 - 14 mg) and 2.1 - 2.5 mg nicotine (FTC 0.9 - 1.0 mg). Smoke
emissions of the carcinogenic BaP were 23.2 - 25.5 ng (FTC 11.9 - 21.9 ng)
and those of NNK were 30.1 - 33.9 ng (FTC 14.4 - 14.9 ng) per cigarette
(Djordjevic et al., 1995a).
Today, more than 97 percent of all cigarettes in the U.S. have filter tips
(Creek et al., 1994) and about 75 percent of these give FTC-measured nicotine
yields of ≤ 1.2 mg/cigarette. The FTC data for “tar,” nicotine, and carbon
monoxide are, therefore, of limited usefulness and can, at most, compare
relative smoke yields of commercial cigarettes generated under the FTC
standardized smoking conditions.
Rickert et al. (1985) examined the delivery of “tar,” nicotine and CO per
liter of smoke for different tobacco products. They found that the mean
yields per liter of smoke were highest for small cigars followed by hand-rolled
and manufactured cigarettes and were lowest for large cigars. Total delivery
was greatest for large cigars because of their larger amount of tobacco.
So far, only a study by Miller (1963) has been concerned with a
standardized method for pipe smoking. The pipe is filled with 1.2 g tobacco
and is smoked by taking five puffs per minute, of two-seconds duration and a
50-ml volume per puff. Miller also determined nicotine in the tobacco and
the smoke yields of the tobaccos from a filter cigarette (1.58 percent nicotine)
and two pipe tobaccos (1.52 percent and 1.30 percent nicotine), all smoked in
a pipe bowl. Then, smoking 1.0 g of the tobacco from a filter cigarette under
the pipe smoking conditions, he found 59.5 mg “tar,” 7.15 mg nicotine, and
1.36 vol. % CO, whereas the pipe tobaccos gave 53.3 and 56.4 mg “tar”, 5.18
and 6.12 mg nicotine, and 1.04 and 1.10 vol% CO. When the filter cigarette
tobacco was smoked in a cigarette with such standard cigarette-smoking
conditions, the yields for the 1 g of tobacco smoked were: 24.1 mg “tar,”
*
Mainstream smoke (MS) is the smoke a smoker draws into his mouth from the butt end or mouth piece of a
cigar, cigarette, or pipe. Sidestream smoke (SS) is the smoke emitted form the burning cone of a cigar or
cigarette, or pipe during the interval between puffs. (SG Report 1979 Chapter 14)

Chapter 3
66
1.63 mg nicotine, and 4.89 vol% CO. Clearly, pipe smoking produces
much higher yields of “tar” and nicotine per gram of tobacco than cigarette
smoking.
It has been reported that with increasing number of puffs per given cigar,
and also with increasing puff volume per given unit of time (puff velocity),
the amount of tobacco burned rises linearly (Rice and Scherbak, 1976).
CORESTA developed a standard smoking method for cigars with the following
parameters: one puff of 20 ml volume is taken during 1.5 seconds every
40 seconds. The cigars are smoked to a butt length of 33 mm. In 1974, the
International Committee for Cigar Smoke Study of CORESTA chose these
smoking parameters as an average of the observations made on cigar smokers
in France, Germany, the U.S., and the U.K. The smoke yields for cigars
reported in the literature since 1974 are based on the CORESTA method
(Table 4). However, for smoke analyses of little cigars, the cigarette-smoking
parameters of the FTC are applied. To date, the testing of the actual smoking
parameters of cigar smokers by a computer-assisted instrument has not
been reported. Table 4a presents the dimensions and yield characteristics
of cigarettes, little cigars, large cigars, and premium cigars smoked under
these standardized machine smoking conditions.
Physicochemical Tobacco smoking, like the burning of all organic matter, is a
Nature of Cigar process of incomplete combustion governed by several in air factors
Smoke relating to the combustibility of certain leaf components (such
as laminae, ribs, and stems), insufficient supply of oxygen, and the existence
of a temperature gradient in the burning cone.
At least three types of reactions occur simultaneously during smoking:
pyrolysis, pyrosynthesis, and distillation. The process of tobacco burning leads
to thermal degradation, in which organic matter is broken down into smaller
molecules (pyrolysis). The newly formed fragments, or radicals, are often
unstable and may recombine with identical and/or other radicals to form
components that were not originally present in tobacco. This process is called
pyrosynthesis. Distillation of certain compounds from the tobacco into the
smoke is the third process occurring during smoking. Compounds such as
nicotine and some low-molecular-weight terpenes participate in this third
process. They decompose only partially (Osdene, 1976). Some of the metals
transfer into the smoke stream while entrained in microfragments of ash
(Wynder and Hoffmann, 1967). It has been suggested that the presence of
high-molecular-weight pigments and other high-molecular-weight components
in tobacco smoke is due to the sharp thermal gradient behind the burning cone
which leads to cellular rupture, thereby expelling these compounds into the
smoke stream where they form the nuclei of the smoke particles (Stedman et
al., 1966).
The smoke from a burning tobacco product is divided into the mainstream
smoke and the sidestream smoke. The heat produced during the burning of
one gram of tobacco is estimated to be 4.5 - 5.0 kcal. The temperature in the
burning cone of a cigar reaches 930°C, in that of a cigarette up to 910°C; it

67
Smoking and Tobacco Control Monograph No. 9
Table 4a
Smoke yields of leading U.S. cigarettes
a
without and with filter tips, little cigars with
filter tips, cigars
b
, and premium cigars
b
1997
Pall Mall Marlboro Swisher King Macanudo
Parameters Non-filter Filter Sweets Edward Premium
Cigarettes Cigarettes Little Cigars Cigars Cigars
Length (mm) 85 85 100 138 176
Weight (g) 1.1 1.0 1.24 8.06 8.01
Puff (No) 11 10 18.5 89.7 119.4
Total Smoke (L) 0.385 0.35 0.4 1.8 2.4
“Tar” (mg) 26 16 24 37 44
CO (mg) 18 14 38 96 97
Nicotine (mg) 1.7 1.1 3.8 9.8 13.3
BaP (ng) 20 16 26.2 96.0 97.4
NNN (ng) 280 200 595 1225 1225
NNK (ng) 160 130 310 1200 1145
a
The cigarettes were smoked under FTC conditions: 1 puff/min, 35 ml, 2-second puff duration
butt length NF, 23 mm; F., 29 mm. (FTC) Pillsbury et al., 1969
b
Little cigars, cigars; and premium cigars were smoked under the conditions of the International Committee for Cigar Smoke
Study (ICCSS): 1 puff/40 seconds, 20 ml, 1.5-second puff duration, butt length 33 mm. Values are averages of 3 runs.
(ICCSS) International Committee for Cigar Smoke Study, 1974.
Abbreviations: BaP, Benzo (
a
) pyrene; NNN, N
1
-nitrosonornicotine; NNK, 4-(methylnitrosamino)
-1-(3-pyridyl)-1-butanone.
Source: Unpublished data Hoffmann, D. American Health Foundation
decreases to 820°C between puffs (Figure 4) (Touey and Mumpower, 1957a;
1957b). Taking four puffs per minute with volumes of 10, 15, or 20 ml, Adams
(1968) reported that peak temperatures of 1,117°C and 1,290°C occur during
smoking of small cigars and 1,139°C and 1,160°C have been measured for
large cigars. Using cigar tobacco in a cigarette, peak temperatures of 944°C
and 970°C were recorded (Table 5).
The temperature of the mainstream smoke emitting from the mouthpiece
with early puffs from cigars and cigarettes lies only a few degrees above room
temperature (25° - 30°C). The temperature of subsequent puffs rises gradually
above 50°C and can even reach 75°C with the last puff of a cigar that is
smoked down to 10 mm (Borowski and Seehofer, 1962).
In general, the pH of the whole smoke of cigars increases from the early
puffs when it is ~ 6.5, to ~ 8.0 for the last (35th) puff. The pH of the puffs
of small cigars increases from 6.5 to 7.4 (14th puff), that of little cigars from
pH 6.5 to 7.5 (9th puff), and that of cigarettes decreases from pH 6.0 to
5.7 (11th puff) (Table 5). This phenomenon is of major significance, since
above pH 6.0 the smoke contains unprotonated (free) nicotine. Thus, the
last puff of a cigar with a pH of 8.0 contains about 50 percent unprotonated

Chapter 3
68
Figure 4
Temperature profiles in the burning cones of cigarettes and cigars
0
0
200
400
600
800
1,000
Temp., °C.
123456
Recorder Chart Travel, In.
Cigarettes
Cigars
78
Chart speed 1 in./min..
91011
Source: Touey and Mumpower, 1951a.

69
Smoking and Tobacco Control Monograph No. 9
Table 5
Comparison of some physicochemical parameters of the mainstream smoke
of cigars and cigarettes
Parameters Cigars Little Cigars Cigarettes
pH
1
3rd Puff 6.5 6.5 6.0
Last Puff 8.0 7.4 5.7
Temperature
2
During puffing, range, °C 1139˚ - 1160˚ n. a. 944 - 970
Between puffs, °C 820 n. a. 800
Reducing Activity
3
(units of DCIP)
Particulate Phase 45.0 n. a. 108.3
Gas Phase 10.1 n. a. 4.9
n. a., not available.
1
Brunnemann and Hoffmann, 1974a;
2
Adams, 1968;
3
Bilimoria and Nisbet, 1972.
nicotine in the vapor phase; that of a small cigar, at pH 7.4, about 30 percent
unprotonated nicotine; and the last puff of a little cigar, at pH 7.5, has
about 32 percent unprotonated nicotine. On the other hand, the smoke of
the U.S. blended cigarette does not contain unprotonated nicotine when
tested under current FTC smoking conditions (Figures 5 and 6) (Brunnemann
and Hoffmann, 1974a). Unprotonated nicotine is present in the vapor phase
of the inhaled smoke; protonated nicotine resides in the particulate phase.
Unprotonated nicotine is absorbed through the mucous membrane of the
oral cavity and delivers a dose of the pharmacoactive agent, that “satisfies”
the primary cigar smoker without his inhaling the smoke (Armitage and
Turner, 1970).
The smoke of fresh (unaged) mainstream smoke of a U.S. blended,
nonfilter cigarette contains about 5 × 10
9
spherical droplets with a particle-
size distribution of 0.1 - 1.0 micron (maximum around 0.2 micron) (Keith
and Derrick, 1961). Slightly less than half of the particles are neutral,
whereas most of the particles carry only one electrical charge and these are
evenly divided between those with negative and those with positive charges
(Norman and Keith, 1975). There is a lack of published data on particle
concentration and particle size distribution in cigar smoke and also on the
electrical charges of cigar smoke particles.
All tobacco smoke products exhibit significant reducing activity.
Studies using the reduction of 2,4-dichloroindophenol as a marker of the
reducing potential of tobacco smoke have shown that cigarette smoke has
a significantly higher reducing potential than cigar or pipe smoke. In
cigarette smoke, about 96 percent of the reducing activity of the total smoke

Chapter 3
70
0
0
10
20
30
40
50
60
70
80
90
100
% of protonated and unprotonated nicotine species
123456
pH
78910
11 12
N
H
N
H
CH
3
N
N
CH
3
N
Source: Brunnemann and Hoffmann, 1974.
Figure 5
Degree of protonation of nicotine in relation to pH.

71
Smoking and Tobacco Control Monograph No. 9
5
0
0
5.5
6.0
6.5
7.0
7.5
8.0
8.5
pH
345678
Puffs
9101112
13 14
20 25
30 35 40
6
4
1
3
2
(1) little cigar I
(2) little cigar II
(3) cigar
(4) Kentucky reference cigarette
(5) blended filter-tipped cigarette (85 mm)
(6) blended cigarette without filter (85 mm)
Source: Brunnemann and Hoffmann, 1974a and 1974b.
Figure 6
pH of total mainstream smoke of various tobacco-products

Chapter 3
72
resides in the particulate phase, while in cigar smoke, 82 percent is found in
the particulate phase (Table 5) (Bilimoria and Nisbet, 1972).
Chemical Tobacco smoke contains more than 4,000 individual components;
Composition about 500 of these occur in the gas phase. The major gas-phase
of Cigar Smoke constituents in cigar smoke are 51.8 - 54.6 volume% nitrogen
(for cigarettes, 55 - 72 vol%), 4.1 - 4.2 vol% oxygen (9.2 - 14.3
Gas Phase* vol%), 15.5 - 16.7 vol% carbon dioxide (6.9 - 13.4 vol%), and
9.7 - 12.7 vol% carbon monoxide (1.9 - 6.3 vol%) (Boyd et al., 1972). These
comparisons strongly indicate that the combustion during puff drawing from
cigars is even less complete (oxygen 4.1 - 4.2 vol%; CO, 1.9 - 6.3 vol%) than
that during cigarette smoking. A primary reason for the low concentration of
O
2
and the high concentration of CO in cigar smoke is the lack of porosity
of the cigar binder and wrapper compared to that of cigarette paper. The
porosity of cigarette paper accelerates the delivery of oxygen into the tobacco
column and the diffusion of certain gaseous components (e.g., CO, CO
2
, NO)
through the paper into the environment.
Table 6 presents select volatile components in the smoke of cigars, little
cigars, and cigarettes. Remarkably, the concentrations of nitrogen oxides
(NO
x
) and ammonia are significantly higher in cigar smoke than in cigarette
smoke. Formation of nitrogen oxides and ammonia is primarily linked to
the nitrate content of the cigar tobacco, the incomplete combustion, and
the lack of porosity of cigar binders and wrappers. The amounts of ammonia
reported in the smoke of cigars and cigarettes may not only originate from
the ammonia produced in the reducing atmosphere of the burning cone but
can also, to a minor extent, come from amides which partially decompose in
the sulfuric acid that is used for trapping the ammonia from the smoke
(Brunnemann and Hoffmann, 1975). In the smoke of cigars, up to 0.8
percent is present as free ammonia at pH levels between 6.8 and 7.2; whereas
cigarette smoke contains only up to 0.01 percent of free ammonia at a pH
between 5.3 and 5.6 (Figure 7) (Sloan and Morie, 1976). The higher
quantities of free ammonia contribute to the pungency of cigar smoke.
Cigar smoke also contains a large number of volatile amines (Pailer et al.,
1969). However, there is a lack of quantitative data. The levels of volatile
N-nitrosamines are also higher in cigar smoke than in cigarette smoke,
again primarily because of the higher nitrate content of the cigar tobacco
compared to that of cigarette tobacco. Furthermore, cigar smoke contains
a large spectrum of volatile agents, such as volatile olefins, dienes (1,3-
butadiene, isoprene, etc.), volatile nitriles, and halogenated hydrocarbons.
* The classification of the tobacco smoke aerosol into gas phase and particulate phase is based on
the separation of the smoke that occurs when it is drawn through a Cambridge glass fiber filter
CM-113. Fifty percent of the components are from the gas phase and pass through the filter.
That portion of the smoke which is trapped on the filter consists of particulate phase
components. These are arbitrary definitions, they do not fully reflect the conditions prevailing
in undiluted, unaged smoke; however, they serve as guidelines.

73
Smoking and Tobacco Control Monograph No. 9
Table 6
Components in mainstream smoke of cigars and cigarettes: gas phase
(values are given for 1.0 g tobacco smoked)
Non-filter Little Filter
Component Cigars Cigarettes Cigars Cigarettes Ref.
Carbon monoxide, mg 39.1 - 64.5 16.3 22.5 - 44.9 19.1 1-3
Carbon dioxide, mg 121 - 144 61.9 47.9 - 97.9 67.8 1-3
Nitrogen oxides (NO
x
), µg 159, 300 160 45, 150 90 - 145 1
Ammonia, µg 30.5 95.3 200, 322 98 4
Hydrogen cyanide, µg 1,035 595 510, 780 448 2
Vinyl chloride, ng n.a. 17.3, 23.5 19.7, 37.4 7.7 - 19.3 5
Isoprene, ng 2,750 - 3,950 420, 460 210 , 510 132 - 990 1.6
Benzene, µg 92 - 246 45, 60 n.a. 8.4 - 97 1,6-8
Toluene, µg n.a. 56, 73 n.a. 7.5 - 112 1,7
Pyridine, µg 49 - 153 40.5 61.3 27.6, 37.0 9
2-Picoline, µg 7.9 - 44.6 15.4 17.0 14.8, 15.6 9
3-+4-Picoline, µg 17.9 - 100 36.1 32.9 12.6, 20.2 9
3-Vinylpyridine, µg 7.0 - 42.5 29.1 21.2 102, 192 9
Acetaldehyde, µg 1,020 960 850, 1,390 94.6 2
Acrolein, µg 57 130 55, 60 87.6 2
N-Nitrosodimethylamine, ng n.a. 16.3 - 96.1 555 7.4 10
N-Nitrosopyrrolidine, µg n.a. 13.8 - 50.7 24.5 6.6 10
n.a., data not available.
References: (1) Wynder and Hoffmann, 1967; (2) Hoffmann et al
.
, 1973; (3) Brunnemann and Hoffmann,
1974b; (4) Brunnemann and Hoffmann, 1975; (5) Hoffmann et al
.
, 1976; (6) Brunnemann et al
.
, 1990; (7)
Osman and Barson, 1964; (8) Appel et al
.
, 1990; (9) Brunnemann et al
.
, 1978; (10) Brunnemann et al
.
, 1977b.
However, the available literature offers few quantitative data for cigar smoke,
except for a report on the presence of vinyl chloride (Hoffmann et al., 1976).
Particulate Phase The particulate phase of tobacco smoke contains at least 3,500
individual components (Roberts, 1988). Most of our knowledge about the
physicochemical nature and composition of tobacco smoke derives from
studies on cigarette smoke.
Only limited research has been done on the chemical composition of
cigar smoke. One would expect cigar smoke chemistry to be qualitatively
similar to that of cigarette smoke, except for differences caused by the use
of additives, by the pH effects, and by the lower concentrations of oxygen
available to support combustion. Cigar smoke may contain components
that derive from additives incorporated into reconstituted tobacco sheets,
and these may be different from additives used in reconstituted tobacco
formulations for cigarettes (Moshy, 1967; Halter and Ito, 1980). The tobacco
of low-yielding cigarettes is often treated with flavor additives (Doull et al.,
1994). Such flavor additives are generally not used for cigars except for some
little cigars with filter tips.

Chapter 3
74
Figure 7
Fraction of free ammonia and methylamine vs. pH.
5
0
0.2
0.4
0.6
0.8
1.0
Fraction of Each Species
6 87 910111213
pH
NH
3
CH
3
NH
2
14
Source: Sloan and Morie, 1976.
Quantitative similarities are seen when one compares the smoke yields of
cigars and cigarettes per gram tobacco smoked (Table 7). This is the case for
the smoke yields of volatile phenols and polynuclear aromatic hydrocarbons
(PAH), compounds primarily pyrosynthesized during smoking. However,
“tar” yields per gram of cigar tobacco burned are somewhat higher because
the nonporous cigar binder and wrapper make the combustion less complete
than that of cigarette tobacco combustion of which is facilitated by highly
porous cigarette paper (Rickert et al., 1985). Also, cigars have larger diameters
than cigarettes which further hinders more complete combustion. The
nicotine yields in the mainstream smoke of cigars are also generally higher
than in the mainstream smoke of cigarettes because the latter contain a
tobacco blend, while most cigars are made solely from burley tobacco that
delivers a weakly alkaline smoke with a high proportion of unprotonated
nicotine.
The significantly lower yields of long-chain paraffin hydrocarbons in
cigar smoke compared to cigarette smoke can, in part, be explained by the
loss of such hydrocarbons during fermentation of the cigar tobacco (Wolf,
1967). The low yields of the long-chain hydrocarbons in cigar smoke are
likely also attributable to the very intense “cracking” of these compounds
during smoking. The high yield of N-nitrosodiethanolamine seen in the
smoke of little cigars was probably related to the treatment of the tobacco
of these little cigars with the sucker growth inhibitor MH-30, maleic hydrazide

75
Smoking and Tobacco Control Monograph No. 9
Table 7
Components in the mainstream smoke of cigars and cigarettes: particulate phase
(values are given for /g tobacco smoked)
Non-filter Little Cigars Filter
Smoke Component Cigars Cigarettes with Filter Cigarettes Ref.
“Tar” (FTC), mg 38.0 - 40.6 16.0 - 36.1 17.4 - 31.8 8.0 - 20.3 1,2,3
Nicotine, mg 2.9 - 3.1 1.7 - 2.65 0.6 - 1.8 0.6 - 1.4 1,2,3
Tridecane, µg 1.2 14.3 4,5
Pentadecane, µg 0.8 14.3 4,5
Eicosane, µg 0.8 27.4 4,5
Docosane, µg 0.6 26.2 4,5
Cholesterol, µg 27.5 49.0
a
6
Camposterol, µg 53.4 57.4
a
6
Stigmasterol, µg 97.5 152
a
6
β-Sitosterol, µg 74.1 82.5
a
6
Phenol, µg 24 - 107 96 - 117 37.0 19.0 - 33.2 2,7
o
-Cresol, µg 19 - 21 22 - 26 4.3 4.2 - 6.8 2,7
m
- and
p
-Cresol, µg 19 - 62 50 - 58 18.0 17 - 23.3 2,7
Catechol, µg 318 129 - 169 178 8
Formic acid, µg 109 - 121 400 9
Acetic acid, µg 286 - 320 900 9
Quinoline, µg 2.0 - 4.1 1.67 0.66 0.62 10
Naphthalene, ng 3,900 - 5,000 1,780 11
1-Methylnaphthalene, ng 1,390 - 1,760 1,110 11
2-Methylnaphthalene, ng 1,720 - 2,130 1,470 11
Acenaphthene, ng 16 50 12,13
Anthracene, ng 119 109 12,13
Pyrene, ng 176 125 12
Fluoranthene, ng 201 125 12
Benz(
a
)anthracene, ng 39 -92.5 92 44.3 40.6 12
Benzo(
a
)pyrene, ng 30 - 51 47 - 58.8 25.7 26.2 12
N-Nitrosodiethanolamine, ng 5.7 4.6 700 38 13
N
1
-Nitrosonornicotine, ng 820 300 7,100 390 14
NNK, ng 4.90 140 5,400 190 14
N
1
-Nitrosoamabasine 4.90 410 2,200 460 14
Copper, ng 40 - 160 < 10 - 100 15
Lead, ng 160 - 280 100 - 510 15
Cadmium, ng 2.0 - 38 16 - 82 15
Zinc, ng 360 - 2,500 120 - 920 15
Nickel, ng 2,500 - 7,000 300 - 600 16,17
a
Small cigar without filter.
b
N
1
-Nitrosoanatabine contains 10 - 15% N
1
-nitrosoanabasine.
References: (1) Hoffmann et al., 1963; (2) Wynder and Hoffmann, 1967; (3) Hoffmann and Wynder, 1972; (4) Spears et al.,
1963; (5) Osman et al., 1965; (6) Schmeltz et al., 1975a; (7) Osman et al., 1963; (8) Brunnemann et al., 1976;
(9) Schmeltz and Schlotzhauer, 1961; (10) Dong et al., 1978; (11) Schmeltz et al., 1976a; (12) Campbell and
Lindsey, 1957; (13) Brunnemann and Hoffmann, 1981; (14) Hoffmann et al., 1979a; (15) Franzke et al., 1977;
(16) Sunderman and Sunderman, 1961; (17) Stahly and Lard, 1977.

Chapter 3
76
diethanolamine. Since 1980-1981, due to an official ban, the use of MH-30
on tobacco has been greatly reduced (Brunnemann and Hoffmann., 1991a).
As to be expected, the smoke of cigars contains significantly higher
amounts of the carcinogenic, tobacco-specific N-nitrosamines (TSNA) than
cigarette smoke (Table 7). A major reason for the elevated levels of TSNA in
cigar smoke is the relatively high concentration of nitrate in cigar tobacco.
During curing and fermentation, nitrate is partially reduced to nitrite, an
important precursor for the N-nitrosation of amines, including alkaloids
like nicotine; nitrate constitutes up to 2.0 percent of the cigar tobacco (Table
3). The nitrosamines formed from nicotine are NNK and NNN (Figure 3).
The latter is also formed in high yields from nornicotine (Hoffmann et al.,
1994). In laboratory animals, NNK and NNN are metabolically activated
by α-hydroxylation which results in the formation of unstable α-hydroxy
nitrosamines. These decompose to yield alkylating agents that react with
the nuclear DNA in vitro and also in vivo (Hecht and Hoffmann, 1989; Hecht,
1996). Lesions formed by this reaction give rise to tumors in the target
organs. NNN elicits carcinoma of the esophagus in rats. In explants of
human esophageal tissue, NNN is also (-hydroxylated, although to varying
extents. The degree of α-hydroxylation of NNN varies between individuals
and is likely related to phenotypic differences (Castonguay et al., 1983). In
this regard, it is of interest to recall that the risk for cancer of the esophagus
among cigar smokers is comparable to that of cigarette smokers (Kahn, 1966;
Schottenfeld, 1984; U.S. Department of Health and Human Services, 1989)
(Chapter 4).
Like most plants, tobacco contains a number of metal ions; a small
percentage of these transfers into the mainstream smoke of tobacco products.
The reported transfer rates into cigar smoke were for lead 2.0 - 6.6 percent
(cigarette smoke 3.4 - 19.7 percent), for zinc 1.0 - 8.5 percent (cigarette smoke
0.6 - 4.6 percent), for cadmium 0.3 - 2.3 percent (cigarette smoke 1.1 - 7.3
percent), and for copper 0.1 - 0.8 percent (cigarette smoke 0.3 - 1.1 percent)
(Franzke et al., 1977). The high transfer rate of nickel into tobacco smoke ((
20 percent) has been explained by the formation of the volatile nickel
carbonyl (bp 43°C) (Sunderman and Sunderman, 1961; Stahly and Lard,
1977). Cigar tobacco was reported to contain between 1.1 and 4.9 (g nickel
per gram tobacco. In inhalation studies, nickel carbonyl (Ni[CO]
4
) induced a
few pulmonary tumors in rats; upon intravenous injection of this compound,
19 out of 20 rats developed lung tumors (International Agency for Research
on Cancer, 1990).
SIDESTREAM Environmental tobacco smoke (ETS) is the term used to describe
SMOKE AND indoor air pollutants derived from burning tobacco products.
ENVIRONMENTAL The major contributor to ETS is the sidestream smoke (SS) that
TOBACCO SMOKE originates between puffs from smoldering cigars, cigarettes,
or pipes. Lesser contributions to ETS come from the smoke
Sources of emitted at the butt end of a burning cigar or cigarette and/or
Environmental from the mouthpiece of a pipe stem, and also from gases diffusing
Tobacco Smoke through cigarette paper. Exhaled smoke also contributes to ETS.

77
Smoking and Tobacco Control Monograph No. 9
It has been known for a long time that the alkaline cigar SS is irritating
to eyes, ears, and throats of people, especially in enclosed environments with
limited ventilation, such as offices and other workplaces and conveyances.
The ph levels of cigar Tobacco and of its smoke are slightly alkaline
(Wolf, 1967; Brunnemann and Hoffmann, 1974a). This contributes to the
unpleasant odor of cigar butts, which contain partially unprotonated, readily
volatilizing ammonia, pyridine, methyl- and ethylpyridines, 3-vinylpyridine,
2,4-, 2,6-, and 3,s-dimethylpyridines as well as allylalcohol, ethylmercaptan,
volatile phenols, aliphatic nitriles, and benzonitrile (Peck et al., 1969; Adler
et al., 1971).
The Physicochemical SS is primarily formed in the burning cones and hot zones
Nature of Sidestream of cigars, cigarettes, and pipes between the drawing of puffs.
Smoke The smoldering tobacco releases more of many compounds
into the SS than into mainstream smoke (MS).
This applies especially to those agents that are preferably formed in
reducing atmospheres, namely ammonia, aliphatic and aromatic amines, and
volatile N-nitrosamines (Table 8). When SS is generated, several compounds
result from the degradation of tobacco constituents of low volatility. These
include benzene, toluene, 3-vinylpyridine (from the Nicotiana alkaloids), and
polynuclear aromatic hydrocarbons (PAH). Smoke components that are
formed by oxidation, such as catechol and hydroquinone, are released into
SS in significantly lower amounts than into MS (Schmeltz et al., 1975a,b;
Schmeltz et al., 1979; Klus, 1990; Guerin et al., 1992).
Because of the release of relatively large quantities of ammonia, the pH
of the SS of cigarettes is neutral (MS slightly acidic) and that of cigars is
alkaline (Figure 8; see Figure 6 to compare with the pH of MS). Therefore,
the SS of both cigarettes and cigars contains a greater proportion of
unprotonated nicotine and ammonia than the MS (Figures 5 and 7;
Brunnemann and Hoffmann, 1974a; Morie, 1972).
Few physicochemical parameters of cigar SS are available in the accessible
literature (Table 9). It is likely that they are generally similar to those of
cigarette SS. Under standardized machine-smoking conditions (FTC method)
(Pillsbury et al., 1969), the generation of MS from cigarettes requires, on
average, 10 puffs of 35 ml each and a total of 20 seconds, while the
formation of SS occurs over 550 seconds. During these periods, 347 mg
tobacco are burned to generate MS and 411 mg tobacco are burned to
produce SS. In the MS of a nonfilter cigarette one finds 10.5 × 10
12
particles;
in the SS, 35 × 10
12
particles (Scassellati-Sforzolini and Savino, 1968); the
particle sizes range from 0.1 to 1.0 µm in MS and from 0.01 to 0.8 µm in SS,
with means of 0.4 µm and 0.32 µm, respectively (Carter and Hasegawa, 1975;
Hiller et al., 1982). Ingebrethsen and Sears (1985) reported that particle size
declines in line with the degree of dilution of SS by air. Diluting SS from
226 µg/m
3
to 26 µg/m
3
and down to 1.4 µg/m
3
reduces the median diameter
from 0.210 to 0.196 and to 0.185 µm, while the percentage of particles with
diameters <0.10 µm increases from about 39 to 54, and to 73 percent of the

Chapter 3
78
Constituent Amount in MS Range in SS/MS
Catechol 100-360 µg 0.6-0.9
Hydroquinone 110-300 µg 0.7-0.9
Aniline 360 ng 30
2-Toluidine 160 ng 19
2-Naphthylamine 1.7 ng 30
4-Aminobiphenyl 4.6 ng 31
Benz[
a
]anthracene 20-70 ng 2-4
Benzo[
a
]pyrene 20-40 ng 2.5-3.5
Cholesterol 22 µg 0.9
γ-Butyrolactone 10-22 µg 3.6-5.0
Quinoline 0.5-2 µg 8-11
Harman 1.7-3.1µg 0.7-1.7
N’
-Nitrosonornicotine 200-3,000 ng 0.5-3
NNK 100-1,000 ng 1-4
N
-Nitrosodiethanolamine 20-70 ng 1.2
(continues)
Table 8
Distribution of select constituents in fresh, undiluted mainstream smoke and diluted sidestream
smoke from nonfilter cigarettes
Constituent Amount in MS Range in SS/MS
Vapor phase
Carbon monoxide 10-23 mg 2.5-4.7
Carbon dioxide 20-40 mg 8-11
Carbonyl sulfide 18-42 µg 0.03-0.13
Benzene 12-48 µg 5-10
Toluene 100-200 µg 5.6-8.3
Formaldehyde 70-100 µg 0.1-≅50
Acrolein 60-100 µg 8-15
Acetone 100-250 µg 2-5
Pyridine 16-40 µg 6.5-20
3-Methylpyridine 12-36 µg 3-13
3-Vinylpyridine 11-30 µg 20-40
Hydrogen cyanide 400-500 µg 0.1-0.25
Hydrazine 32 ng 3
Ammonia 50-130 µg 40-170
Methylamine 11.5-28.7 µg 4.2-6.4
Dimethylamine 7.8-10 µg 3.7-5.1
Nitrogen oxides 100-600 µg 4-10
N
-Nitrosodimethylamine 10-40 ng 20-100
N
-Nitrosodiethylamine ND-25 ng <40
N
-Nitrosopyrrolidine 6-30 ng 6-30
Formic acid 210-490 µg 1.4-1.6
Acetic acid 330-810 µg 1.9-3.6
Methyl chloride 150-600 µg 1.7-3.3
Particulate phase
Particulate matter 15-40 mg 1.3-1.9
Nicotine 1-2.5 mg 2.6-3.3
Anatabine 2-20 µg <0.1-0.5
Phenol 60-140 µg 1.6-3.0

79
Smoking and Tobacco Control Monograph No. 9
Table 8
(continued)
Cadmium 100 ng 7.2
Nickel 20-80 ng 13-30
Zinc 60 ng 6.7
Polonium-210 0.04-0.1 pCi 1.0-4.0
Benzoic acid 14-28 µg 0.67-0.95
Lactic acid 63-174 µg 0.5-0.7
Glycolic acid 37-126 µg 0.6-0.95
Succinic acid 110-140 µg 0.43-0.62
National Research Council, 1986.
total ETS particles. In respect to particle sizes in the MS and SS of cigars, it is
likely that similar parameters prevail; however, precise data are currently
not available.
Environmental The tobacco smoke released into the environment from a burning
Tobacco Smoke cigarette, cigar, or pipe, and the exhaled smoke (that portion not
retained by the smoker) is usually diluted by air several hundred-fold and
often a thousand-fold before the ETS-polluted aerosol is inhaled
(International Agency for Research on Cancer, 1986; U.S. Department of
Health and Human Services, 1986; National Research Council, 1986; Guerin
et al., 1992). However, to date only one model study with cigar smoke as a
source for ETS has been reported (Nelson et al., 1997). It involved the
concurrent smoking of three cigars of one brand by three men over a 10-
minute period in a 45 m
3
chamber. The environmental conditions were
static, i.e., there was neither air supply nor recirculation of the air in the
chamber. Table 10 compares ETS data from this model study with the data
from a model study with six cigarette smokers located for 10 minutes in the
same chamber under identical (static) chamber conditions (Nelson et al.,
1996 and 1997). Clearly, the smoking of three cigars by three smokers
during 10 minutes polluted the air significantly more with CO (16.9 to 25.3
ppm), nitrogen oxides (412 to 520 ppb), nicotine (168 to 450 µg/m
3
), and
respirable suspended particulate matter (RSP; 1,520 to 5,770 µg/m
3
) than the
smoking by six cigarette smokers which generated 0.629 to 0.782 ppm CO,
226 to 461 ppb nitrogen oxides, 49 to 61 µg/m
3
nicotine, and 1,170 to 1,960
µg/m
3
RSP (Table 10). The greater degree of ETS pollution generated by the
three cigar smokers can be explained, at least in part, by the fact that these
cigar smokers burned cumulatively between 21.4 g and 33.9 g of tobacco
while the six cigarette smokers burned only between 3.77 g and 4.69 g
tobacco during the same time. This model study documents clearly what has
been assumed, namely that cigar smokers pollute enclosed environments to a
significantly higher degree than cigarette smokers. Studies of the levels of
CO produced under actual cigar smoking conditions are described in
Chapter 5 (Repace et al., 1998).
ETS differs from freshly generated mainstream smoke in a number of
ways. The conditions under which MS is formed are very different from
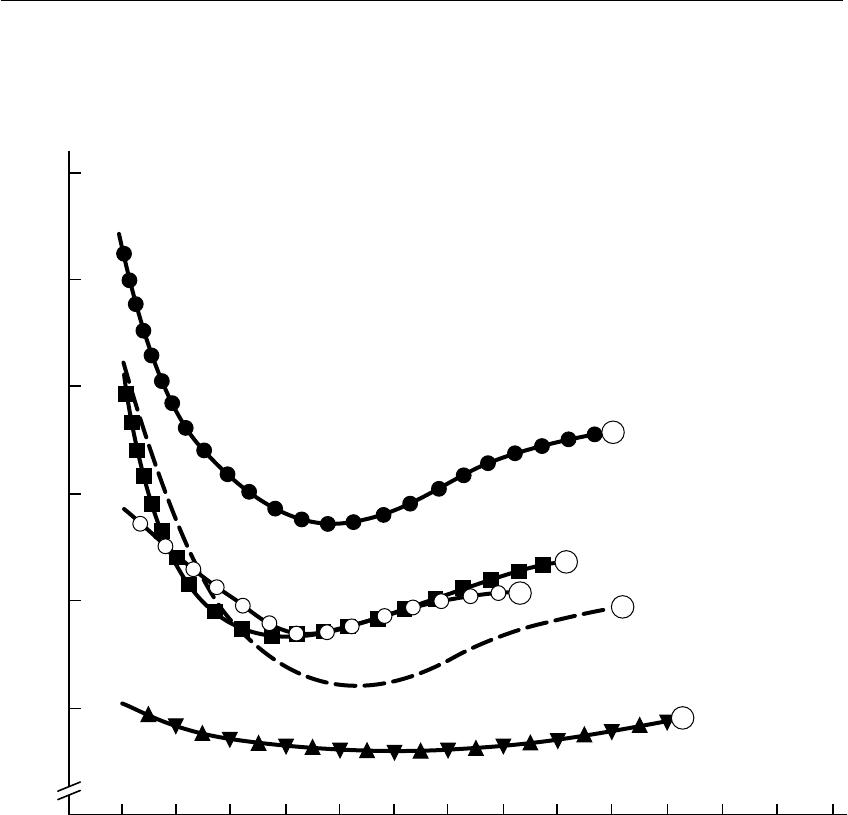
Chapter 3
80
0
0
6.5
7.0
7.5
9.0
8.5
8.0
pH
1 32 45678
Puffs
910111213 14
1
4
2
3
5
those prevailing during SS formation, and the latter is the main contributor
to ETS. The pH of SS is different from that in the MS of cigars and cigarettes
(Figures 6 and 8), reflecting the presence of free ammonia and creating major
differences in the degree of unprotonated nicotine (Figures 5 and 7). In
addition, with the higher degree of air dilution of SS, more nicotine
evaporates from the particulate phase into the vapor phase. Eudy et al. (1986)
reported that 90 - 95 percent of the nicotine is present in the vapor phase of
(1) little cigar I
(2) little cigar II
(3) French (black tobacco) cigarette
(4) Kentucky reference cigarette
(5) blank (air)
Source: Brunnemann and Hoffmann, 1974a and 1974b.
Figure 8
pH of total sidestream smoke of various tobacco-products

81
Smoking and Tobacco Control Monograph No. 9
Table 9
Some selected compounds in the sidestream smoke of cigars, little cigars, nonfilter cigarettes
and filter cigarettes (values are given for 1 g tobacco burned)
Nonfilter Little Cigar Filter
Compound Cigars Cigarette with Filter Tips Cigarette Ref.
Ammonia, mg 7.18 (44) 9.34 (47) 7.14 (13) 1
6.11 (64) 12.9 (40)
Hydrogen cyanide, µg 134 (0.85) 114 (0.17) 167 (0.37) 2
141 (0.30)
Pyridine, µg 665 - 800 (5013) 420 (10) 3
2-Picoline, µg 170 - 255 (6-20) 160 (10) 3
3- and 4-Picoline, µg 600 - 930 (–51) 380 (13) 3
3-Vinylpyridine, µg 595 - 900 (14-80) 800 (28) 3
NDMA, ng 473 (6.4) 930 (50) 2,280 (412) 950 (129) 4,5
NEMA, ng 15 (1.4) 74 (30) 97 (15) 129 (95) 4,5
NDEA, µg 72.6 (35.3) 29 (26) 56 (89) 4,5
NPYR, µg 128 (10.5) 410 (27.3) 922 (32) 758 (89) 4,5
Cholesterol, µg 23.6 (0.9) 9.5 (0.6)
a
Campesterol, µg 32.5 (0.) 12.5 (0.8)
a
6
Stigmasterol, µg 67.0 (0.7) 11.8 (0.8)
a
6
β-Sitosterol, µg 35.0 (0.5) 9.8 (0.8)
a
6
NNN, µg 4.27 (5.2) 2.13 (7.1) 1.14 (0.16) 0.19 (0.48) 7
NNK, µg 4.03 (8.3) 0.63 (3.7) 1.05 (0.15) 0.24 (1.3) 7
NAB, µg 0.34 (0.82) 0.71 (0.34) 0.19 (0.41) 7
Numbers in parentheses SS/MS.
a
Little cigar without filter.
References: (1) Brunnemann and Hoffmann, 1974; (2) Brunnemann et al., 1977a; (3) Brunnemann et al., 1978;
(4) Brunnemann et al., 1977b; (5) Brunnemann and Hoffmann, 1991; (6) Schmeltz et al., 1975a and
1975b; (7) Hoffmann et al., 1979.
ETS. The particle mass median diameter in ETS is significantly smaller than
the particle diameter of inhaled MS (Carter and Hasegawa, 1975;
Ingebrethsen and Sears, 1985). Furthermore, even compounds with
relatively high molecular weight, such as the paraffin hydrocarbons C
25
H
52
to
C
34
H
70
, have been found to be present in the vapor phase of ETS to a
significant degree (Ramsey et al., 1990).
Exhaled smoke may also contribute more to the particulate than to the
vapor phase of ETS (Baker and Procter, 1990).
The time elapsing between generating and inhaling mainstream smoke is
only fractions of seconds or, at most, seconds; thus, chemical reactions
between constituents of freshly generated MS are limited compared to
reactions during the aging of ETS, which may go on for periods up to a few
hours and may be influenced by various atmospheric conditions. Certain
ETS constituents may react with other materials in an enclosed environment,
or components may be absorbed by textiles or by the surfaces of furniture.

Chapter 3
82
Table 10
Contribution of cigar and cigarette smoke to environmental tobacco smoke model
studies in a 45 m
3
room operated in the static mode
a
Cigars
b
Cigarettes
c
ETS - component C F D B E A FF FFLT ULT 100
Tobacco burned, g 7.11 7.33 10.5 7.77 10.3 6.53 0.7 0.661 0.629 0.782
CO, ppm 20.0 16.8 22.8 18.3 24.7 25.3 6.3 6.0 6.4 7.7
NO
x
, ppb 572 412 445 526 472 520 234 226 242 261
3-Ethenylpyridine, µg/m
3
114 125 136 149 128 185 25 27 34 27
Nicotine, µg/m
3
168 202 283 290 169 450 51 61 49 56
RSP, µg/m
3
1810 1520 2920 2280 1280 5770 1440 1330 1170 1960
Solanesol, µg/m
3
43 26 16 74 21 102 45 44 35 53
a
No air supply, no air recirculation.
b
Three cigar smokers smoked the same cigar brands concurrently for 10 minutes.
c
Six cigarette smokers smoked the same cigarette brands concurrently.
Abbreviations: ETS, environmental tobacco smoke; Nox, nitrogen oxide plus nitrogen dioxide; RST, respirable suspended particulate matter; FF, full flavor cigarette;
FFLT, full flavor-low “tar”; ULT, ultra low “tar” cigarette; 100, full flavor-low “tar” 100 mm cigarette.
References: Nelson et al., 1997; Nelson et al., 1996.

83
Smoking and Tobacco Control Monograph No. 9
This is the case with nicotine. The ratio between smoke components in ETS
thus undergoes changes over time.
Tables 11 and 12 list some data for specific constituents of the vapor
phase and of the particulate phase of ETS. These tables present only a
fraction of the data that are known about ETS composition. (More detailed
information is in the following sources: U.S. Department of Health and
Human Services, 1986; National Research Council, 1986; Guerin et al., 1992.)
The tables do indicate some elevation in the concentration of toxic agents
in enclosed environments polluted with ETS compared to outdoor air.
Moreover, there are concerns about an apparent ongoing TSNA formation
during aging of ETS, yet there are no data in the literature to verify this
phenomenon.
Tables 11 and 12 also list trace amounts of those agents in ETS that
IARC (1987) regards as either “carcinogenic to humans,” or as “probably or
possibly carcinogenic to humans.” These include the human carcinogens
benzene and the aromatic amines 2-naphthylamine and 4-aminobiphenyl, as
well as the animal carcinogens 1,3-butadiene, isoprene, acrylonitrile,
formaldehyde, acetaldehyde, volatile N-nitrosamines, tobacco-specific
N-nitrosamines, and various polynuclear aromatic hydrocarbons.
TOXICITY AND As stated earlier, tobacco smoke contains at least 4,000
CARCINOGENICITY compounds (Roberts, 1988). At first glance, it appears to
OF CIGAR SMOKE be an insurmountable task to identify all of the individual
chemicals and groups of chemicals that are involved in the toxicity or
carcinogenicity of the smoke of cigars, cigarettes, or pipes. However,
intensive research in the tobacco sciences and advances in our
understanding of toxicology and carcinogenesis during the past five decades
have enabled scientists to define which agents, or groups of agents, are major
contributors to the biologic activities of tobacco smoke (U.S. Department of
Health and Human Services, 1989; Hoffmann et al., 1997).
Toxicity Tables 6 and 7 list several smoke constituents that contribute to the
overall toxicity and carcinogenicity of cigar smoke. Carbon monoxide and
nicotine are major contributors to the acute toxicity of cigar smoke. Among
agents which also add to the acute toxicity of cigar smoke are nitrogen
oxides, hydrogen cyanide, ammonia, and volatile aldehydes.
Human hemoglobin has 210 times greater affinity for carbon monoxide
than for oxygen. Inhaling tobacco smoke with up to 6 volume percent of CO
diminishes the oxygen carrying capacity of the blood. Carboxyhemoglobin
(COHb) concentration in the blood of nonsmokers amounts to about 0.5
percent, whereas in smokers it may reach 8 - 9 percent. The relationship
between smoking and CO intoxication has received little attention. In 1969,
Hamill and O’Neill reported two cases of CO intoxication of cigar smokers.
Both were secondary cigar smokers, practicing inhalation of the smoke just as
they did with cigarettes. One smoked 40 - 50 cigars, the other up to 15 cigars
per day. Both had CO intoxication with polycythemia and decreased arterial
oxygen saturation. Their COHb concentrations were 13 - 15 percent and 12 -
13 percent, respectively. In primary cigar smokers, COHb amounts to about

Chapter 3
84
Table 11
Concentrations of ETS-compounds in indoor air - vapor phase*
Concentration
Compound Mean Range Reference
Carbon Monoxide, ppm
25 offices 2.8 Szadkowski et al., 1976
Nonsmoking offices 2.6 Szadkowski et al., 1976
Office: 72m
3
-40 cigs/day < 2.5 - 4.6 Harke, 1974
Office: 78m
3
-70 cigs/day < 2.5 - 9.0 Harke, 1974
Offices - 66, urban area 2.3 ± 2.0 0.1 - 10.5 Guerin et al., 1992
Offices - 57, control-outdoor 2.5 ± 2.3 NR - 10.4 Guerin et al., 1992
Working areas - 221 situations 2.2 0.0 - 31.9
controls - 450 situations 2.1 0.0 - 21.9 Guerin et al., 1992
Restaurants, 49 3.4 ± 1.2 2.0 - 7.9 Guerin et al., 1992
13 controls 3.0 ± 0.6 2.0 - 4.1 Guerin et al., 1992
Restaurants, 99 4.2 ± 2.7 1.5 - 42.3 Guerin et al., 1992
99 outdoor controls 2.5 ± 2.1 0.3 - 13.7 Guerin et al., 1992
Nitrogen Oxides, ppb
10 Office Buildings, NO
2
24 ± 7 11 - 32 Guerin et al., 1992
outdoor controls, NO
2
27 ± 11 Guerin et al., 1992
5 Office Buildings, NO
2
16 ± 5 7 - 20 Guerin et al., 1992
outdoor controls 14 ± 6 Guerin et al., 1992
44 workrooms
a
, 227 determ., NO 82 Weber and Fischer, 1986
44 workrooms
a
, 227 determ., NO
2
64 Weber and Fischer, 1986
44 workrooms
b
, 102 determ., NO 66 Weber and Fischer, 1986
44 workrooms
b
, 102 determ., NO
2
49 Weber and Fischer, 1986
Aliphatic Hydrocarbons µg/m
3
Ethane 56 - 100 Löfroth et al., 1989
outdoor air, control 8 - 9
Propane 30 - 70 Löfroth et al., 1989
outdoor air, control 6 - 7
1,3-Butadiene
c
11 - 19 Löfroth et al., 1989
outdoor air, control < 1 - 1
(Bar at 3 different days) 3.5 27 - 4.5 Brunnemann et al., 1990
Isoprene
c
, 6 taverns 85 - 150 Löfroth et al., 1989
outdoor air, control < 1 - 1
4 restaurants 42.6 16.6 - 90 Higgins et al., 1991
1 bar, 3 samplings 97 60 - 106 Brunnemann et al., 1990
Aromatic Hydrocarbons, µg/m
3
Benzene
a
, 6 coffee houses 100 50 - 150 Badré et al., 1978
3 train spaces 68 20 - 100 Badré et al., 1978
cars, ventilation 30 20 - 40 Badré et al., 1978
cars, no ventilation 150 Badré et al., 1978
trains Löfroth et al., 1989
outdoor air, control 6 -
bar, 3 samplings 31 31 - 36 Brunnemann et al., 1990

85
Smoking and Tobacco Control Monograph No. 9
Table 11
(continued)
Concentration
Compound Mean Range Reference
Toluene, coffee house 448 40 - 1,040 Badré et al., 1978
4 train compartments 1128 180 - 1,870 Badré et al., 1978
car, ventilation 500 Badré et al., 1978
car, no ventilation 30 50 - 70 Badré et al., 1978
bar, 3 days 55 41 - 80 Brunnemann et al., 1990
Formaldehyde
b
, (tavern) µg/m
3
89 - 109 Löfroth et al., 1989
Acetaldehyde
c
(tavern) µg/m
3
183 - 204 Löfroth et al., 1989
coffees 460 170 - 630 Badré et al, 1978
trains 546 65 - 1,040 Badré et al, 1978
automobile - ventilation 370 260 - 480 Badré et al, 1978
automobile - no ventilation 1080 Badré et al, 1978
Acetonitrile bowling alley, µg/m
3
75.9 Higgins et al., 1991
residence, smoke 17.3 Higgins et al., 1991
residence, no smoke 3.4 Higgins et al., 1991
4 restaurants 17.5 2.4 - 48.9 Higgins et al., 1991
Acrylonitrile
b
bowling alley, µg/m
3
1.8 Higgins et al., 1991
residence, smoker 0.8 Higgins et al., 1991
residence, nonsmoker 0.6 Higgins et al., 1991
4 restaurants 0.6 0.1 - 1.9 Higgins et al., 1991
Pyridine bowling alley, µg/m
3
38 Higgins et al., 1991
residence, smoker 6.5 Higgins et al., 1991
residence, nonsmoker 0.6 Higgins et al., 1991
4 restaurants 5.0 0.8 - 15.7 Higgins et al., 1991
3-Vinylpyridine bowling alley, µg/m
3
3.6 Higgins et al., 1991
residence, smoker 6.4
residence, nonsmoker 3.2 ND
4 restaurants 3.2 0.2 - 6.4
415 nonsmokers, smoker’s home Jenkins et al., 1996
16 h breathing some samples 14.0 Jenkins et al., 1996
520 nonsmokers, workplace
8 h breathing some samples 5.52
Volatile N-Nitrosamines µg/m
3
N
-Nitrosodimethylamine
b
train, beverage car 0.11 - 0.13 Brunnemann and
Hoffmann, 1978
bar 0.24 Brunnemann and
Hoffmann, 1978
discotheque 0.09 Brunnemann and
Hoffmann, 1978
The concentrations of individual components in ETS reported before 1985-1988 are, in general, significantly higher
than those reported today. This is a consequence of measures to limit indoor smoking or to ban smoking entirely,
as in the case of US airlines.
a,b,c
These compounds are all carcinogenic to animals. According to the International Agency for Research
on Cancer (1987), compounds are:
a
carcinogenic to humans;
b
probably carcinogenic to humans; and
c
possibly carcinogenic to humans.

Chapter 3
86
Table 12
Concentrations of ETS-compounds in indoor air - particulate phase*
Concentration
Compound Mean Range Reference
Nicotine**, µg/m
3
(residences, 47 houses) 2.2 0.1 - 9.4 Lederer & Hammond, 1991
(residences, 3 houses) 11.1 7.6 - 14.6 Muramatsu et al
.
, 1984
(offices, 44) 1.1 0.0 - 16.0 Weber & Fischer, 1986
(offices, 10) 2.3 0.3 - 6.7 Thompson et al
.
, 1989
(restaurants, 6 coffees) 25 - 52 Badré et al
.
, 1978
(restaurants, 5 coffees) 14.8 7.1 - 27.8 Muramatsu et al., 1984
(cafeterias, 3) 26.4 11.6 - 42.2 Muramatsu et al., 1984
2.3 - 4.4 Thompson et al
.
, 1989
(bars, 2) 8.4 4.7 - 13.0 Kirk et al
.
, 1968
(bars, 5) 7.4 2.0 - 13.1 Miesner et al
.
, 1989
(pubs, 3) 31 Muramatsu et al
.
, 1987
Automobile (natural ventilation) 65 Badre et al
.
, 1978
(ventilation) 1,010 Badre et al
.
, 1978
Trains (8) 16.4 8.6 - 26.1 Muramatsu et al
.
, 1984
Airplanes, (48 smoking seats) Oldaker & Conrad, 1987
(20 nonsmoking seats) 5.5 ≤0.08 - 40.2 Oldaker & Conrad, 1987
Aromatic Amines, µg/m
3
2-Naphthylamine
a
(offices) 0.27 - 0.34
4-Aminobiphenyl
a
0.1
Carcinogenic PAH, µg/m
3
Benzo(
b
)fluoranthene
c
(rooms) 0.132 - 0.578 Gundel et al
.
, 1990
(outdoor air) 0.007 - 0.098 Gundel et al
.
, 1990
Benzo(
a
)pyrene
b
(common smoking conditions) 0.2 - 10 Guerin et al
.
, 1988
(heavy smoking conditions) 10 - 20 Guerin et al
.
, 1988
Benzo(
a
)pyrene (room air) 3.25 Adlkofer et al
.
, 1989
Tobacco-Specific
N
-Nitrosamines, µg/m
3
N
1
-Nitrosonornicotine
c
(3 bars) 11.8 4.3 - 22.8 Brunnemann et al
.
, 1992
(2 restaurants) nd. - 1.8 Brunnemann et al
.
, 1992
(2 train comparts.) n.d. Brunnemann et al
.
, 1992
(smoker’s home) n.d. Brunnemann et al
.
, 1992
4-(Methylnitrosamino)-1-(3-pyridyl)-1-butanone
c
(3 bars) 14.9 9.6 - 23.8 Brunnemann et al
.
, 1992
(2 restaurants) 1.4, 3.3 Brunnemann et al
.
, 1992
(2 train comparts.) 4.9 - 5.2 Brunnemann et al
.
, 1992
(smoker’s home) 1.9 Brunnemann et al
.
, 1992
*See footnote of Table 9.
**Although in ETS, generally, 90-95% of the nicotine is in the vapor phase for didactic reasons, nicotine in ETS is listed
under “Particulate Phase”.
n = not detected.
a,b,c
The compounds are all carcinogenic to animals. According to the International Agency for Research on Cancer (1987),
compounds are:
a
carcinogenic to humans;
b
probably carcinogenic to humans; and
c
possibly carcinogenic to humans.

87
Smoking and Tobacco Control Monograph No. 9
2 percent; in secondary cigar smokers, the values are usually higher, up to 11
percent (Castleden and Cole, 1973).
Ciliatoxic Development of squamous epithelium metaplasia is likely to be
Agents accentuated by the presence of ciliatoxic compounds that cause mucus
stagnation. This knowledge motivated several investigators to identify the
ciliatoxic agents in tobacco smoke in in vitro and in vivo assays (Kensler and
Battista, 1963; Wynder et al., 1963; Bernfeld et al., 1964; Dalhamn and
Rylander, 1966). Battista (1976) tabulated the existing knowledge about
the chemical nature of ciliatoxic agents in tobacco smoke (Table 13).
Although the concentrations of ciliatoxic agents per volume of cigar smoke
are somewhat higher than those in cigarette smoke, the lungs of primary
cigar smokers will only be exposed to a fraction of these toxic agents because
these smokers tend to inhale far less of the smoke than cigarette smokers do.
However, secondary cigar smokers who are inhaling this smoke into their
lungs will have significant exposure to ciliatoxins.
Genotoxicity During the past two decades, in vitro and in vivo short-term assays have
been employed to establish the genotoxicity of xenobiotic agents in order
to gain an indication of their carcinogenic potential. Genotoxic agents have
the ability to form DNA adducts and DNA-oxidation products in cellular
nuclei, or otherwise change the configuration of DNA. So far, only one
short-term test for the genotoxicity of cigar “tar” has been reported. Sato et
al. (1977) tested five cigar “tars” for their mutagenic activities on the
Salmonella typhimurium tester strains TA98 and TA100 and compared these
activities with those of eight cigarette “tars.” The genotoxic agents in these
“tars” were metabolically activated with an S9 liver fraction of untreated rats.
The number of revertants induced by 1 mg of cigar “tar” in TA100 was 922 ±
63; those in TA98 were 2,320 ± 305. One mg of cigarette “tar” caused, on
average 735 ± 101 revertants in TA 100 and 1,460 ± 317 revertants in TA98.
The mutagenicity of cigar “tars” was significantly higher (in TA100, p = 0.01;
in TA98, p = 0.004) when compared to cigarette “tars.”
Carcinogenicity The first report on the carcinogenicity of the “tar” from cigars was
and Carcinogenic conducted with denicotinized “tar” by Croninger et al., 1958
Agents (Table 14). Subsequently, three additional bioassays with cigar
“tar” were reported in the literature (Table 14). Several of these studies,
especially the study by Davies and Day (1969) reported a significantly higher
tumorigenic activity with cigar “tar” in mouse skin than with cigarette “tar,”
as reflected in the induction of both papilloma and carcinoma in the skin.
This result was expected since cigar “tar” contains higher concentrations of
carcinogenic PAH.
Table 15 lists those agents in cigarette and cigar smoke that, according
to the International Agency for Research on Cancer (1987, 1990, 1991,
1993a, 1993b, 1994, 1996), are animal carcinogens; ten of these are also
carcinogenic in humans. Because data for cigar smoke are lacking, the yields
of carcinogens in the smoke of cigarettes made exclusively from bright and
blended tobacco are compared with those in the smoke of cigarettes made
exclusively from burley tobacco (Table 16). Because cigars are primarily

Chapter 3
88
Table 13
Vapor phase constituents with high ciliatoxic potency -
in vitro
Amount in Smoke (µg/puff)
Compound Potency Typical (Range)
Hydrogen Cyanide +++ 38 (16-63)
Formaldehyde +++ 5 (2.5-11)
Acrolein +++ 10 (5.6-10.4)
Sulfur Dioxide +++ <1
Crotonaldehyde ++ 1.6
2,3-Butanedione ++ 12
Ammonia ++ 1
Nitrogen Dioxide ++ <10
Methacrolein + 1
Vinyl Acetate + 0.5
Nitric Oxide + 60 (12-75)
ED
50
(8 puffs)
Score (µg/puff)
+++ High = ≤50
++ Moderate = 50-100
+ Low = 100-500
Vapor phase constituents with low ciliatoxic potency - in vitro
Aliphatic Hydorcarbons Ethers
Cyclopentane Furan
Cyclopentene 2-Methylfuran
Cis
-1,3-Pentadiene 2,5-Dimethylfuran
Trans
-1,3-Pentadiene
2-Methyl-1,3-Butadiene
Esters
Limonene Methyl Formate
Methyl Acetate
Aromatic Hydrocarbons
Ethyl Acetate
Benzene
Toluene
Nitriles
Acetonitrile
Aldehydes
Propionitrile
Acetaldehyde Acrylonitrile
Propionaldehyde Isobutyronitrile
Butyraldehyde Methacrylonitrile
Valeraldehyde
Isovaleraldehyde
Sulfur Compounds
Pivaldehyde Hydrogen Sulfide
2-Methylvaleraldehyde
Other Nitrogenous Compounds
Nitrous Oxide
Ketones
Acetone Miscellaneous
2-Butanone Carbon Dioxide
2-Pentanone Carbon Monoxide
3-Pentanone Phenol Vapor
+≥ 500 µg/puff needed to achieve activity comparable to cigarette smoke. None of the above are present in cigarette smoke
at levels ≥ 20 % of the amount needed for biological activity.
Source: Battista, 1976
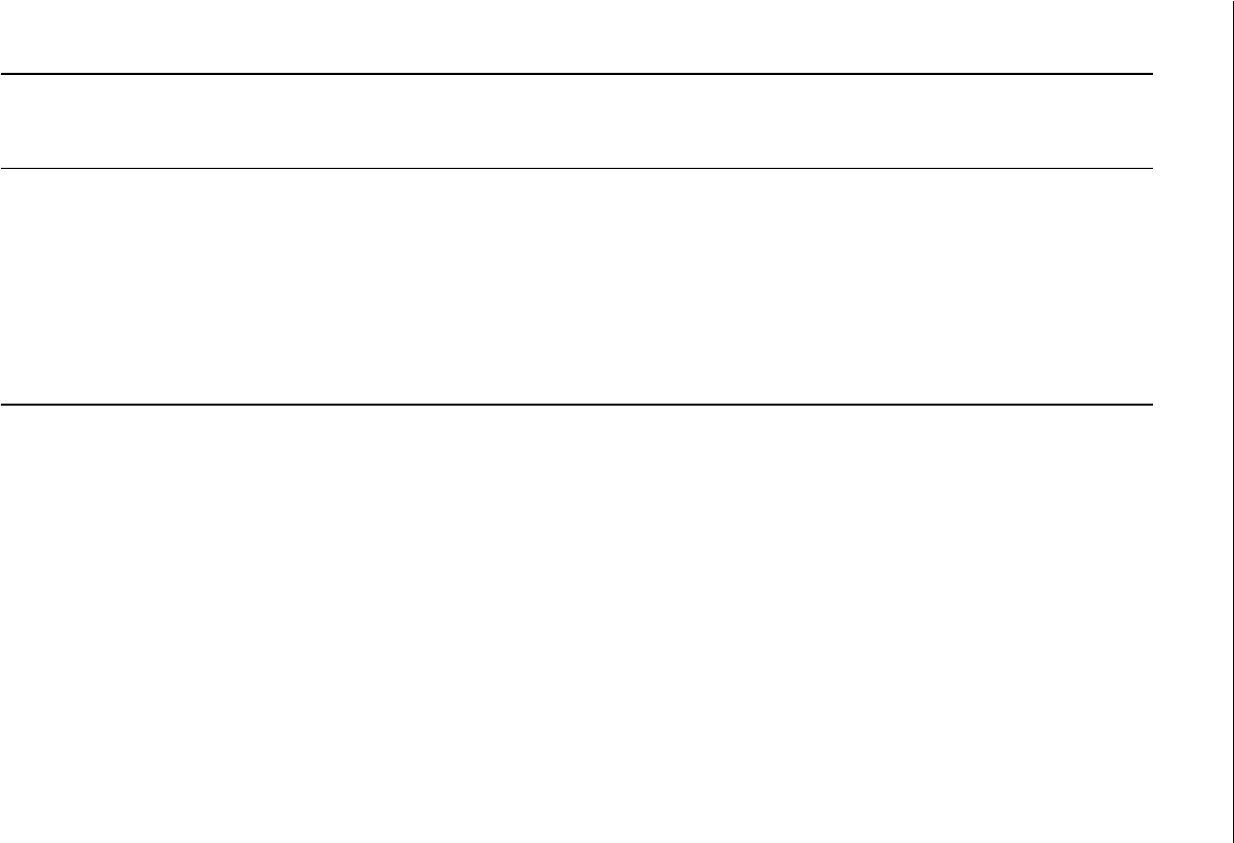
89
Smoking and Tobacco Control Monograph No. 9
Table 14
Comparison of the induction of papilloma and carcinoma in the skin of mice with “tars” from cigars and cigarettes
“Tar”
dose per Applications Cigar “Tar” “Tar” from Control Cigarettes
Mouse % “Tar” application, each # % % # % %
Strain Sex Suspension mg week mice papilloma cancer mice papilloma cancer Reference
Swiss F 33 25 3 100 33 18 Croninger et al
.
, 1958
CAF
1
F 33 25 3 100 50 10 Croninger et al
.
, 1958
Swiss F 50 - NF 40 3 100 65* 41 100 47 37 Croninger et al
.
, 1958
Swiss M,F 50 3 42 40 40 24 Kensler, 1962
Swiss M,F 50 3 42 40 34 34 Kensler, 1962
CAF
1
M 50 21 3 87 27.5 15 86 27 15 Homburger et al
.
, 1963
CAF
1
F 50 21 3 82 37.5* 19 96 15 23 Homburger et al
.
, 1963
ICI - Albino F 25 75 2 144 44.4** 27.1** 144 27.8 13.2 Davies & Day, 1969
ICI - Albino F 12.5 37.5 2 144 20.8* 11.1** 144 7.6 0.7 Davies & Day, 1969
ICI - Albino F 6.25 18.7 2 144 6.3 2.1 Davies & Day, 1969
Abbreviations: NF, nicotine free “tar.”
Cigar “tar” induces significantly more papilloma or carcinoma than the cigarette control “tar.”
*p ≤ 0.05; ** p ≤0.01.

Chapter 3
90
Table 15
Carcinogens in tobacco and tobacco smoke
IARC evaluation
evidence of
carcinogenicity
a
Compound In processed In mainstream In In humans
tobacco
b
smoke
b
laboratory
(per gram) (per cigarette) animals
PAHs
c
Benz(a)anthracene 20-70 ng Sufficient
Benzo(b)fluoranthene 4-22 ng Sufficient
Benzo(j)fluoranthene 6-21 ng Sufficient
Benzo(k)fluoranthene 6-12 ng Sufficient
Benzo(a)pyrene 0.1-90 ng 20-40 ng Sufficient Probable
Dibenz(a,h)anthracene 4 ng Sufficient
Dibenzo(a,I)pyrene 1.7-3.2 ng Sufficient
Dibenzo(a,l)pyrene present Sufficient
Indeno(1,2,3-cd)pyrene 4-20 ng Sufficient
5-Methylchrysene 0.6 ng Sufficient
Aza-arenes
Quinoline 1-2 µg Sufficient
Dibenz(a,h)acridine 0.1 ng Sufficient
Dibenz(a,j)acridine 3-10 ng Sufficient
7-H-Dibenzo(c,g)-carbazole 0.7 ng Sufficient
N-Nitrosamines
N-Nitrosodimethylamine ND-215 ng 0.1-180 ng Sufficient
N-Nitrosoethylmethylamine 3-13 ng Sufficient
N-Nitrosodiethylamine ND-2.8 ng Sufficient
N-Nitrosopyrrolidine 5-50 ng 3-60 ng Sufficient
N-Nitrosodiethanolamine 50-3000 ng ND-68 ng Sufficient
N-Nitrososarcosine 20-120 ng Sufficient
N-Nitrosonornicotine 0.3-89 µg 0.12-3.7 µg Sufficient
4-(Methylnitrosamino)-3- 0.2-7 µg 0.08-0.77 µg Sufficient
(pyridyl)-1-butanone
N’-Nitrosoanabasine 0.01-1.9 µg 0.14-4.6 µg Limited
N-Nitrosomorpholine ND-690 ng Sufficient
Aromatic amines
2-Toluidine 30-200 ng Sufficient Inadequate
2-Napththylamine 1-22 ng Sufficient Sufficient
4-Aminobiphenyl 2-5 ng Sufficient Sufficient
N-Heterocyclic amines
AaC 25-260 ng Sufficient
MeAaC 2-37 ng Sufficient
IQ 0.26 ng Sufficient Probable
Trp-P-1 0.29-0.48 ng Sufficient
Trp-P-2 0.82-1.1 ng Sufficient
Glu-P-1 0.37-0.89 ng Sufficient
Glu-P-2 0.25-0.88 ng Sufficient
PhlP 11-23 ng Sufficient Possible
Aldehydes
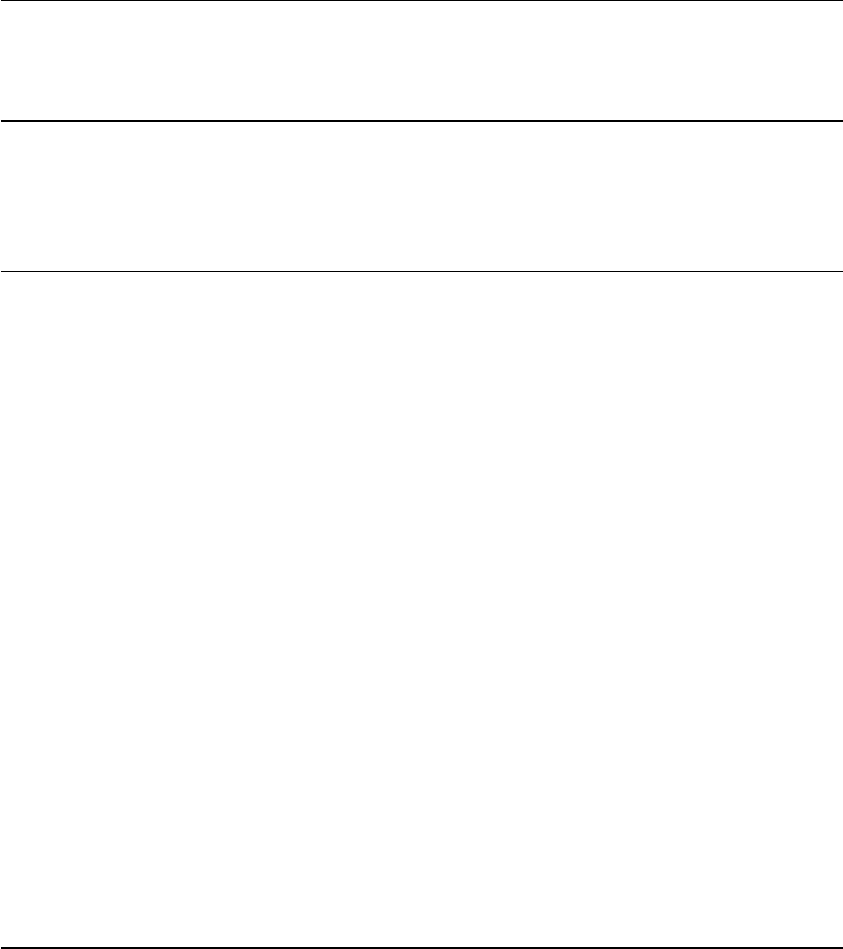
91
Smoking and Tobacco Control Monograph No. 9
Table 15
(continued)
IARC evaluation
evidence of
carcinogenicity
a
Compound In processed In mainstream In In humans
tobacco
b
smoke
b
laboratory
(per gram) (per cigarette) animals
Formaldehyde 1.64-7.4 µg 70-100 µg
d
Sufficient Limited
Acetaldehyde 1.4-7.4 µg 18-1400 µg
d
Sufficient Inadequate
Miscellaneous organic compounds
1,3-Butadiene 20-75 µg Sufficient Probable
Isoprene 450-1000 µg Sufficient Possible
Benzene 12-70 µg Sufficient Sufficient
Styrene 10 µg Limited Possible
Vinyl chloride 1-16 µg Sufficient Sufficient
DDT
e
20-13,400 ng 800-1200 ng Sufficient Possible
DDE
e
7-960 ng 200-370 ng Sufficient
Acrylonitrile 3.2-15 µg Sufficient Limited
Acrylamide Present Sufficient Probable
1,1-Dimethylhydrazine 60-147 µg Sufficient
2-Nitropropane 0.73-1.21 µg Sufficient
Nitrobenzene 25.3 ng Sufficient Possible
Ethyl carbamate 310-375 ng 20-38 ng Sufficient
Ethylene oxide 7 µg Sufficient Sufficient
Di(2-ethylhexyl)phthalate Present 20 µg Sufficient
Furan 18-30 µg Sufficient Inadequate
Benzo(b)furan Present Sufficient Inadequate
Inorganic compounds
Hydrazine 14-51 ng 24-43 ng Sufficient Inadequate
Arsenic 500-900 ng 40-120 ng Inadequate Sufficient
Beryllium 15-75 mg 0.5 mg Sufficient Sufficient
Cobalt 90-1,400 mg 0.13-0.2 mg Sufficient Inadequate
Nickel 2000-6000 ng 0-600 ng Sufficient Limited
Chromium 1000-2000 ng 4-70 ng Sufficient Sufficient
Cadmium 1300-1600 ng 41-62 ng Sufficient Sufficient
Lead 8-10 µg 35-85 ng Sufficient Inadequate
Polonium-210 0.2-1.2 pCi 0.03-1.0 pCi Sufficient Sufficient
a
No designation indicates that IARC has not evaluated the compound.
b
ND, not detected.
c
PAH, polynuclear aromatic hydrocarbons: AaC, 2-amino-9H-pyrido[2,3-b]indole; MeAaC, 2-amino-3-methyl-9H-pyrido[2,3-
b]indole; IQ, 2-amino-3-methylimidazo[4,5-b]quinoline; Trp-P-1, 3-amino-1,4-dimethyl-5H-pyrido[4,3-b]indole; Trp-2, 3-
amino-1-methyl-5H-pyrido[4,3-b]indole; Glu-P-1, 2-amino-6-methyl[1,2-a:3’,2”-d]imidazole; Glu-P-2, 2-aminodipyrido[1,2-
a:3’,2’-d]imidazole; PhlP, 2-amino-1-methyl-6-phenylimidazo[4,5-b]pyridine.
d
The 4
th
report of the Independent Scientific Committee on Smoking and Health (1988) published values for the 14 leading
British cigarettes in 1986 (51.4% of the market) of 20-1050 µg/cigarette (mean 910 µg) for acetaldehyde.
e
During the last decade, DDT and DDE levels have been drastically reduced in U.S. cigarette tobacco ((60 ng and (13 ng).
Source: Hoffmann and Hoffmann, 1997

Chapter 3
92
Table 16
Known carcinogens (ng/cigarette) in the smoke of bright or blond and burley and black tobacco
Carcinogens Bright or blended tobacco Burley or black tobacco
I. Volatile nitrosamines
NDMA NF 6.8-13.8 29
F 1.8-5.7 4.3
NEMA NF (0.1-1.8 2.7
F 0.4-1.0 0.5
NPYR NF 11.0-30.3 25
F 3.1-8.7 10.5
NDMA NF 9.4-48.4 38.8-76.4
NEMA NF (0.1-7.1 2.1-6.3
NPYR NF 6.9-41.2 22.7-36.1
II. NDELA NF (Exp. Cigarettes) 30-51 290
III. TSNA
NNN NF (Exp. Cigarettes) 620 3700
NNK NF (Exp. Cigarettes) 420 320
NAT
b
NF (Exp. Cigarettes) 410 4600
NNN NF 85-255 512-625
NNK NF 70-156 108-432
NAT
b
NF 81-225 266-353
NNN NF 29 203
NNK NF 40-136
NAT
b
NF 45 108
NNN NF 79-885 550-800
NNK NF 62-185 84-470
NAT
b
NF 75-380 225-520
NNN F 213 117-389
NNK F 32 13-55
NAT
b
F 92 74-196
IV. Aromatic amines
2-Toluidine NF 32.2 162
F 41.0 66.8
2-Naphthylamine NF 1.0 1.7
F 2.1 1.8
4-Aminobiphenyl NF 2.4 4.6
F 0.3-0.2 23
V. 2-Nitropropane NF 220-1190 1430-2180

93
Smoking and Tobacco Control Monograph No. 9
Table 16
(continued)
Carcinogens Bright or blended tobacco Burley or black tobacco
VI. PAH
BaA NF (Exp. Cigarettes) 21.0-25.9 10.7-16.7
BaP NF (Exp. Cigarettes) 38-53 24
NF (Exp. Cigarettes) 7.5-9.6 25
NF (Exp. Cigarettes) 35.4 19.7
VII. Volatile Aldehydes
Formaldehyde NF (Exp. Cigarettes) 26,800-36,300 16,100-25,100
Acetaldehyde NF (Exp. Cigarettes) 797,000-906,000 726,000-966,000
IX. Benzene 27,000 12,000
X. Quinoline F 620 1200
Note.
Abbreviations: NDMA, nitrosodimethylamine; NEMA, nitrosoethylamine; NPYR, nitrosopyrrolidine; NDELA,
nitrosodiethanolamine; TSNA, tobacco-specific
N
-nitrosamines; NNN,
N’
-nitrosonornicotine; NNK, 4-
(methylnitrosamino)-1-(3-pyridyl)-1-butanone; NAT,
N’
-nitrosoanatabine; BaA, benz[a]anthracene; BaP,
benzo[a]pyrene; NF, nonfilter; F, filter. The pH of the smoke of blond type cigarettes varies between 6.15 (1
st
puff) and
5.7 (last puff); the pH of the French black cigarette with filter tip measures from 6.8 to 7.4 and without filter tip from 6.6
to 6.95 cm. With pH above 6, the toxicity of the smoke increases.
a
Black cigarettes = French type black cigarettes made exclusively from Burley tobacco; Blond cigarettes = Virginia type
cigarettes and U.S. Blended cigarettes.
b
NAT contains some N’-nitrosoanabasine (NAB).
Hoffmann and Hoffmann, 1997
made with burley tobacco, this table also indicates those carcinogens that
would be expected to be more prevalent in cigar smoke than in cigarette
smoke (Hoffmann and Hoffmann, 1997).
BIOMARKERS FOR Estimates of the smoker’s exposure to toxic and carcinogenic
THE UPTAKE OF smoke constituents are based on the measurements of certain
TOBACCO SMOKE biomarkers. In general, these are determined in saliva, blood,
urine, and/or exhaled air.
Upon inhaling alkaline cigar smoke, nicotine is absobed
Nicotine through the mucous membranes in the
oral cavity as well as across the alveolar surface of the lung. The nicotine
concentration in the blood of a cigar smoker rises gradually (Russell et al.,
1980). In blood with a pH of 7.4, about 31 percent of the nicotine is present
in unprotonated form. Nicotine transfers from the bloodstream across cell
membranes, including those of the central nervous system. In the case
of those secondary cigar smokers and of cigarette smokers who inhale
tobacco smoke, the aerosol reaches the small airways and alveoli of the
lung from which nicotine is quickly absorbed. Within minutes, the blood
concentration of nicotine rises to a maximum (U.S. Department of Health

Chapter 3
94
and Human Services, 1988). Using nicotine-
14
C and measuring the
radioisotope in exhaled air, Armitage et al., (1975) found that cigarette
smokers absorb 82 - 92 percent of the inhaled nicotine; those who do not
inhale the smoke absorbed about 29 percent of inhaled nicotine.
After smoking one piece of the respective product, the nicotine level in
the plasma of cigarette smokers rose from 25 to between 35 and 40 ng/ml;
that of secondary cigar smokers rose from 12.8 to 45.6 ng; and that of
primary cigar smokers changed from 3.4 to 5.2 ng/ml as average
measurements in five smokers per group (Turner et al., 1977). These data
show clearly that the primary cigar smokers takes up far less nicotine because
he does not inhale the smoke deep into the lungs as in the case with cigarette
smokers and secondary cigar smokers.
Carbon Monoxide The determination of carboxyhemoglobin (COHb) is regarded as
the most reliable assay for the uptake of carbon monoxide by smokers. In
nonsmokers who have no significant exposure to CO in their occupational
or home environment, the COHb level is below 1.7 percent; even levels as
low as 0.2 percent COHb have been reported in nonsmokers. Turner et al.
(1977) reported the mean concentration of COHb in 1,933 cigarette smokers
to be 4.78 percent, with 94.7 percent of the measurements indicating COHb
to be ( 1.7 percent. The mean COHb concentration for 39 primary cigar
smokers was 1.36 percent and none showed COHb levels above 1.7 percent.
One hundred and fifty-four secondary cigar smokers had a mean COHb
concentration of 6.8 percent; 97.4 percent of these had concentrations above
1.7 percent. These data were confirmed by several additional reports, all of
which clearly show that the primary cigar smoker tends to inhale not at all or
only very shallowly, while the secondary cigar smoker inhales the smoke at
least as deeply as the cigarette smoker does.
The determination of CO in exhaled breath is not as reproducible as the
COHb determination that measures uptake of CO. However, the method can
be readily executed in an office or at any site by just asking the subject to
exhale into a CO meter. Ockene et al. (1987) conducted a large-scale study
and measured 1.8 - 2.1 CO in the exhaled breath of primary cigar smokers
and 3.3 - 11.0 in the breath of secondary cigar smokers. Similar findings
were reported by others (Cowie et al., 1973; Goldman, 1976, Wald et al.,
1981).
Hydrogen Cyanide The smoke of 1 g tobacco from a cigar contains 1,000 µg of
hydrogen cyanide (HCN), and that from a little cigar contains up to 780 µg.
The smoke of 1 g cigarette tobacco contains up to 600 µg of HCN (Table 6).
The release of HCN into the sidestream smoke per gram of tobacco burned in
a little cigar amounts to 114 µg and that in cigarettes reaches 134 - 167 µg
(Table 9). Although HCN is liberated from certain food items (cyanogens;
e.g. cabbage, broccoli, conifers, vegetables, and certain nuts), the quantities
produced in this manner are significantly lower than the amounts of HCN
inhaled as a tobacco smoke constituent (Galanti, 1997). Therefore, they
usually do not interfere with the assay of thiocyanate, the most important
metabolite of HCN, in physiological fluids of smokers. Thiocyanate

95
Smoking and Tobacco Control Monograph No. 9
concentration is determined by a colorimetric method in an autoanalyzer
(Butts et al., 1974). In one study, the mean concentration of thiocyanate in
the saliva of 30 nonsmokers on a cyanogen-containing diet was 101 ± 51 µg/
ml; in 15 nonsmokers on a diet free of cyanogens, thiocyanate levels were 92
± 90µg/ml, and in the saliva of 20 smokers it was 413 ± 172 µg/ml (p < 0.01
vs. both nonsmokers’ groups) (Galanti, 1977).
Pechacek et al. (1985) reported serum thiocyanate levels in never
smokers at 2.52 ± 1.60 µg/ml, in primary cigar and pipe smokers at 4.22 ±
2.56 µg/ml, in secondary cigar and pipe smokers at 5.63 ± 3.55 µg/ml, and
in cigarette smokers at 8.34 ± 3.03 µg/ml.
Benzene Benzene, a leukomogenic agent, is a ubiquitous contaminant of the
respiratory environment. The American Conference of Governmental
Industrial Hygienists has set the upper permissible limit of a time-weighted
concentration of benzene for an 8-hour work day and a 40-hour work week
(TWA) at 10 ppm (32 µg/L) (American Conference of Governmental
Industrial Hygienists, 1996). Benzene in the smoke of 1 g tobacco burned
as a cigar, amounts to between 90 and 250 µg per gram tobacco (est. 80-
200 µg/L); from 1 g tobacco smoked as a cigarette, one obtains between
8 and 60 µg benzene (est. 25-180 µg/L).
Polynuclear Tobacco smoke contains at least ten carcinogenic PAH (Hoffmann
Aromatic and Hoffmann, 1997). Benzo(a)pyrene (BaP) concentration in
Hydrocarbons environmental samples and food items serves as a surrogate measure
(PAH) of PAH-related carcinogenic potential. Per gram tobacco BaP yields
in the mainstream smoke (MS) of cigars range from 30 to 51 ng; in MS of
little cigars, 26 ng; and in MS of a cigarette without a filter tip, 26 - 59 ng
(Table 7). Up to 90 percent of the PAH in cigarette smoke is retained upon
inhalation in the respiratory tract of a long-term smoker; however, only a
small percentage of the PAH is absorbed from food as found in the digestive
tract (Bresnick et al., 1983; Grimmer, 1983; Rahman et al., 1986).
Carcinogenic PAH are primarily contact carcinogens. They are
metabolically activated by P450 isozymes to their ultimate carcinogenic
forms, the dihydrodihydroxy epoxides (Dipple et al., 1984). They form
intracellular adducts with macromolecules, including DNA (Dipple et al.,
1984). The prevailing DNA adduct formed through BaP metabolism is
(+)trans-anti-7,8-dihydro-9-hydroxy-10-N
2
-guanosine (Geacintov et al.,
1997).
Among biomakers of uptake and metabolic activation of smoke
constituents in cigarette smokers, hemoglobin adducts of 4-aminobiphenyl,
BaP, and other PAH have been measured, and urinary metabolites and/or
detoxification products of NNK and/or benzene have been quantified. As an
indicator of endogenous N-nitrosation, leading to N-nitrosamine formation,
N-nitrosoproline has been determined in the urine of cigarette smokers.
Similar biomarker studies for cigar smokers are lacking.

Chapter 3
96
SUMMARY AND Today, several types of cigars are marketed in the United States:
RESEARCH NEEDS little cigars, (each weighing less than 1.36 g), regular cigars, small
cigars, cigarillos, and premium cigars.
Primary cigar smokers tend not to inhale the cigar smoke, whereas
primary cigarette smokers do tend to inhale the cigarette smoke. The
principal reason for this difference is the pH of cigar smoke which is initially
6.2 for early puffs and rises to 8.0 for later puffs. At alkaline pH conditions,
part of the nicotine is present in unprotonated form in the vapor phase.
Unprotonated, volatile nicotine is absorbed through the mucous membrane
of the oral cavity and is quickly transported via the bloodstream to the
various sites, including the central nervous system, where it exerts the
pharmacological effects that seem to “satisfy” the smoker. The elevated pH
of the smoke of cigars is caused by the relatively high nitrate content of the
air-cured and fermented cigar tobacco (1.4 - 2.1 percent) compared to the
nitrate content of the U.S. blended cigarette tobacco (0.5 - 1.7 percent).
In the burning cigar, part of the nitrate is reduced to ammonia and
part of it yields NO
x
. Nitrogen dioxide in the smoke contributes to the
N-nitrosation of secondary and tertiary amines. The most abundant amines
in tobacco smoke, nicotine and the minor Nicotiana alkaloids, are thereby
nitrosated and become TSNA. Some TSNA are formed by pyrosynthesis and
some TSNA transfer from the tobacco into the smoke. TSNA are present in
significantly higher amounts in cigar smoke than in cigarette smoke.
Tobacco smoke contains more than 4,000 individual compounds with
about 500 of these in the gas phase. One gram of tobacco burned in a cigar
delivers between 39 and 65 mg carbon monoxide and 160 - 300 µg nitrogen
oxides compared to maxima of 19 mg carbon monoxide and up to 160 µg of
nitrogen oxides for the same amount of tobacco burned in a cigarette. These
high concentrations of CO and NO
x
in cigar smoke are due to the very low
porosity of the cigar binder and wrapper which contrasts with the high
porosity of cigarette paper.
Many toxic agents and 62 known carcinogens have been identified
among the 4000 compounds in cigarette smoke. Fewer of these have been
identified in cigar smoke. However, it is highly likely that most of the toxic
and carcinogenic constituents found in cigarette smoke are also present
in cigar smoke, albeit at different concentrations. Disregarding studies on
the effects of additives to cigar tobacco, there is only a limited need to
specifically identify toxic and carcinogenic compounds in cigar smoke.
There exists a need to investigate two particular areas with regard to
health effects of cigar smoking. One is the study of the smoking patterns
of primary and secondary cigar smokers and of the uptake of toxic and
carcinogenic smoke constituents by both types of cigar smokers, as well as
the study of metabolism of critical constituents by the cigar smoker. It is
especially important to verify the possibility of endogenous formation of
carcinogenic N-nitrosamines in cigar smokers. Except for a few isolated
investigations on nicotine uptake by cigar smokers, these aspects remain
unexplored.

97
Smoking and Tobacco Control Monograph No. 9
The second area of needed investigation relates to the reduction of toxic
and carcinogenic agents in cigar smoke, including nicotine. Can the porosity
of the cigar wrapper be changed? Is it possible, by addressing this aspect and
others, to reduce the high yields of carbon monoxide and “tar” in cigar
smoke? Are there ways to reduce the high nitrate content of cigar tobacco?
In view of the increasing consumption of cigars in the United States, our
knowledge regarding the uptake and metabolic fate of the toxic and
carcinogenic agents in cigar smoke, and means for their reduction in
the smoke should be intensified. Such efforts need to parallel public health
measures toward informing the consumers about the ill effects of cigar
smoke on human health.
CONCLUSIONS
1. Cigar smoke contains the same toxic and carcinogenic compounds
identified in cigarette smoke.
2. When examined in animal studies, cigar smoke tar appears to be at least
as carcinogenic as cigarette smoke tar.
3. The differences in risk between cigarette smoking and cigar smoking
appear to be related to the differences in patterns of use of those two
tobacco products, principally non-daily use and less inhalation among
cigar smokers, rather than a difference in the composition of the smoke.
4. The amount of nicotine available as free, unprotonated nicotine is
generally higher in cigars than in cigarettes due to the higher pH of cigar
smoke. This free nicotine is readily absorbed across the oral mucosa, and
may explain why cigar smokers are less likely to inhale than cigarette
smokers.
.
REFERENCES
Adams, J.D., Lee, S.J., Vinchkoski, N., Castonguay, A.,
Hoffmann, D. On the formation of the tobacco-
specific carcinogen 4-(methylnitrosamino)-1-(3-
pyridyl)-1-butanone during smoking, Carcinogenesis
17:339-346, 1983.
Adams, P.I. Combustion temperatures in cigars and
cigarettes. A comparative study Tobacco Science
12:144-150, 1968.
Adler, R., Peck, R.L., Thompson, L. Chemistry of cigar
butt odor. II. Further investigations on the
distillable portion. Tobacco Science 15:121-123,
1971.
Adlkofer, F.X., Scherer, G., Von Meyernick, L.,Von
Malzan, C.H., Jarcyk, L. Exposure to ETS and its
biological effects: A review. In: Present and Future
Indoor Air Quality C. J. Bieve, Y. Courteous and M.
Govaerts (eds.), Elsevier Science Publishers, pp.
183-196, 1989.
American Conference of Governmental Industry
Hygienists. 1996-1997 Threshold Limit Values for
Chemical Substances and Physical Agents, and
Biological Exposure Indices. American Conference
of Governmental Industry Hygienists, Cincinnati,
Ohio, 1996.
Acknowledgments The authors greatly appreciate the editoral assistance of Mrs.
Patricia Sellazzo. Our studies in tobbacco carcinogenesis are supported by
grants CA-29850, CA-70972, and Cancer Center grant CA-17613 from the
National Cancer Institue.

Chapter 3
98
Ames, B.N., Shigenaga, M.K., Hagen, T.M. Oxidants,
antioxidants, and the degenerative disease of aging.
Proc. Natl. Acad. Sci. USA 90: 7915/7922, 1993.
Andren, A.W., Harriss, R.C. Mercury content of
tobacco. Environmental Letters 1(4):231-234, 1971.
Appel, B.R., Guirguis, G., Kim, I.S., Garbin, O.,
Fracchia, M., Flessel, C.P., Kizer, K.W., Book, S.A.,
Warriner, T.E. Benzene, benzo(a) pyrene, and lead
in smoke of tobacco products other than cigarettes.
American Journal of Public Health 80 (5):560-564,
1990.
Armitage, A.K., Turner, D.M. Absorption of nicotine in
cigarette and cigar smoke through the oral mucosa.
Nature (London) 226:1231-1232, 1970.
Armitage, A.K., Dollery, C.T., George, C.F., Houseman,
T.H., Lewis, P.J., Turner, D.M. Absorption and
metabolism of nicotine from cigarettes. British
Medical Journal 4(5992):313-316, 1975.
Badré, R., Guillerm, R., Abran, N., Bourdin, M.,
Dumas, C. Atmospheric pollution by smoking.
Annales Pharmaceutiques Francaises 36 (9-10):443-
452, 1978.
Baker, R.R., Proctor, C.J. The origin and properties of
environmental tobacco smoke. Environment
International 16:231-245, 1990.
Battista, S.P. Ciliatoxic components in cigarette
smoke. In: Smoking and Health. Volume 1. The Risk
for the Smoker. Proceedings of the Third World
Conference on Smoking and Health DHEW
Publication No. (NIH) 76-1221: 517-534,
Washington, D.C., 1976.
Benowitz, N.L., Jacob, P.,III., Fong, I., Gupta, S.
Nicotine metabolic profile in man and comparison
of cigarette smoking and transdermal nicotine.
Journal of Pharmacology and Experimental Therapeutics
268 (1):296-303, 1994.
Bernfeld, P., Nixon, C.W., Homburger, F. Studies on
the effect of irritant vapors on ciliary mucus
transport. I. Phenol and cigarette smoke. Toxicology
and Applied Pharmacology 6:103-111, 1964.
Bilimoria, M.H., Nisbet, M.A. Differentiation of
tobacco smoke condensates on the basis of reducing
properties. Beiträge zur Tabakforschung 6:27-31,
1972.
Borowski, H., Seehofer, F. Temperaturverlauf des
Hauptstromrauches im Cigaretten stummel
während des Rauchens. Beiträge zur Tabakforschung
1:329-333, 1962.
Boyd, D.F., Briggs, C.D., Darby, P.W. Dependence of
the gas phase composition of smoke on the
combustion temperature of tobacco products.
Tobacco Science 16:160-165, 1972.
Bradford, J.A., Harlan, W. R., Hanmer, H.R. Nature of
cigarette smoke. Technic of experimental smoking.
Industrial and Engineering Chemistry 28:836-839,
1936.
Bresnick, E., Anderson, M.W., Gorse, F.A., Jr.,
Grosjean, D., Hites, R.A., Kappas, A., Kouri, R.E.,
Pike, M.C., Selkirk, J.K., White, L.J., Frazier, J.A.,
Grossblatt, N., Perrin, J.E. Polycyclic Aromatic
Hydrocarbons: Evaluation of Sources and Effects,
Chapters 1, 2, 4, and 6. Washington, D.C:
National Academy Press, 1983.
Brunnemann, K.D., Cox, J.E., Hoffmann, D. Analysis
of tobacco-specific N-nitrosamines in indoor air.
Carcinogenesis 13:2415-2418, 1992.
Brunnemann, K.D., Hoffmann, D. The pH of tobacco
smoke. Food Cosmetics and Toxicology 12:115-124,
1974(a).
Brunnemann, K.D., Hoffmann, D. Analytical studies
on N-nitrosamines in tobacco and tobacco smoke.
Recent Advances in Tobacco Science 17:71-112,
1991(b).
Brunnemann, K.D., Hoffmann, D. Assessment of the
carcinogenic N-nitrosodiethanolamine in tobacco
products and tobacco smoke. Carcinogenesis 2:1123-
1127, 1981.
Brunnemann, K.D., Hoffmann, D. Chemical studies
on tobacco smoke. XXIV. A quantitative method
for carbon monoxide and carbon dioxide in
cigarette and cigar smoke. Journal of
Chromatographic Science 12 (2):70-75, 1974 (b).
Brunnemann, K.D., Hoffmann, D. Chemical studies
on tobacco smoke XXXIV. Gas chromatographic
determination of ammonia in cigarette and cigar
smoke. Journal of Chromatographic Science 13: 1237-
1244, 1975.
Brunnemann, K.D., Hoffmann, D. Decreased
concentrations of N-nitrosodiethanolamine and -
N-nitrosomorpholine in commercial tobacco
products. Journal of Agricultural and Food Chemistry
39:207-208, 1991 (a).
Brunnemann, K.D., Hoffmann, D., Wyder, E.L., Gori,
G.B. Determination of tar, nicotine and carbon
monoxide in cigarette smoke. A comparison of
international smoking conditions. Proc. 3rd World
Conference on "Smoking and Health", Volume 1.
Modifying the Risk for the Smoker. DHEW Publ. No.
(NIH) 76-1221, pp. 441-449; 1976a.
Brunnemann, K.D., Kagan, M.R., Cox, J.E., Hoffmann,
D. Analysis of 1,3-butadiene and other selected gas
phase components in cigarette mainstream and
sidestream smoke by gas chromatography-mass
selected detection. Carcinogenesis 11:1863-1868,
1990.
Brunnemann, K.D., Lee, H.C., Hoffmann, D.
Chemical studies on tobacco smoke. XLVII. On
quantitative analysis of catechols and their
reduction. Analytical Letters 9:939-955, 1976.
Brunnemann, K.D., Scott, J.C., Hoffmann, D. N-
nitrosoproline, an indicator for N-nitrosation of
amines in processed tobacco. Journal of Agricultural
and Food Chemistry 31:905-909, 1983.

99
Smoking and Tobacco Control Monograph No. 9
Brunnemann, K. D., Stahnke, G., Hoffmann, D.
Chemical studies on tobacco smoke. LXI. Volatile
Pyridines: Quantitative analysis in mainstream and
sidestream smoke of cigarettes and cigars. Analytical
Letters A 11:545-560, 1978.
Brunnemann, K.D., Yu, L., Hoffmann, D. Assessment
of carcinogenic volatile N-nitrosamines in tobacco
and in mainstream and sidestream smoke from
cigarettes. Cancer Research 37: 3218-3222, 1977b.
Brunnemann, K.D., Yu, L., Hoffmann, D. Chemical
Studies on tobacco smoke. XLIX. Gas
chromatographic determination of hydrogen
cyanide and cyanogen in tobacco smoke. Journal of
Analytical Toxicology 1:38-42, 1977a.
Burton, H.R., Dye, N.K., Bush, L. Distribution of
tobacco constituents in tobacco leaf tissue. 1.
Tobacco-specific nitrosamines, nitrate, nitrite and
alkaloids. Journal of Agricultural and Food Chemistry
40 (6):1050-1055, 1992.
Butts, W.C., Kuehneman, J., Widdowson, G.M.
Automated method for determining serum
thiocyanate to distinguish smokers from
nonsmokers. Clinical Chemistry 20(10) 1344-1348,
1974.
Byrd, G.D., Chang, K.M., Greene, J.M., deBethizy, J.D,
Reynolds, J.H. Evidence for urinary excretion of
glucuronide conjugates of nicotine, cotinine, and
trans-3'-hydroxycotinine in smokers. Drug
Metabolism and Disposition 20 (2):192-197, 1992.
Campbell, J.M., Lindsey, A.J. Polycyclic hydrocarbons
in cigar smoke. British Journal of Cancer 11: 192-195,
1957.
Carter, W.L., Hasagawa, I. Fixation of tobacco smoke
aerosols for size distribution studies. Journal of
Colloid Interface Science 63:134-141, 1975.
Castleden, C.M., Cole, P.V. Inhalation of tobacco
smoke by pipe and cigar smokers. Lancet II
(819):21-22, 1973.
Castonguay, A., Stoner, G.D., Schut, H.A.J., Hecht,
S.S. Metabolism of tobacco-specific N-nitrosamines
by cultured human tissues. Proceedings of the
National Academy of Sciences 80: 6694-6697, 1983.
Chakraborty, M.K., Ghelani, L.M., Patel, B.K.
Agricultural and technological experiments to
reduce toxic chemicals in bidi smoke. In: Tobacco
and Health: The Indian Scene. L. D. Sanghvi and P.
Natami, eds. Tata Memorial Centre, Bombay, India,
1989, pp. 89-100.
Cigar Aficionado. Coronas and Lonsdales, Fall 1996.
1991.
Cornell, A., Cartwright, W.F., Bertinuson, T.A.
Influence of microorganisms (fermentation) on the
chemistry of tobacco. Recent Advances in Tobacco
Science 5:27-61, 1979.
Cowie, J., Sillett, R.W., Boll. K.P. Carbon monoxide
absorption by cigarette smokers who change to
smoking cigars. Lancet I: 1033-1035, 1973.
Creek, L. Capehart, T., Grise, V. U.S. Tobacco Statistics
1935-1992, U.S. Department of Agriculture.
Statistical Bulletin 869:14, 1994.
Croninger, A.B., Graham, E.A., Wynder, E.L.
Experimental production of carcinoma with
tobacco products. V. Carcinoma induction in mice
with cigar, pipe and all-tobacco cigarette tar. Cancer
Research 18:1263-1271, 1958.
Dalhamn, T., Rylander, R. Cigarette smoke and
ciliastasis. Effect of varying composition of smoke.
Archives of Environmental Health 13:47-50, 1966.
Davies, R.F., Day. T.D. A study of the comparative
carcinogenicity of cigarette and cigar smoke
condensate on mouse skin. British Journal of Cancer
23:363-368, 1969.
Dipple, A., Moschel, R.C., Bigger, A.H. Polynuclear
aromatic hydrocarbons. In: Chemical Carcinogenesis,
Second Edition, C.E. Searle (ed.). Washington,
D.C., American Chemical Society Monograph 182:41-
163, 1984.
Djordjevic, M.V., Brunnemann, K.D., Hoffmann, D.
Identification and analysis of a nicotine- derived N-
nitrosamino acid and other nitroamino acids in
tobacco. Carcinogenesis 10:725-731, 1989.
Djordjevic, M.V., Fan, J., Ferguson, S, Hoffmann, D.
Self-regulation of smoking intensity, smoke yields
of low-nicotine, low-”tar” cigarettes. Carcinogenesis
16:2015-2021, 1995(a).
Djordjevic, M.V., Fan, J., Hoffmann, D. Assessment of
chlorinated pesticide residues in cigarette tobacco
based on supercritical fluid extraction and GC-
ECD. Carcinogenesis 16:2627-2632, 1995b.
Djordjevic, M.V., Hoffmann, D. Analysis of the
mainstream smoke of cigarettes, little cigars, cigars,
and premium cigars. 1998 unpublished data.
Dong, M., Schmeltz, I., Jacobs, E., Hoffmann, D.
Chemical studies on tobacco smoke. LV. Aza-arenes
in cigarette smoke. Journal of Analytical Toxicology
2:21-25, 1978.
Doull, J., Frawley, J.P., George, W. List of ingredients
added to tobacco in the manufacture of cigarettes
by six major American cigarette companies.
Washington D.C: Covington and Burling, April 12,
1994.
Eudy, L.W., Thome, F.W., Heavner, D.K., Green, C.R.,
Ingebrethsen, B.J. Studies on the vapor-particulate
phase distribution of environmental nicotine by
selective trapping and detection methods.
Proceedings of the 70th Annual Meeting of the Air
Pollution Control Association, Minneapolis, MN:
paper 38.7, 1986.
Fagerström, K.O. Effects of a nicotine-enriched
cigarette on nicotine titration, daily cigarette
consumption and levels of carbon monoxide,
cotinine and nicotine. Psychopharmacology 77
(2):164-167, 1982.

Chapter 3
100
Frankenburg, W.G., Gottscho, A.M. Nitrogen
compounds in fermented cigar leaves. Industrial and
Engineering Chemistry 44:301-305, 1952.
Frankenburg, W.G., Gottscho, A.M., Vaitekinnos, A.A.
Biochemical conversion of some tobacco alkaloids.
Tobacco Science 2:9-13, 1958.
Franzke, Ch., Ruick, G., Schmidt, M. Untersuchungen
zum Schwermetallgehalt von Tabakwaren und
Tabakrauch. Nahrung 21(5):417-428, 1977.
Galanti, L.M. Specificity of salivary thiocyanate as a
marker of cigarette smoking is not effected by
alimentary sources. Clinical Chemistry 43:184-185,
1997.
Geacintov, N.E., Cosman, M., Hingerty, B.E., Amin,
S., Broyde, S., Patel, D.J. NMR solution structures of
stereoisomeric covalent polycyclic aromatic
carcinogen - DNA adducts: Principles, patterns and
diversity. Chemical Research in Toxicology 10:111-
146, 1997.
Goldman, A.L. Cigar smoking. American Review of
Respiratory Diseases 113:87-89, 1976.
Grimmer, G. (ed.) Environmental Carcinogenesis:
Polycyclic aromatic hydrocarbons. Chemistry,
Occurrence, Biochemistry, Carcinogenicity. C.R.C.
Press, Inc., Boca Raton, Florida, 1983.
Guerin, M.R. Formation and general characteristics of
environmental tobacco smoke. Air Pollution Control
Association Speciality Conference on Combustion
Process and the Quality of Indoor Environments,
Niagara Falls, NY, 1988.
Guerin, M.R., Jenkins, R.A., Tomkins, B.A. The
Chemical Nature of Environmental Tobacco
Smoke: Composition and Measurement. Chelsea,
MI: Lewis Publishers, Inc., 1992.
Gundel, L.A., Daisey, J.M., Offermann, F.J.
Development of an indoor sampling and analysis
method for particulate polycyclic aromatic
hydrocarbons. Proceedings of the 5th International
Conference on Indoor Air Quality and Climate.
Toronto, Canada. Volume 2:299-304, 1990.
Haley, N.J., Sepkovic, D.W., Hoffmann, D., Wynder,
E.L. Cigarette smoking as a risk factor for
cardiovascular diseases. Part VI. Compensation
with nicotine availability as a single variable.
Clinical Pharmacology and Therapeutics 38:164-170,
1985.
Halter, H.M., Ito, T.I. Effect of tobacco reconstitution
and expansion process on smoke composition.
Recent Advances in Tobacco Science 4:113-137, 1980.
Hamill, W., O’Neill, R.P. Carbon monoxide
intoxication in cigar smokers. Irish Journal of
Medical Science 8 (6):273-277, 1969.
Harke, H.P. The problem of passive smoking. I. The
influence of smoking on the CO concentration of
office rooms. Internationales Archiv für
Arbeitsmedizin 33:199-206, 1974.
Hecht, S.S. Recent studies on mechanisms of
bioactivation and detoxification of 4-(methyl-
nitrosamino)-1-(3-pyridyl)-1-butanone (NNK), a
tobacco-specific lung carcinogen. Critical Reviews in
Toxicology 26:163-181, 1996.
Hecht, S.S., Hoffmann, D. The relevance of tobacco-
specific N-nitrosamines to human cancer. Cancer
Surveys 8:273-294, 1989.
Herning, R.I., Jones, R.T., Bachman, J., Mines, A.H.
Puff volume increases when low-nicotine cigarettes
are smoked. British Medical Journal Clinical Research
Edition 287:187-189, 1981.
Higgins, C.E., Thompson, C.V., Ilgner, R.H., Jenkins,
R.A., Guerin, M.R. Determination by vapor phase
hydrocarbons and nitrogen constituents in
environmental tobacco smoke. Analytical Chemistry
Division, Oak Ridge National Laboratory, Oak
Ridge, TN 37831; 6120, 1991.
Hiller, F.C., McCusker, K.T., Mazumder, M.K.,Wilson,
J.D., Bone, R.C. Deposition of sidestream cigarette
smoke in the human respiratory tract. American
Review of Respiratory Diseases 125:406-408, 1982.
Hoffmann, D., Adams, J.D., Brunnemann K.D., Hecht,
S.S. Assessment of tobacco specific N-nitrosamines
in tobacco products. Cancer Research 39:2505-2509,
1979 (a).
Hoffmann, D., Brunnemann, K.D. Endogenous
formation of N-nitrosoproline in cigarette smokers.
Cancer Research 43:5570-5574, 1983.
Hoffmann, D., Brunnemann, K.D., Prokopczyk, B.,
Djordjevic, M.V. Tobacco-specific N-nitrosamines
and areca-derived N-nitrosamines: chemistry,
biochemistry, carcinogenicity and relevance to
humans. Journal of Toxicology and Environmental
Health 41:1-5, 1994.
Hoffmann, D., Djordjevic, M.V., Hoffmann, I. The
changing cigarette. Preventive Medicine, 26: 427-434,
1997.
Hoffmann, D., Dong, M., Hecht, S.S. Origin in
tobacco smoke of N’-nitrosonornicotine, a tobacco-
specific carcinogen. Brief Communication. Journal
of the National Cancer Institute 58: 1841-1844, 1977
Hoffmann, D., Hoffmann, I. Chemical studies on
tobacco smoke. The changing cigarette, 1950-1995.
Journal of Toxicology and Environmental Health
50:307-364, 1997.
Hoffmann, D., Patrianakos, C.P., Brunnemann K.D.,
Gori, G.B. Chemical studies on tobacco smoke
XXXVI. Chromatographic determination of vinyl
chloride in tobacco smoke. Analytical Chemistry
48:47-50, 1976.
Hoffmann, D., Rathkamp, G., Brunnemann, K.D.,
Wynder, E.L. Chemical studies on tobacco smoke
XXII. On the profile analysis of tobacco smoke.
Science of the Total Environment 2:151-171, 1973.

101
Smoking and Tobacco Control Monograph No. 9
Hoffmann, D., Rathkamp, G., Wynder, E.L.
Comparison of the yields of several selected
components in the smoke from different tobacco
products. Journal of the National Cancer Institute
31:627-637, 1963.
Hoffmann, D., Rivenson, A., Hecht, S.S., Hilfrich, J.,
Kobayashi, N. Wynder, E.L. Model studies in
tobacco carcinogenesis with the Syrian golden
hamster. [Review]. Progress in Experimental Tumor
Research 24:370-390, 1979(b).
Hoffmann, D., Sanghvi, L.D., Wynder, E.L.
Comparative analysis of Indian bidi and American
cigarette smoke. International Journal of Cancer 14:49-
53, 1974.
Hoffmann, D., Wynder, E.L. Chemical studies on
tobacco smoke XVIII. Smoke of cigarettes and little
cigars. An analytical comparison. Science 178:1197-
1199, 1972.
Homburger, F., Treger, A., Baker, J.R. Mouse skin
painting with smoke condensates from cigarettes
made of pipe, cigar and cigarette tobaccos. Journal of
the National Cancer Institute 31:1445-1459, 1963.
Ingebrethsen, B.J., Sears, S.B. Particle size distribution
measurements of sidestream smoke. Abstract’s 39th
Tobacco Chemists Research Conference, Montreal,
Quebec, 1985.
International Agency for Research on Cancer.
Beryllium and Beryllium compounds. IARC
Monographs on the Evaluation of Carcinogenic Risks to
Humans 58: 41-117, 1993a.
International Agency for Research on Cancer. Tobacco
Smoking. IARC Monographs on the Evaluation of the
Carcinogenic Risk of Chemicals to Humans 38, 1986, p.
421.
International Agency for Research on Cancer. Overall
evaluations of carcinogenic risk to humans: An
updating of IARC Monographs Volumes 1-42, p. 440,
Lyons, France, 1987.
International Agency for Research on Cancer. Nickel
and Nickel Compounds. IARC Monographs on the
Evaluation of Carcinogenic Risks to Humans 49:257-
445, 1990.
International Agency for Research on Cancer. DDT
and associated compounds. IARC Monographs on the
Evaluation of Carcinogenic Risks to Humans. 53:179-
249, 1991.
International Agency for Research on Cancer.
Cadnium and cadnium compounds. IARC
Monographs on the Evaluation of Carcinogenic Risks to
Humans. 58:119-237, 1993b.
International Agency for Research on Cancer.
Ethyleneoxide. ARC Monographs on the Evaluation of
Carcinogenic Risks to Humans. 60:73-159, 1994.
International Agency for Research on Cancer.
Nitrobenzene. IARC Monographs on the Evaluation of
Carcinogenic Risks to Humans. 65:381-408, 1996.
International Committee for Cigar Smoke Study.
Machine smoking of cigars. Bulletin du Information
CORESTA 1:31-34, 1974.
Iskander, F.Y., Bauer, T.L., Klein, D.E. Determination
of 28 elements in American cigarette tobacco by
neutron-activation analysis. Analyst 111:107-109,
1986.
Jeffers, H.P., Gordon, K. The Good Cigar. New York:
Lyons and Burford Publishers, 1996.
Jenkins, R.A., Palansky, A., Counts, R.W., Bayne, C.K.,
Dindall, A.B., Guerin, M.R. Exposure to
environmental tobacco smoke in sixteen cities in
the United States as determined by personal
breathing zone air sampling. Journal of Exposure,
Analytical and Environmental Epidemiology 6:473-
502, 1996.
Kahn, H.A. The Dorn study on smoking and mortality
among U.S. Veterans: Report on eight and one half
years of observation. National Cancer Institute
Monographs 19:1-125, 1966.
Keith, C.H., Derrick, J.C. Measurement of the particle
size distribution and concentration of cigarette
smoke by the conifuge. Tobacco Science 5:84-91,
1961.
Kensler, C.J. The pharmacology of tobacco smoke.
Effects of chronic exposure. In: Tobacco and Health.
G. James and T. Rosenthal (eds.) Springfield, IL:
Charles G. Thomas Publishers, 1962, pp. 5-20.
Kensler, C.J., Battista, S.P. Components in cigarette
smoke with ciliary depressant activity and their
selective removal by filters containing activated
charcoal granules. New England Journal of Medicine
269:1161-1169, 1963.
Kingsborough, E.K. Antiquities of Mexico. Comparing
facsimilies of ancient Mexican paintings. London,
1831-1849.
Kirk, P.W.W., Hunter, M., Back, S.O., Lester, J.N.,
Perry, R. Environmental Tobacco and Indoor Air.
In: Indoor and Ambient Air Quality. R. Perry and
P.W.W. Kirk (eds.), London: Selper Ltd., 1988, pp.
99-112.
Klus, H. Distribution of mainstream and sidestream
smoke components. Recent Advances in Tobacco
Science 16:189-222, 1990.
LaVoie, E.J., Shigematsu, P.L., Adams, J.D., Hoffmann,
D. Comparison of the steam-volatile components
in cigarette, pipe and chewing tobaccos. Journal of
Agricultural and Food Chemistry 33:876-879, 1985.
Lawson, F.R., Corley,C., Schechter, M.S. Insectide
residues on tobacco during 1962. Tobacco Science
8:110-112, 1964.
Lederer, B.P., Hammond, S.K. Evaluation of vapor
phase nicotine and respirable suspended particle
mass as markers for environmental tobacco smoke.
Environmental Science and Technology 25:770-777,
1991.
Löfroth, G., Burton, R.M., Forehand, I., Hammond,
K.S., Seila, R.I., Zweidinger, R.B., Lewtas, J.
Characterization of environmental tobacco smoke.
Environmental Science and Technology 23:610-14,
1989.

Chapter 3
102
Lopt, S., Vistisen, K., Ewertz, M., Tjonneland, A.,
Overvad, K., Poulsen, H.E. Oxidative DNA damage
estimated by 8-hydroxydeoxyguanosine excretion
in humans: influence of smoking, gender, and body
mass. Carcinogenesis 13:2241-2247, 1992.
Martell, E.A. Radioactivity of tobacco trichomes and
insoluble cigarette smoke particles. Nature 249
(5):215-217, 1974.
Miesner, E.A., Rudnick, S.N., Hu, P.-C., Spengler, J.D.,
Preller, I., Özkaynak, H., Nelson, W. Particulate and
nicotine sampling in public facilities and offices.
Journal of the Air Pollution Control Association
39:1577-1582, 1989.
Miller, J.E. Determination of the components of pipe
tobacco smoke by means of a new pipe-smoking
machine. Proceedings of the 3rd World Tobacco
Scientific Congress. Salisbury, Rhodesia, CORESTA.
February 1963, 11.
Morie, G.P. Fractions of protonate and unprotonated
nicotine in tobacco smoke at various pH. Tobacco
Science 16: p. 76, 1972.
Moshy, R.J. Reconstituted tobacco sheet. In: Tobacco
and Tobacco Smoke. Studies in Experimental
Carcinogenesis, E.L. Wynder and D. Hoffmann, (eds.)
New York: Academic Press, 1967, pp. 47-83.
Muramatsu, M., Umemura, S., Okada, T., Tomita, H.
Estimation of exposure to tobacco smoke with a
newly developed nicotine personal monitor.
Environmental Research 35:218-227, 1984.
Muramatsu, M., Umemura, S., Fukui, J., Arai, T., Kira,
S. Estimation of personal exposure to ambient
nicotine in daily environment. International Archives
of Occupational and Environmental Health 59 (6): 545-
550, 1987.
National Research Council. Environmental Tobacco
Smoke. Measuring Exposures and Assessing Health
Effects. National Academy Press: Washington, D.C.,
1986.
Nelson, P.R., Kelly, S.P., Conrad, F.W. Environmental
chamber test method for the quantitative
comparison of environmental tobacco smoke
generated by different cigarettes. Presented at a
Conference on “Eclipse and the Reduction Strategy
for Smoking”. Duke University, Winston-Salem,
North Carolina, August 29, 1996, p. 31.
Nelson, P.R., Kelly, S.P., Conrad, F.W. Generation of
environmental tobacco smoke by cigars. Presented
at the 51
st
Tobacco Chemists’ Research Conference.
Winston-Salem, North Carolina, September 14-17,
1997, p. 15.
Norman, V., Keith, C.H. Charged particles in cigarette
smoke. Tobacco Science 9:75-79, 1975.
O’Hara, C.B. Cohabitation. How the cigar resurgence is
affecting the cigarette industry. Tobacco International
198(4):39-41, 1996.
Ockene, J.K., Pechacek, T.F., Vogt,T., Svendsen, K.
Does switching from cigarettes to pipes or cigars
reduce tobacco smoke exposure? American Journal of
Public Health 77(11):1412-1416, 1987.
Oldaker, G.B., III, Conrad, F.W., Jr. Estimation of the
effect of environmental tobacco smoke on air
quality within passenger cabins of commercial
aircraft. Environmental Science and Technology
21:994-999, 1987.
Osdene, T.S. Reaction mechanisms in the burning
cigarette. In The Recent Chemistry of Natural Products
Including Tobacco. N. J. Fina, ed. Philip Morris
Second Science Symposium; New York, Philip
Morris, 42-59, 1976.
Osman, S., Barson, J. Hydrocarbons in cigar smoke.
Tobacco Science 8:158-160, 1964.
Osman, S., Barson, J., Dooley, C.J. Paraffins of tobacco
smoke. Journal of the Association of Official
Agricultural Chemists 48:1059-1062, 1965.
Osman, S., Schmeltz, I., Higman, H.C., Stedman, R.L.
Volatile phenols in cigar smoke Tobacco Science
7:141-143, 1963.
Pailer, M., Vollmin, J, Karninen, Ch., Kuhn, H. Über
das Vorkommen von primären und sekundären
Aminen im Zigarrenrauch. Fachliche Mitteilungen der
Österreichischen Tabakregie 10:1-4, 1969.
Pechacek, T.F., Folsom, A.R., deGaudermaris, R.,
Jacobs, D.R., Jr., Luepker, R.V., Gillum R.F.,
Blackburn, H. Smoke exposure in pipe and cigar
smokers: Serum thiocyanate measures. Journal of the
American Medical Association 254 (23):3330-3332,
1985.
Peck, R.L., Osman, S.F., Barson, J.L. Cigar butt aroma.
I. Preliminary study of cigar butt headspace vapors.
Tobacco Science 13:38-39, 1969.
Pillsbury, H.C., Bright, C.C., O’Connor, J., Irish, F.W.
Tar and nicotine in cigarette smoke. Journal of the
Association of Official Analytic Chemists 52:458-462,
1969.
Posselt, W., Reimann, L. Chemische Untersuchungen
des Tabaks und Darstellung des eigenthümlichen
wirksamen Princips dieser Pflanze. Geigers Magazin
der Pharmazie 24:138-161, 1828.
Rahman, A., Barrowman, J.A. and Rahimtula, A. The
influence of bile on bioavailability of polycyclic
aromatic hydrocarbons from rat intestine. Canadian
Journal of Physiology and Pharmacology 64:1214-
1218, 1996.
Ramsey, R.S., Moneghan, J.H., Jenkins, R.A.
Generation, sampling, and chromatographic
analysis of particulate matter in dilute sidestream
tobacco smoke. Analytica Chimica Acta 236: 213-
220, 1990.

103
Smoking and Tobacco Control Monograph No. 9
Repace, J.L., Ott, W.R., Klepeis, N.E. indoor air
pollution from cigar smoke. (Chapter 5) in: Cigars:
health effects and trends, Monograph 9, D. Burns,
K.M. Cummings, D. Hoffmann (eds.). USDHHS
NIH NCI, Bethesda, MD. U.S. Department of Health
and Humans Services, National Institutes of Health,
1998.
Rice, R.L., Scherbak, M. A method for measuring the
burning characteristics of cigars. Beiträge zur
Tabakforschung 8:326-329, 1976.
Rickert, W.S., Robinson, J.C., Bray, D.F., Roberts, B.,
Collishaw, N.E., Characterization of tobacco
products: a comparative study of the tar, nicotine
and carbon monoxide yield of cigars manufactured
cigarettes and cigarettes made from fine cut
tobacco. Preventative Medicine 14:226-233, 1985.
Roberts, D.L. Natural tobacco flavor. Recent Advances
in Tobacco Science 14:49-113, 1988.
Russell, M.A.H. The case of the medium-nicotine, low-
tar, low-carbon monoxide cigarette Banbury Reports
3:297-310, 1980.
Sato, S., Seino, Y., Ohka, T., Yahagi, T., Nagao, M.,
Matsushima, T., Sugimura, T. Mutagenicity of
smoke condensates from cigarettes, cigars and pipe
tobacco. Cancer Letters 3 (1-2):1-8, 1977.
Scassellati-Sforzolini, G., Savino, A. Evaluation of a
rapid index of ambient contamination by cigarette
smoke in relation to the composition of gas phases
of the smoke. Rivista Italiana di Igiene 28:43-55,
1968.
Schmeltz, I., Brunnemann, K.D., Hoffmann, D.,
Cornell, A. On the chemistry of cigar smoke:
Comparisons between experimental little and large
cigars. Beiträge zur Tabakforschung 8:367-377, 1976a.
Schmeltz, I., dePaolis, A., Hoffmann, D. Phytosterols
in tobacco: Quantitative analysis and fate in
tobacco combustion. Beiträge zur Tabakforschung
8:211-218, 1975a.
Schmeltz, I. Hoffmann, D., Wynder, E.L. The
influence of tobacco smoke on indoor atmospheres.
I. An overview. Preventive Medicine 44:66-82, 1975b.
Schmeltz, I., Schlotzhauer, W.S. Volatile acids in cigar
smoke. Tobacco Science 5:92-94, 1961.
Schmeltz, I., Tosk, J., Hoffmann, D. Formation and
determination of naphthalenes in cigarette smoke.
Analytical Chemistry 48:645-650, 1976 (b).
Schmeltz, I., Wenger, A., Hoffmann, D., Tso, T.C.
Chemical studies on tobacco smoke. LXIII. On the
fate of nicotine during pyrolysis and in a burning
cigarette. Journal of Agricultural and Food Chemistry
27:602-608, 1979.
Schottenfeld, D. Epidemiology of cancer of the
esophagus. Seminars in Oncology 11 (2):92-100,
1984.
Sheets, T.J. Pesticide residues on tobacco: Perceptions
and realities. Recent Advances in Tobacco Science
17:33-69, 1991.
Sloan, C.H., Morie, G.P. Determination of
unprotonated ammonia in whole cigarette smoke.
Beiträge zur Tabakforschung 8:362-365, 1976.
Spears, A.W., Laser, C.W., Bell, J. Quantitative
determination of alkalis in cigarette smoke. Journal
of Gas Chromatography 1:34-37, 1963.
Stahly, EE, Lard, E.W. Further considerations of metal
carbonyls in tobacco smoke. Chemistry and Industry,
London pp. 85-86, 1977.
Stedman, R.L., Chamberlain, W.J., Miller, R.L. High
molecular weight pigment in cigarette smoke.
Chemistry and Industry, London pp. 1560-1562,
1966.
Sunderman, F.W. Sr., Sunderman, F.W. Jr. Nickel
poisoning. XI. Implication of nickel as a pulmonary
carcinogen in tobacco smoke. American Journal of
Clinical Pathology 35:203-209, 1961.
Szadkowski, D., Harke, H.P., Angener, J. Burden of
carbon monoxide from passive smoking in offices.
Innere Medizin 3:310-313, 1976.
Thompson, C.V., Jenkins, R.A., Higgins, C.A. A
thermal desorption method for the determination
of nicotine in indoor environments. Environmental
Science and Technology 23:429-435, 1989.
Touey, G.P., Mumpower, R.C.II. Combustion-zone
temperatures in cigars and cigarettes. Meeting of
the Cigar Manufacturers’ Association of America
Inc. Atlantic City, NJ, Dec 4-5, 1957.
Touey, G.P., Mumpower, R.C.II. Measurement of the
combustion-zone temperatures of cigarettes.
Tobacco Science 1:33-37, 1957b.
Tso T.C. Production, Physiology and Biochemistry of
the Tobacco Plant. Beltsville, MD: IDEALS Inc.,
1990.
Tso, T.C., Harley, N., Alexander, L.T. Radium-226 and
polonium-210 in burley and cigar wrapper tobacco.
Tobacco Science 10:105-106, 1966 (a).
Tso, T.C., Harley, N., Alexander, L.T. Source of lead-
210 and polonium-210 in tobacco, Science 153:880-
882, 1966 (b).
Turner, J.A., McM, Sillett, R.W., McNicol, M.W. Effect
of cigar smoking on carboxyhemoglobin and
plasma nicotine concentrations in primary pipe
and cigar smokers and in cigarette smokers. British
Medical Journal 2:1387-1389, 1977.
U.S. Department of Health, Education, and Welfare.
The Health Consequences of Smoking. A Report of the
Surgeon General: 1972. U.S. Department of Health,
Education, and Welfare, Public Health Services and
Mental Health Administration. DHEW Publication
No. (HSM) 72-7516, 1972.
U.S. Department of Health, Education, and Welfare.
Smoking and Health. A Report of the Surgeon General.
U.S. Department of Health, Education, and
Welfare, Public Health Service, Office of the
Assistant Secretary for Health, Office on Smoking
and Health. DHEW Publication No. (PHS) 79-
50066, 1979.

Chapter 3
104
U. S. Department of Health and Human Services. The
Health Consequences of Involuntary Smoking. A Report
of the Surgeon General. DHHS (CDC) 87-8398,
Washington D.C., 1986.
U. S. Department of Health and Human Services. The
Health Consequences of Smoking. Nicotine Addiction. A
Report of the Surgeon General. DHHS Publication No.
(CDC) , 88-8406. Rockville, MD. U.S. Dept of
Health and Human Services. Office on Smoking
and Health, 1988.
U. S. Department of Health and Human Services.
Reducing the Health Consequences of Smoking: 25
Years of Progress. A Report of the Surgeon General.
DHHS Public No. (CDC) 89-8411, Washington
D.C., 1989.
U. S. Department of the Treasury, Bureau of Alcohol,
Tobacco & Firearms. Tobacco-Subpart B. Definitions
of cigars. Federal Register, pp. 141-143, April 1, 1996.
U. S. Environmental Protection Agency. Maleic
hydrazide. Notification of issuing of intent to suspend
pesticide registrations, Federal Register 46 (179):45999-
46000, 1981.
U. S. National Council on Radiation Protection and
Measurement. Ionizing radiation exposure of the
population of the United States. National Council on
Radiation Protection Rept. 93, Bethesda, MD, 1987.
Van der Boor, P. Consistent high quality , a telling
mark of the machine-made cigar Tobacco Journal
International 35186, 32-35, 1996.
Voges, E. Tobacco Encyclopedia. Tobacco Journal
International, Mainz, Germany, 1984.
Wald, N.J., Idle, M., Boreham, J., Bailey, A. Carbon
monoxide in breath in relation to smoking and
carboxyhemoglobin levels. Thorax 36:366-369,
1981.
Weber, A., Fischer, T. Passive smoking at work.
International Archives of Occupational and
Environmental Health 47 (31):209-221, 1980.
Wiernik, A., Christakopoulos A., Johansson, L.,
Wahlberg, I. Effect of air-curing on chemical
composition of tobacco. Recent Advances in Tobacco
Science 21:39-80, 1995.
Wolf, F. A. Tobacco production and processing. In:
Tobacco and Tobacco Smoke: Studies in Experimental
Carcinogenesis. E.L. Wynder and D. Hoffmann,
(eds.) New York: Academic Press, 5-41, 1967.
Wynder, E.L., Hoffmann, D., eds. Tobacco and
Tobacco Smoke: Studies in Experimental
Carcinogenesis, New York, Academic Press, 1967.

105
Smoking and Tobacco Control Monograph No. 9
Disease Consequences of Cigar Smoking
Thomas G. Shanks and David M. Burns
This chapter is a review of the health effects of cigar use. It is an
extension of chapters on pipes and cigars from the 1973 and 1979 Reports
of the U.S. Surgeon General entitled the Health Consequences of Smoking and
the Smoking and Health (DHHS 1973; DHHS 1979). Studies published during
the last two decades are emphasized, and original analyses of the cigar
smoking data subset from the CPS-I study are presented. The tables
summarizing research on specific diseases include studies discussed in the
previous publications. However, only the studies published since 1976 will
be reviewed in this chapter.
Cigar smoking has largely been a male behavior in the US, and so most
studies have exclusively utilized male populations. These data should be
applied with caution to the increasing numbers of women who are smoking
cigars.
Many epidemiological studies combine cigar and pipe smokers together,
or combine primary cigar smokers [those without prior history of cigarette
smoking] with secondary cigar smokers [those with varying histories of
prior cigarette or pipe smoking] and mixed smokers [those who currently
smoke cigars and cigarettes or pipes]. These combinations are often made
necessary by the small number of cigar smokers present in these studies, but
they make the resulting rate comparisons problematic in describing the effect
of cigar use. Further, many of the cigar studies have been done in European
countries, which have different traditions of cigar smoking, including different
tobaccos, differing sizes of cigars, and different levels of inhalation.
DEFINITION The definition of a cigar is given in another section of this monograph
OF TERMS (Chapter 3). For this chapter the term means any of the products
which are purchased as cigars. Cheroots, which are classed with cigars in
some studies, are small cigars, made of heavy-bodied tobaccos. For a more
complete discussion of tobacco products, plant varieties and manufacture,
see the IARC Monograph “Tobacco Smoking” (IARC, 1986; Chapter 3).
A primary cigar smoker is a smoker who smokes only cigars and
who has never smoked cigarettes or a pipe; these subjects give us the purest
estimation of the effect of cigar smoking. A secondary cigar smoker
currently smokes only cigars, but previously smoked cigarettes and/or a pipe,
either in combination with cigars or exclusively. Because of earlier use of
other tobaccos, the health effects of cigar smoking derived from secondary
cigar smokers may be affected by the earlier pattern of smoking.
The level of exposure to cigar smoke is usually measured in cigars per
day, which is an imprecise measure because of the varying sizes of cigars.
Some studies use a measure of grams smoked per day, weighting varying sizes
of cigars differently. Others attempt to quantify lifetime cigar consumption,

Chapter 4
106
using years of cigar smoking or equivalent pack-years of cigarettes, or some
other cumulative measure. Level of exposure is also referred to as intensity
of smoking and dose. The comparison of cigarette and cigar exposures is
further complicated by the older age of initiation of cigar smoking in
comparison to cigarette smoking (Chapter 2) and the profound effect
of duration of exposure on disease risk.
Inhalation becomes a critical issue with cigar smoking, since degree
of inhalation varies widely among cigar smokers. Many studies provide a
self-reported measure of inhalation, such as: none, slightly, moderately,
deeply. Such measures are shown to have a degree of validity by the, positive
association with rates of some diseases, such as lung cancer. Further studies
by Herling and Kozlowski (1988) and Wald and Watt (1997) have shown that
self-reported inhalation predicts expired-air carbon monoxide and
carboxyhaemoglobin levels, which argues for the validity of self-reported
inhalation measures.
The expression log(x) means the natural log of x. Absolute rates are given
in numbers of cases or deaths per 100,000 person-years. The abbreviation OR
stands for odds ratio; RR, for risk ratio. Confidence intervals are given for the
95 percent range for the given statistic. When not otherwise indicated, the
rates given are for mortality due to disease in the specified classification.
THE CPS-I STUDY The Cancer Prevention Study I of the American Cancer Society,
conducted between 1959 and 1972, was one of the largest prospective cohort
studies ever undertaken, following more than one million individuals for
twelve years (Garfinkel, 1985). Many results from the CPS-I study have been
previously published, but for cigar-related mortality rates, only summary
rates from the first four years of the follow-up period have been published
(Hammond, 1966). The ACS has made this data set available for a more
detailed analysis. Because of the size of the data set, the detail of smoking
behavior information gathered, and the relatively large number of cigar
smokers among the subjects, this study provides an opportunity to consider
the relationship of number of cigars per day and inhalation to mortality rates
from many diseases. Data from CPS-I was used because of the larger number
of cigar smokers in the study in comparison with the CPS-II.
The data gathered on each subject in the CPS-I study includes a smoking
history, with age of initiation to cigarette smoking, number of cigarettes/
cigars/pipes smoked per day, and level of inhalation, though no information
was gathered about age of initiation of smoking cigars or pipes. Since US
mortality rates for blacks are different from those for whites and because
blacks are under-represented in the CPS-I study, the analyses of CPS-I data
which follow are restricted to white subjects. Further, there are few female
cigar smokers in the data set, so the analyses are restricted to white males.
The number of subjects in various smoking behavior groups in the CPS-I
data set are given in Table 1.
In presenting results from the CPS-I data set, tables are constructed
for Mortality Rate Ratios (MRR) for various diseases in order to provide

107
Smoking and Tobacco Control Monograph No. 9
Table 1
Number of subjects in smoking groups in CPS-I Study, white male subjects
Smoking Group N
Neversmokers 92,307
Current Primary Cigar Smokers 15,191
Current Primary Pipe Smokers 9,623
Current Cigarette Only Smoker 174,997
Current Cigar, Pipe & Cigarette Smokers 3,471
Current Mixed Cigar & Pipe Smokers 6,767
Current Mixed Cigar & Cigarette Smokers 10,294
Current Mixed Pipe & Cigarette Smokers 11,470
Current Secondary Cigar Smokers 7,404
Current Secondary Pipe Smokers 7,033
Former Primary Cigar Smokers 5,446
Former Primary Pipe Smokers 3,549
Former Cigarette Only Smokers 42,225
Former Mixed Cigar & Cigarette 4,649
Former Mixed Pipe & Cigarette 10,724
Former Mixed Cigar & Pipe 3,952
Former Cigar, Pipe & Cigarette Smokers 6,921
Total White Male Subjects 442,455
comparisons between smoking groups. All MRR’s compare a smoking group
to the neversmoker group and are age-standardized to the neversmoker
age distribution from the study. See the appendix on methods for details.
All rates given are rates of mortality, as specified by the primary cause of
death from the death certificate.
In the tables presenting CPS-I rate ratios, primary and secondary cigar
smokers are divided into levels of 1-2, 3-4, and 5 or more cigars per day.
Smokers of both cigars and cigarettes have tobacco exposure information
available for cigarettes only. Levels of inhalation for all smokers are
subjectively reported by the subjects, using the following scale: none, slightly,
moderately, deeply. The distribution of these responses for primary and
secondary cigar smokers and cigarette only smokers is given in Figure 1 and
reveals that cigarette smokers are much more likely to report deep inhalation
than primary cigar smokers, with secondary cigar smokers having an
intermediate pattern. These inhalation patterns show that primary and
secondary cigar smoker rates, when not stratified by levels of inhalation, are
dominated by individuals who inhale slightly or not at all; whereas,
unstratified cigarette-only smoker rates are dominated by those who inhale
moderately or deeply. Degree of inhalation is a continuum, with the
subjective evaluation providing only an approximate measure.

Chapter 4
108
Figure 1
Levels of inhalation from CPS-1 study
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
Percent reporting
Primary Cigar Cigarette OnlySecondary Cigar
78.4%
14.1%
4.0%
0.5%
58.0%
23.8%
13.0%
2.2%
5.9%
13.1%
55.4%
24.8%
Level of Inhalation:
none
slightly
moderately
deeply

109
Smoking and Tobacco Control Monograph No. 9
Table 2
All cause mortality and cigar smoking: mortality ratios by type of smoking (males only, except as noted)
Rate Ratio (RR)
Never- Mixed, Cigar
Prospective Studies Sample Size* Smoker Cigar & Cigarette Cigarette
Hammond & Horn (1958) 187,783 1.0 1.22 1.36 1.68
Doll & Peto (1976) 41,000 1.0 1.09** 1.20 1.64
Best (1966) 78,000 1.0 1.06 1.22 1.54
Kahn (1966) 293,000 1.0 1.10 1.51 1.84
Hammond (1966) 440,559 1.0 1.25 1.57 1.86
Carstensen (1987) 25,129/1,256/131 1.0 1.39 (1.16-1.65) 1.45 (1.36-1.54)
Sandler (1989) 46,926/1,671/504 1.0 1.20** (1.07-1.35) 1.41 (1.29-1.55)
Lange (1992) male 6,511/808/326 1.0 1.6 (1.3-2.0) 1.9 (1.6-2.4) plain
1.8 (1.4-2.3) filter
Lange (1992) female 7,703/770/185 1.0 1.8 (1.4-2.2) 2.4 (2.0-2.9) plain
1.7 (1.4-2.1) filter
Ben-Shlomo (1994) secondary 19,018/658/132 1.0 1.20 (1.01-1.43) 2.00 (1.92-2.07)
Wald & Watt (1997) primary 21,520/1,309/113 1.0 1.23**(0.99-1.75) 2.26 (1.97-2.58)
Wald & Watt (1997) secondary 21,520/522/69 1.33**(1.03-1.73)
CPS-I primary 442,455/15,072/3,754 1.0 1.08 (1.05-1.12) 1.47 (1.41-1.53) 1.66 (1.64-1.68)
CPS-I secondary 442,455/7,349/1,462 1.12 (1.06-1.18)
* for prospective studies reviewed, the number of cigar smokers and number of deaths in this group are also given.
**cigar and pipe combined

Chapter 4
110
ALL CAUSE There is a consistent pattern of elevated overall mortality for all groups
MORTALITY of smokers, and a dose-response effect for increasing exposure to tobacco
smoke is present in the CPS-I data. The exposure is variously measured as
cigars/cigarettes/pipes per day, grams of tobacco per day, lifetime dose in
pack-years, duration of smoking, etc. and can be further modified by
describing the level of inhalation of smoke.
In a Swedish prospective mortality study which followed 25,129 men
from 1963 through 1979 (Carstensen, 1987), the All-Cause Mortality RR for
cigar-only smokers is 1.39 (1.16-1.65) compared to neversmokers, based on
131 deaths during the follow-up period. The corresponding RR for cigarette-
only smokers is 1.45 (1.36-1.54). The cigar only group is based on smoking
behavior at the time of the initial survey, and thus is a combination of
primary and secondary cigar smokers. The authors note that no information
is available on inhalation patterns of Swedish cigar smokers. Rates are
standardized by age and residence.
In a 12-year follow-up study of 46,926 individuals of both sexes in
Washington County, Maryland (Sandler, 1989) from 1963-1975, for pipe/
cigar smokers a RR of All Cause Mortality of 1.83 (1.13-2.96) was calculated
for men under 50 years of age and 1.13 (1.00-1.28) for men over 50 years of
age, providing an overall rate of 1.20 (1.07-1.35). These rates were adjusted for
age, housing quality, schooling, and marital status. Smoking categories were
based on usage at the time of the 1963 interview and do not reflect prior
history or changes during the follow-up.
Lange et al. (1992) report on the Copenhagen City Heart Study, a Danish
prospective population-based study of 6,511 men and 7,703 women, followed
from 1976 through 1989, which included 1,578 smokers of cheroots/cigars
of both sexes. The questionnaire included an inhalation question (yes/no).
Smoking groups are based on behavior at enrollment and do not distinguish
based on previous smoking. Thus cigar/cheroot includes both primary and
secondary cigar/cheroot smokers. This study found a RR of total mortality
for cigar/cheroot smokers of 1.8 (1.4-2.2) in women and 1.6 (1.3-2.0) in men,
age-adjusted and compared to neversmokers of the same sex. These rates are
somewhat lower than those found for smokers of unfiltered cigarettes, which
were 2.4 (2.0-2.9) for women and 1.9 (1.6-2.4) for men. Mortality rates for
cigar/cheroot smokers with self-reported inhalation were compared with
cigarette smokers who reported inhaling. For those cigar/cheroot smokers
with inhalation, the ratio of total mortality for women was 1.6 (1.2-2.2)
compared to female smokers of cigarettes who inhaled; and 1.0 (0.8-1.2) for
male cigar/cheroot smokers with inhalation compared to male smokers of
cigarettes with inhalation. For cigar/cheroot smokers who do not inhale,
the ratios as compared to inhaling cigarette smokers were 0.6 (0.5-0.8) for
women and 0.7 (0.6-0.8) for men, both significantly lower.
Ben-Shlomo et al. (1994) present smoking results from the Whitehall
prospective cohort study of 19,018 men from the British Civil Service
aged 40-69, with 18 years of follow-up beginning in 1967. Too few primary
cigar smokers (n=105) were available for reliable results. Secondary cigar

111
Smoking and Tobacco Control Monograph No. 9
smokers (n=658) produced a significantly elevated age-adjusted RR for all-
cause mortality of 1.20 (1.01-1.43) when compared to neversmokers, while
current cigarette smokers (n=7,921) had a RR of 2.00 (1.92-2.07). The authors
note that the RR for secondary cigar smokers is similar to that for former
cigarette smokers who had a RR of 1.15 (1.08-1.23). Smoking categories are
based on questions at the beginning of the study, with no reclassification
during the 18 years of follow-up.
Wald and Watt (1997) compare primary cigar and pipe smokers and
secondary cigar and pipe smokers who switched from cigarettes at least
20 years previously to neversmokers, former smokers, and cigarette smokers,
using data from a prospective study of 21,520 professional men in London
aged 35-64 years, recruited in 1975-82 and followed to October 1993.
Compared to neversmokers, primary pipe/cigar smokers have an age-adjusted
RR of mortality of 1.23 (0.99-1.75) and secondary pipe/cigar smokers who
switched from cigarettes at least 20 years previously have a RR of 1.33 (1.03-
1.73), while cigarette smokers have a RR of 2.26 (1.97-2.58). The study
includes self-reported inhalation level and carboxyhaemoglobin saturation at
initial exam. Comparison of these measures confirm the validity of self-
reported inhalation measures; both demonstrate the relatively higher levels of
inhalation of secondary cigar and pipe smokers compared to primary (never-
cigarette) cigar and pipe smokers. Carboxyhaemoglobin saturation was found
to be related to the risk of the three smoking related diseases investigated
[coronary heart disease, lung cancer, and COPD] across all smoking categories,
and in their analysis explained all of the variance related to smoking. A lower
level of mean total tobacco consumption of 8.1 g/day is noted for both
primary and secondary pipe and cigar smokers compared to 20.0 g/day for
cigarette smokers. Group classification is based on data from the initial
examination and does not reflect any changes in smoking behavior during
the average 14.3 years of follow-up.
The All Cause Mortality ratios for the CPS-I data are given in Tables 3 and
4, by numbers of cigars/cigarettes per day and level of inhalation. Generally
rates are significantly elevated as compared to neversmokers. Only the lowest
level of smoking (1-2 cigars per day) fails to show significance in the risk for
combined ages for primary and secondary cigar smokers. In every case
MRR's are particularly elevated for smokers less than 65 years of age.
There are positive gradients with numbers of cigars per day and with levels
of inhalation. Rates for moderate and deep inhalers of cigars reach levels
similar to cigarette smokers.
In order to assess the relative contributions of age, cigars per day, and
inhalation level to the rates of all-cause mortality, the primary cigar smoker
data was tabulated into cells by the factors of 5-year chronological age,
number of cigars per day (1-2, 3-4, 5+), and level of inhalation (0,1,2,3,
as coded for none, slightly, moderately, deeply). For each cell the absolute
rate of mortality was calculated. These data were subjected to a step-wise
multivariate Poisson regression with each factor and its log square and square
root transforms included as factors. The strongest factors in this procedure
are shown in Table 5. The purpose was to test the significance of each factor

Chapter 4
112
Table 3
Rate ratio of all-cause mortality by level of cigar/cigarettes per day
Age (years)
Daily Use 35-49 50-64 65-79 80+ Combined (95% CI) Deaths*
PRIMARY CIGAR 3,698/19667
1-2 0.72 1.10 1.02 0.97 1.02 (0.97, 1.07)
3-4 1.98 1.18 1.10 0.95 1.08 (1.02, 1.15)
5 + 1.64 1.38 1.17 0.98 1.17 (1.10, 1.24)
Combined 1.32 1.21 1.09 0.97 1.08 (1.05, 1.12)
SECONDARY CIGAR 1,452/19667
1-2 0.94 1.08 1.05 0.93 1.02 (0.93, 1.12)
3-4 1.37 1.57 1.26 0.74 1.17 (1.07, 1.28)
5 + 1.66 1.66 1.16 0.86 1.18 (1.08, 1.29)
Combined 1.29 1.43 1.15 0.84 1.12 (1.06, 1.18)
CIGAR & CIGARETTE 2,225/19667
1-19 1.65 1.68 1.29 1.06 1.31 (1.23, 1.39)
20 2.73 2.09 1.55 1.49 1.66 (1.55, 1.78)
21 + 2.73 2.15 1.99 1.11 1.78 (1.61, 1.97)
Combined 2.30 1.91 1.44 1.15 1.47 (1.41, 1.53)
CIGARETTE ONLY 38,220/19667
1-19 1.92 1.73 1.50 1.16 1.46 (1.43, 1.49)
20 2.45 2.15 1.70 1.29 1.69 (1.66, 1.71)
21 + 2.81 2.48 1.95 1.26 1.88 (1.85, 1.91)
Combined 2.49 2.17 1.68 1.21 1.66 (1.64, 1.68)
Based on data from CPS-I Study. Age-standardized rate ratio for smoking group compared to neversmokers.
* Number of deaths in subject group/neversmoker group.
as explanatory terms for the trend in the data, not to propose a model of
biological action. More information about the procedure followed is given
in the appendix.
Age is the strongest factor, reflecting the positive association of
advancing age with mortality. For the inhalation factor, the square and
square root transformation were assessed, in addition to the coded variable.
The square of depth of inhalation is the most significant of these inhalation
transforms, and is the most strongly significant factor in predicting the rate
of mortality. The square of inhalation was a better fit than inhalation,
emphasizing the effect of inhalation in increasing mortality rates. The
number of cigars per day also is a significant factor, though the strength
of the association is less than for age or inhalation.
Summary Risk ratios of All Cause Mortality for cigar smokers are higher than rates
for neversmokers, though generally lower than rates observed for cigarette
smokers. Cigar smokers who inhale exhibit all cause mortality rates that are
higher than the rates for cigar smokers who do not inhale, and the risk ratios
for inhaling cigar smoke approach the rates for cigarette smokers. The risk
ratios increase with increasing number of cigars smoked per day and
increasing depth of inhalation.

113
Smoking and Tobacco Control Monograph No. 9
Table 4
Rate ratio of all cause mortality by level of inhalation
Age (years)
Level of Inhalation 35-49 50-64 65-79 80+ Combined (95% CI) Deaths*
PRIMARY CIGAR 3,580/19667
None 1.13 1.16 1.05 0.94 1.04 (1.00, 1.08)
Slight 1.80 1.30 1.19 1.08 1.19 (1.09, 1.30)
Moderate-deep 1.02 1.87 1.72 1.22 1.60 (1.38, 1.84)
Combined 1.27 1.22 1.08 0.96 1.08 (1.04, 1.11)
SECONDARY CIGAR 1,400/19667
None 1.45 1.11 1.13 0.81 1.04 (0.97, 1.11)
Slight 1.01 1.57 1.18 0.83 1.16 (1.04, 1.29)
Moderate-deep 1.30 2.18 1.30 0.77 1.33 (1.16, 1.51)
Combined 1.32 1.40 1.16 0.81 1.11 (1.05, 1.17)
CIGAR & CIGARETTE 2,344/19667
None, slight 1.98 1.64 1.31 1.07 1.32 (1.24, 1.40)
Moderate 2.49 1.99 1.58 1.36 1.61 (1.51, 1.73)
Deep 2.68 2.41 1.92 1.24 1.84 (1.66, 2.03)
Combined 2.34 1.90 1.45 1.14 1.46 (1.41, 1.52)
CIGARETTE ONLY 39,825/19667
None, slight 2.04 1.97 1.57 1.14 1.54 (1.50, 1.57)
Moderate 2.45 2.14 1.68 1.22 1.65 (1.63, 1.67)
Deep 2.75 2.42 1.92 1.44 1.90 (1.86, 1.94)
Combined 2.49 2.18 1.68 1.20 1.66 (1.64, 1.68)
Based on data from CPS-I Study. Age-standardized rate ratio for smoking group compared to neversmokers.
* Number of deaths in subject group/neversmoker group.
Table 5
Results of step-wise poisson regression of absolute all-cause mortality rates
Variable Coeffecient SE F-test Probability
(Constant) 1.2211 0.00165
Age (years) 0.09559 0.0000217 1557.2 <10
-10
***
Inhalation
2
(0-3) 0.09887 0.000100 64.5 <10
-10
***
Cigars per day 0.02689 0.0000942 5.4 0.02*
***p<0.0001; **p<0.01; *p<0.05
CAUSE SPECIFIC The determination that cigar smoking can cause a specific disease
MORTALITY is based on a review of all the available information and draws
heavily on the similarities between the composition of cigar and cigarette
smoke described in Chapter 3. Data on cigarette smoking and disease risks
are much more extensive, and it is probably reasonable to assume that most
of the diseases caused by the inhalation of tobacco smoke from cigarettes
can be caused by the inhalation of tobacco smoke from cigars. However,
this chapter examines the data for a number of causes of death and reaches

Chapter 4
114
conclusions about the evidence on cigar smoking and disease based on a
number of criteria, including: the replication of a result in more than one
study, the presence of a dose response relationship with number of cigars
smoked per day and depth of inhalation, the demonstration of independent
effects of inhalation and number of cigars per day in a regression modeling
of the CPS-I data, and the presence of a relationship in larger and better
controlled studies.
LUNG CANCER The causal link between cigarette smoking and lung cancer has led to
a number of studies examining a similar link between cigar and pipe smoking
and lung cancer. These studies have demonstrated an elevated risk for lung
cancer among cigar smokers, but the magnitude of the risk is lower than that
for cigarette smokers. The 1979 review article provides references to studies
up to that time (DHHS, 1979). Table 6 summarizes the case-control and
prospective studies of lung cancer and cigar smoking.
Joly, Lubin, and Caraballoso (1983) conducted a case-control study of
male and female lung cancer cases in Cuba, in part focused on differentiating
level of risk between dark Cuban and lighter Virginia tobaccos. Analyses
are provided for male cigar only and mixed cigar and cigarette smokers. No
separation is made between primary and secondary cigar smokers. Controls
are a mixed group of hospital non-tobacco-related cases and neighborhood
matches. For cigar-only smokers an OR of 4.4 (2.3-8.2) is reported overall; for
mixed smokers a OR of 15.0 (9.0-24.9) is reported, comparing to the OR of
14.1 (8.8-22.6) for male cigarette smokers. There was a significant increase
in lung cancer risk with increasing duration of smoking for both groups
of cigar smokers, but the level of daily consumption was not significantly
related to risk. Depth of inhalation for cigar-only smokers is reported, noting
a significant positive trend in OR with increasing depth and frequency of
inhalation. There was a significant trend for mixed smokers of cigars and
cigarettes to inhale more frequently and more deeply than cigar-only smokers.
Lubin, Richter, and Blot (1984) present the cigar and pipe subset of a
larger case-control study of western European male lung cancer cases, with
6,920 cases and 13,460 controls. Controls matched hospital patients whose
admission was not for a tobacco-related illness. There were 37 cases with cigar-
only smoking with an estimated RR of 2.90 (2.1-4.0) and 180 mixed cigarette
and cigar cases with a RR of 6.87 (5.5-8.5). Tables in the paper present the
trend with years of cigar smoking (not significant) and number of cigars per
day (significant), which increases to a RR of 8.93 (6.8-11.1) for smokers of
7 or more cigars per day. A table presents significant increasing risk with both
frequency and depth of inhalation for cigar only smokers, though the same
table for mixed cigar and cigarette smokers is not significant. When smoking
cigars, mixed cigar/cigarette smokers were more likely to inhale than cigar -
only smokers; and when smoking cigarettes, less likely to inhale than cigarette-
only smokers.
Benhamou, Benhamou, and Flamant (1986) present analysis of the
cigar smoking subset of 1,529 French lung cancer cases: 9 are exclusive cigar
smokers and 68 are mixed cigar and cigarette smokers, compared to exposure

115
Smoking and Tobacco Control Monograph No. 9
Table 6
Lung cancer and cigar smoking: mortality ratios by type of smoking (males only except as noted)
Odds Ratio (OR)
Never- Mixed, Cigar
Prospective Studies Sample Size* Smoker Cigar & Cigarette Cigarette
Levin (1950) 236/481 0.7 2.1
Schrek (1950) 82/522 0.6 1.7
Wynder & Graham (1950) 605/780 5.1 15.7
Sadowsky (1953) 477/615 2.4 5.6 3.7
Wynder & Cornfield (1953) 63/133 2.5 8.5
Randig (1954) 415/381 5.3 5.0
Mills & Porter (1950) 444/430 6.0** 5.4
Mills & Porter (1957) 484/1588 2.8** 4.5
Lombard & Snegireff (1959) 500/1839 1.7** 8.1
Wicken (1966) 803/803 2.2** 4.2 4.3
Abelin & Gsell (1967) 118/524 3.4 5.7
Wynder (1970) 210/420 2.0** 12.4
Joly (1983) 607/1,108 4.4 (2.3-8.2) 15.0 (9.0-24.9) 14.1 (8.8-22.6)
Lubin (1984) 6,920/13,460/37 2.90 (2.1-4.0) 6.87 (5.5-8.5) 9.03 (7.9-10.3)
Benhamou (1986) 1,529/2,899 5.6 (2.3-13.5) 8.5 (5.4-13.6) 13.3 (9.3-19.1)
Higgins (1988) 2,085/3,948 3.1 (1.8-5.6) 10.5 (7.8-14.4) 16.0 (12.2-20.9)
10+ cigars/day 25.1 (7.2-87.4)

Chapter 4
116
Table 6 (continued)
Rate Ratio (RR)
Never- Mixed, Cigar
Prospective Studies Sample Size* Smoker Cigar & Cigarette Cigarette
Hammond & Horn (1958) 187,783 1.0 1.02 7.63 10.73
Doll & Peto (1976) 41,000 1.0 5.80** 8.20 14.00
Best (1966) 78,000 1.0 2.94 14.91
Kahn (1966) 293,000 1.0 1.59 12.14
Carstensen (1987) 25,129/1,256/11 1.0 7.6 (3.7-13.6) 7.4 (5.8-9.3)
Lange (1992) male 6,511/808/47 1.0 6.0 (2.2-17) 7.3 (2.6-20) plain
6.0 (2.2-19) filter
Lange (1992) female 7,703/770/14 1.0 4.9 (3.0-12) 7.9 (2.9-21) plain
4.8 (1.7-13) filter
Ben-Shlomo (1994) secondary 19,018/658/20 1.0 7.64 (4.6-11.8) 11.92 (10.7-13.2)
Wald & Watt (1997) primary 21,520/1,309/6 1.0 3.19** (1.07-9.50) 16.4 (7.55-44.2)
Wald & Watt (1997) secondary 21,520/522/9 8.64** (3.19-23.3)
CPS-I primary 442,455/15,072/73 1.0 2.10 (1.63-2.65) 11.31 (9.72-13.07) 12.39 (11.97-12.83)
CPS-I secondary 442,455/7,349/86 6.29 (5.01-7.79)
*For prospective studies reviewed, the number of cigar smokers and number of deaths in this group are also given.
**Cigar and pipe combined.

117
Smoking and Tobacco Control Monograph No. 9
data from 2,899 matched hospital controls. In comparison to non-smokers,
this study yields an OR of 5.6 (2.3-13.5) for the cigar only smokers and
8.5 (5.4-13.6) for the mixed cigar and cigarette smokers, as compared to
an OR of 13.3 (9.3-19.1) for the cigarette only smokers. A test of secondary-
cigar smokers yielded lower risk (RR=0.40, p<.01) compared to cigarette only
smokers after adjustment for combined duration of smoking. The authors
explain this lower risk as an effect of reduction in inhalation reported when
changing from cigarettes to cigars, cigar-only smokers reporting lower rates
of inhalation than mixed cigar and cigarette smokers, and cigarette-only
smokers reporting highest levels of inhalation.
Higgins, Mahan, and Wynder (1988) present the cigar and pipe subset of a
lung cancer case-control study involving 24 hospitals in 6 cities of the United
States, including 2,085 cases and 3,948 matched hospital controls. Cigar-only
smokers have a lung cancer OR of 3.1 (1.8-5.6), based on 18 cases. Former
cigar only smokers have an OR of 2.5 (1.3-4.8), based on 12 cases quit for at
least one year. Mixed smokers, comprised of cigarette and cigar, cigarette
and pipe, or smokers of all three products, have an OR of 10.5 (7.8-14.4).
The authors also examine the change in lung cancer risks among cigarette
smokers who switch to cigars, as compared to those who quit smoking all
tobacco products. A table, partially reproduced in Figure 2, shows the
continuing risk for secondary cigar and/or pipe smokers broken into decades
of years since switching from cigarettes to cigar/pipe smoking. Figure 2 shows
uniformly higher risks for secondary cigar/pipe smokers than for former
cigarette smokers who have stopped all smoking, suggesting that the benefits
of cessation or cigarette smoking are diminished in the presence of continued
cigar use. Analyses of dosage, duration of smoking and inhalation were
performed combining primary cigar and pipe smokers (never smoked
cigarettes), by weighting each cigar or pipeful as one unit. This comparison
showed smokers of fewer than 5 cigars/pipefuls per day as not different from
neversmokers with an OR of 0.8 (0.3-2.1), but smokers of 5-9 cigars/pipefuls
per day have an OR of 3.2 (1.6-6.3) and smokers of 10 or more cigars/pipefuls
per day an OR of 6.7 (3.4-13.3). The group smoking ten or more cigars per day
excluding pipe smokers, has an OR of 25.1 (7.2-87.4). The risk with duration
of smoking is significant after 30 years of smoking. Rates are significantly
elevated for cigar/pipe smokers who inhale, with OR of 12.3 (4.0-37.7)
compared to an OR of 2.3 (1.4-3.8) for those who do not inhale.
In a large prospective study of 25,129 Swedish men from 1963 through
1979, as reported by Carstensen, Pershagen, and Eklund (1987), approximately
5 percent of the study population were cigar smokers. For lung cancer, an age-
adjusted RR of 7.6 (3.7-13.6) is reported for cigar only smokers, which is
similar to the overall risk of 7.4 (5.8-9.3) for cigarette smokers. The test for
trend by grams/day of any tobacco is highly significant. There is a similar
linear trend in RR for lung cancer by grams/day of tobacco smoked for
cigarette, pipe and cigar comsumption, with the RR for cigars slightly lower.
Tobacco use habits were only recorded at the beginning of the study and do
not account for changes in smoking pattern during the 17 years of the study.

Chapter 4
118
Figure2
Decreasing odds ratio for lung cancer by years of cessation of cigarette smoking,
by quitting or switching to cigars/pipe (Higgins, 1988).
In the Danish prospective study previously discussed (Lange, 1992),
overall mortality from lung cancer for male smokers of cheroots/cigars was
reported at an age-adjusted RR of 6.0 (2.2-17) versus neversmokers, compared
to the RR of 7.3 (2.6-20) for smokers of non-filter cigarettes and
6.0 (2.2-19) for smokers of filter cigarettes. For females, the corresponding
RRs are 4.9 (3.0-12) for cheroot/cigar-only smokers, 7.9 (2.9-21) for plain
cigarettes, and 4.8 (1.7-13) for filter cigarettes. In comparing mortality rates
by inhalation level, the inhaling cigarette smoker is used as the comparison
group. The RR for inhaling cigar/pipe smokers is 1.1 (0.7-1.6); for non-
inhaling cigar/pipe smokers, 0.4 (0.3-0.6). Cigarette smokers who do not
inhale are reported at 0.2 (0.1-0.8), also significantly lower than inhaling
cigarette smokers. For females, the Risk Ratio of inhaling cigar/cheroot
smokers compared to inhaling cigarette smokers is 1.5 (0.5-3.7); the
comparison of non-inhaling cigar/cheroot smokers to inhaling cigarette
smokers, 0.4 (0.2-0.9); and non-inhaling cigarette smokers to inhaling
cigarette smokers, 0.3 (0.1-0.8). The categories of tobacco use are a snapshot
of the habits at enrollment in the study and do not reflect prior useage
or changes during the period of follow-up. Consequently, primary and
secondary cigar smokers are pooled, and reported rates may be higher
than would be found for primary cigar/cheroot smokers. Conversely,
any cessation or reduction in smoking during the period of the study
would not be reflected in these statistics.
14
12
10
8
6
4
2
0
<10 yrs
Odds Ratio for lung cancer mortality
10-19 yrs 20-29 yrs 30+ yrs
Years of cigarette smoking cessation
12
11.9
9.9
6.1
5.3
3.7
4.8
1.9
secondary
cigar / pipe
former
smoker

119
Smoking and Tobacco Control Monograph No. 9
Wald and Watt (1997) report an age-adjusted RR of lung cancer of
3.19 (1.07-9.50) for primary cigar/pipe smokers and 8.64 (3.19-23.3) for
secondary cigar/pipe smokers who switched from cigarettes at least 20 years
before the beginning of the study, compared to a RR of 16.4 (7.55-44.2) for
current cigarette smokers. These rate differences are consistent with the
pattern of total tobacco consumption and levels of inhalation noted earlier.
Tables 7 and 8 present age-standardized lung cancer mortality ratios from
the CPS-I study by level of cigars/cigarettes per day and by level of inhalation.
Generally these tables show a positive gradient with quantity smoked. The
gradient in Table 8 for levels of inhalation is strongly positive, with highest
rates for the deepest inhalation level.
To assess the strength of association of the factors of numbers of cigars
per day and level of inhalation to rates of lung cancer deaths, the absolute
rates of lung cancer for primary cigar smokers were subjected to a step-wise
Poisson analysis of variance. For details, see the appendix. The results are
summarized in Table 9.
Depth of inhalation shows the strongest association with rates of
lung cancer deaths. The values for inhalation are an arbitrary scale for the
responses: ‘none’, ‘slight’, ‘moderate’, and ‘deeply’. The square and square
root transform of the values were also tested in the regression, with the
square transformation testing as the strongest factor. The chronological age
variable is also highly significant, but in contrast to the analysis of all cause
mortality, age is a less powerful predictor of lung cancer risk than inhalation.
The number of cigars per day is also significant in predicting rates, with a
positive slope.
Age specific lung cancer death rates from CPS-I for cigar smokers of
various numbers of cigars smoked per day and different inhalation patterns
can be modeled to compare the effects of number of cigars smoked per day
and inhalation on lung cancer death rates. Figure 3 is a graph of the modeled
rates of lung cancer deaths for several cigar smoking groups, in comparison to
smokers of 20 cigarette per day rates and neversmokers. All rate curves are
based on Poisson regression of observed absolute rates. The rates for cigar
smokers vary depending on the parameters of smoking behavior. Cigar
smokers smoking five or more cigars per day with moderate inhalation
approach the rates of smokers of 20 cigarette per day; cigar smokers smoking
one or two cigars per day with no inhalation are near rates for neversmokers.
The modeled rates in Figure 3 present a pattern of disease risk for cigar smokers
that increases with increasing exposure of the lung to cigar smoke. As the
number of cigars smoked per day increases and more importantly, as the depth
of inhalation increases, the risk of developing lung cancer increases from those
of someone who has never smoked to those of someone who has smoked 20
cigarettes per day.
Summary Studies of lung cancer mortality among cigar smokers provide a convincing
pattern of elevated lung cancer risks for cigar smokers. Lung cancer mortality
ratios increase with increasing number of cigars smoked per day and with

Chapter 4
120
Table 7
Rate ratio of cancer of the lung and bronchus by level of cigar/cigarettes per day
Age (years)
Daily Use 35-49 50-64 65-79 80+ Combined (95% CI) Deaths*
PRIMARY CIGAR 73/191
1-2 0.83 1.27 0.66 0.9 (0.54,1.66)
3-4 2.35 3.02 1.02 2.36 (1.49,3.54)
5 + 13.71 3.86 3.19 2.10 3.40 (2.34,4.77)
Combined 4.04 2.24 2.34 1.09 2.10 (1.63,2.65)
SECONDARY CIGAR 83/191
1-2 7.86 2.18 3.20 4.16 3.18 (1.78,5.24)
3-4 6.78 10.84 6.54 8.52 (5.87,11.97)
5 + 11.92 5.97 7.21 (5.02,10.03)
Combined 2.93 6.98 6.54 4.98 6.29 (5.01,7.79)
CIGAR & CIGARETTE 182/191
1-19 5.35 6.92 8.22 7.57 7.64 (5.87,9.77)
20 12.03 14.31 17.24 19.69 16.73 (13.24,20.85)
21 + 8.56 19.18 15.46 13.37 (9.55,18.21)
Combined 8.51 11.81 11.78 9.69 11.31 (9.72,13.07)
CIGARETTE ONLY 3,166/191
1-19 5.17 7.17 8.38 2.39 6.75 (6.18,7.37)
20 12.51 13.03 14.72 8.15 12.86 (12.14,13.60)
21 + 13.09 19.48 23.36 14.62 20.23 (19.20,21.30)
Combined 11.18 13.97 14.28 5.61 12.39 (11.97,12.83)
Based on data from CPS-I Study. Age-standardized rate ratio for smoking group compared to neversmokers.
* Number of deaths in subject group/neversmokers group.
increasing depth of inhalation. When depth of inhalation and number of
cigars per day are examined together, depth of inhalation is more powerful in
predicting lung cancer risk than number of cigars smoked per day. Limited
data exist on risks for those who switch from smoking cigarettes to smoking
only cigars, but the data that do exist suggest that lung cancer risks of
switching to cigars is substantially above that for cigarette smokers who stop
smoking all tobacco products.
Overall, lung cancer risks for cigar smokers may be similar to those seen in
cigarette smokers once they are adjusted for differences in level of inhalation
and quantity of tobacco smoked per day. The data clearly establish cigar
smoking as a cause of lung cancer.
ORAL CANCERS Both primary and secondary cigar smokers are less likely to inhale
deeply than are cigarette smokers (Figure 1), and this difference in inhalation
patterns is a major determinant of the differences in lung cancer risks that
occur due to smoking cigars and cigarettes. However, the mouth and oral
cavity are exposed to the carcinogens in smoke whether the smoke is inhaled
or not.

121
Smoking and Tobacco Control Monograph No. 9
Table 9
Results of step-wise poisson regression of absolute rates of lung cancer deaths
Variable Coeffecient SE F-test Probability
(Constant) –2.4107 0.0119
Inhalation
2
(0-3) 0.3557 0.000523 37.2 <10-
7
***
Age (years) 0.07514 0.000159 27.7 <10
-5
***
Cigars per Day 0.2324 0.000727 11.7 0.001**
***p<0.0001; **p<0.01; *p<0.05
Table 8
Rate ratio of cancer of the lung and bronchus by level of inhalation
Age (years)
Level of Inhalation 35-49 50-64 65-79 80+ Combined (95% CI) Deaths*
PRIMARY CIGAR 69/191
None 1.94 2.30 1.16 1.97 (1.48,2.57)
Slight 2.90 1.02 1.89 (0.81,3.72)
Moderate-deep 6.96 5.90 4.93 (1.80,10.72)
Combined 4.09 2.36 2.27 1.15 2.11 (1.64,2.67)
SECONDARY CIGAR 83/191
None 5.30 5.99 4.78 5.41 (3.93,7.27)
Slight 11.25 7.00 6.78 10.22 7.63 (4.66,11.78)
Moderate-deep 12.79 12.35 9.77 (5.88,15.25)
Combined 2.99 6.93 6.87 5.15 6.47 (5.15,8.01)
CIGAR & CIGARETTE 183/191
None, slight 10.29 11.65 4.86 9.64 (7.75,11.85)
Moderate 10.48 10.04 8.50 28.16 12.92 (9.81,16.70)
Deep 18.80 17.90 23.12 16.84 (12.08,22.85)
Combined 8.22 11.50 11.84 9.53 11.20 (9.66,12.92)
CIGARETTE ONLY 3,162/191
None, slight 7.68 11.76 10.72 2.47 9.33 (8.61,10.10)
Moderate 9.95 14.01 15.07 7.46 13.13 (12.53,13.75)
Deep 15.14 16.26 19.22 13.58 17.11 (16.00,18.28)
Combined 11.27 14.18 14.24 5.62 12.44 (12.02,12.88)
Based on data from CPS-I Study. Age-standardized rate ratio for smoking group compared to neversmokers.
* Number of deaths in subject group/neversmokers group.
Spitz (1988) presented a case-control study of 185 squamous cell carcinoma
of the upper aerodigestive tract, including larynx, tongue, orohypopharynx,
floor of mouth, and other cancers of the oral cavity, demonstrating an OR of
2.8 (1.5-5.5) for cigar use for all oral cancer sites combined. The cigar category
appears to include both primary and secondary cigar smokers, and non-
smokers may include ex-smokers.
Blot et al. (1988) report a case-control study of 1,114 oral and pharyngeal
cancer cases, excluding salivary and nasopharyngeal carcinoma, with 1,268

Chapter 4
122
Figure 3
Lung cancer death rates for cigar smokers with different patterns of inhalation and number of
cigars per day compared with one pack per day cigarette smokers
population-based controls. Pooling primary cigar and/or pipe smokers they
report an OR of 1.9 (1.1-3.4) adjusted for age and alcohol consumption,
which rises to 16.7 (3.7-76.7) for men smoking 40 or more cigars per week,
but this ratio is based on only 14 cases and 1 control. A positive gradient in
risk is also shown with increasing consumption of alcohol. An OR of 1.9 for
cancer of the tongue and 1.6 for cancer of the pharynx among pipe/cigar
smokers as compared to neversmokers is reported, but neither confidence
intervals nor the data to calculate them are provided.
Merletti et al. (1989) report a case-control study of cancer of the oral
cavity-oropharynx in Torino, Italy, with 122 cases of both sexes and 606
population-based controls. Male cigar smokers, with or without the
combination of other tobacco products, have a higher risk than cigarette-only
smokers based on 11 cases, with OR = 14.6 (4.7-45.6), compared to an OR of
3.9 (1.6-9.4) for cigarette smokers. OR's are age-adjusted and based on male
neversmokers rates.

123
Smoking and Tobacco Control Monograph No. 9
Table 10
Oral cancer and cigar smoking: rate ratios by type of smoking (males only)
Odds Ratio (OR)
Never- Mixed, Cigar
Case-Control Studies Sample Size* Smoker Cigar & Cigarette Cigarette
Lip
Broders (1920) 537/500 0.8 0.0
Ebenius (1943) 439/300 0.7
Levin (1950) 143/554 1.9 1.4
Sadowsky (1953) 571/615 1.1 0.4 1.4
Wynder (1957) 14/115 0.8 2.2 1.0
Staszewski (1960) 394/912 2.1** 2.4
Keller (1970) 301/265 1.4 2.6
Oral
Spitz (1988) incl larynx 185/185 2.8 (1.5-5.5) 4.5 (2.4-8.5)
Blot (1988) 1,114/1,268 1.9** (1.1-3.4) 1.9 (1.3-2.9)
40+ cigars/week 12/7 16.7 (3.7-76.7)
Merletti (1989) 86/385 14.6 (4.7-45.6) 3.9 (1.6-9.4)
Franceschi (1990) 157/1,272 20.7** (5.6-76.3) 11.1 (3.4-34.8)
Franceschi (1992) mouth 104/726 21.9** (3.8-125.6) 11.8 (3.6-38.4)
Tongue
Franceschi (1992) 102/726 3.4** (0.3-39.1) 10.5 (3.2-34.1)
Rate Ratio (RR)
Mixed, Cigar
Prospective Studies Cigar & Cigarette Cigarette
Hammond & Horn (1958) 187,783 1.0 5.00 5.06
Doll & Hill (1976) 41,000 1.0 9.00** 10.00 14.00
Hammond (1966) 440,559 1.0 4.94** 9.90
Kahn (1966) oral 293,000 1.0 4.11 4.09
Kahn (1966) pharyngeal 1.0 3.06** 12.54
Chow (1993) nasopharyngeal 248,046/2 1.0 1.0** (0.2-5.2) 3.9 (1.5-10.3)
CPS-I combined oral 442,455/15,072/26 1.0 7.92 (5.12-11.69) 10.72 (6.24-17.17) 8.23 (7.17-9.40)
*For prospective studies reviewed, the number of cigar smokers and number of deaths in this group are also given.
**Cigar and pipe combined.

Chapter 4
124
Franceschi et al. (1990) present the results of a case-control study in
northern Italy of 157 male oral cavity cancers, 134 pharyngeal cancers,
and 162 laryngeal cancers, with 1,272 male controls composed of matched
hospital inpatients with conditions unrelated to tobacco and alcohol. For
smokers of cigars or pipes only, they found an age-adjusted OR of 20.7 (5.6-
76.3) for oral cavity cancer based on 6 cases and an OR of 2.8 (0.3-26.1) for
laryngeal cancer based on 1 case, in comparison to neversmokers. Franceschi
et al. (1992) also reported a case-control study of 102 men with cancer of the
tongue and 104 patients with cancer of the mouth, compared to 726 hospital
controls. For cigar or pipe only smokers an OR of 3.4 (0.3-39.1) is calculated
for tongue cancer based on 1 case, and an OR of 21.9 (3.8-125.6) for cancer of
the mouth based on 5 cases, both compared to neversmokers.
Chow et al. (1993) report the 26-year follow-up of 250,000 US veterans.
They do not find any increased risk of nasopharyngeal cancer among cigar
and pipe-only smokers with an age-adjusted RR of 1.0 (0.2-5.2), but they do
report a RR of 3.9 (1.5-10.3) for all current cigarette smokers taken together,
compared to neversmokers.
Analyses from the CPS-I study for combined buccal and pharyngeal
cancers are presented in Tables 11 and 12. These tables include deaths
coded for lip, tongue, floor of mouth, mouth unspecified and mouth other,
oral mesopharynx, nasopharynx, hypopharynx and pharynx unspecified.
Cancer of the salivary glands is not included in this grouping because separate
analyses show that these cancers do not appear to be related to tobacco
consumption. Table 16 is included to demonstrate this lack of relationship
between cigarette smoking and cancer of the salivary glands. There are
insufficient data to provide a similar table for cigar smokers and cancer of the
salivary glands, but the lack of deaths in the cigar smoking group provides
evidence of the lack of relationship between this cancer and cigar exposure.
Rates for combined oral/pharyngeal cancers for primary and secondary cigar
smokers are approximately equal to rates for cigarette smokers (Table 11).
A positive gradient is seen with number of cigars/cigarettes per day. Rates for
smokers of 5+ cigars per day are higher than rates for smokers of 21+ cigarettes
per day. Table 12 shows a positive gradient for inhalation among cigar-only
and cigarette-only groups, with very high rates for moderate-deep inhalation
of cigars. The cigar and cigarette group does not show this effect, but the data
on inhalation here is complicated, involving two tobacco products, and the
coding for this study does not allow separate indication of inhalation for
cigars and cigarettes.
Tables 13 and 14 provide a more focused look at the pharyngeal cancers,
combining codings for oral mesopharynx, nasopharynx, hypopharynx and
pharynx unspecified. Elevated rates are observed for these cancers among
all smokers, with a strong positive gradient for numbers of cigars/cigarettes
per day and level of inhalation. Rates for cigar and cigarette smokers are
approximately equivalent, with highest rates for smokers of both cigars and
cigarettes. There is not enough data on secondary cigar smokers to generate
a table. A step-wise Poisson regression analysis confirmed a significant

125
Smoking and Tobacco Control Monograph No. 9
Table 11
Rate ratio of buccal and pharyngeal cancer combined by level of cigars/cigarettes per day*
Age (years)
Daily Use 35-49 50-64 65-79 80+ Combined (95% CI) Deaths**
PRIMARY CIGAR 25/18
1-2 2.33 2.12 (0.43,6.18)
3-4 7.06 6.56 8.51 (3.66,16.77)
5 + 10.54 15.50 15.94 (8.71,26.75)
Combined 5.33 7.37 7.92 (5.12,11.69)
SECONDARY CIGAR 8/18
1-2 4.39 (0.06,24.45)
3-4
5 + 5.23 19.62 13.73 (5.50,28.30)
Combined 1.85 6.89 6.58 (2.83,12.97)
CIGAR & CIGARETTE 17/18
1-19 9.16 6.93 7.29 (2.66,15.86)
20 12.00 15.41 13.42 (5.78,26.44)
21 + 39.04 23.86 (4.80,69.71)
Combined 8.32 13.01 10.72 (6.24,17.17)
CIGARETTE ONLY 216/18
1-19 5.98 4.99 5.93 (4.28, 8.02)
20 10.74 4.34 6.85 (5.37, 8.62)
21 + 13.41 12.21 12.04 (9.81,14.63)
Combined 10.52 6.49 8.23 (7.17, 9.40)
Based on data from CPS-I study. Age-standardized rate ratio for smoking group compared to neversmokers.
* Includes: lip, tongue, floor of mouth, other parts of mouth, mouth unspecified, oral mesopharynx, nasopharynx,
hypopharynx, pharynx unspecified, not including salivary glands.
** Number of deaths in subject group/neversmoker group.
association of absolute rates of pharyngeal cancers for primary cigar smokers
with age (F=20.5, p<.0001), inhalation (F=7.7, p<.01), and a marginally
significant association with cigars per day (F=3.6, p=.07).
The data on cancer of the tongue is summarized in Table 15, providing
comparisons based on numbers of cigars/cigarettes and depth of inhalation.
Primary and secondary cigar smokers are pooled to provide enough data.
These tables show highly elevated rates of tongue cancer for all smokers, with
a strong positive gradient by numbers of cigars/cigarettes per day and depth
of inhalation. These rates must be considered as approximate, since they are
based on only two deaths among the neversmoker comparison group, and
nine deaths among the cigar smokers.
Summary The risk of oral and pharyngeal cancers are similar for cigar smokers
and cigarette smokers, with an overall risk seven to ten times higher than for
neversmokers. Positive gradients are observed when rates are stratified by
numbers of cigars per day, demonstrating a dose-response relationship
between cigar smoke exposure and risk of these cancers. Further, the level
of inhalation affects the rates of these cancers, with highest rates for cigar
smokers who inhale moderately or deeply. No relationship between smoking

Chapter 4
126
Table 12
Rate ratio of combined buccal and pharyngeal cancer by level of inhalation*
Age (years)
Level of Inhalation 35-49 50-64 65-79 80+ Combined (95% CI) Deaths**
PRIMARY CIGAR 25/18
None 4.12 5.85 6.98 (4.13,11.03)
Slight 6.92 9.04 7.83 (1.57,22.88)
Moderate-deep 22.36 33.43 27.88 (5.60,81.46)
Combined 5.40 7.07 7.85 (5.03,11.68)
SECONDARY CIGAR 8/18
None 3.08 3.67 3.27 (0.66, 9.56)
Slight 14.32 8.75 (1.76,25.58)
Moderate-deep 13.24 24.19 (2.72,87.32)
Combined 1.89 7.08 6.77 (2.92,13.34)
CIGAR & CIGARETTE 17/18
None, slight 8.90 12.27 10.47 (4.78,19.87)
Moderate 3.42 9.62 7.02 (1.89,17.97)
Deep 15.15 14.08 13.65 (3.67,34.95)
Combined 8.01 12.31 10.20 (5.94,16.33)
CIGARETTE ONLY 227/18
None, slight 8.81 5.44 6.26 (4.47, 8.53)
Moderate 11.09 5.68 8.43 (7.00,10.06)
Deep 12.33 8.66 12.48 (9.61,15.94)
Combined 10.91 6.23 8.32 (7.27, 9.48)
Table 13
Rate Ratio of pharyngeal cancer by level of cigars/cigarettes per day*
Age (years)
Daily Use 35-49 50-64 65-79 80+ Combined (95% CI) Deaths**
PRIMARY CIGAR 12/10
1-2 6.40 3.81 (0.77,11.13)
3-4 4.23 13.51 7.52 (2.02,19.26)
5 + 4.22 19.54 9.92 (3.20,23.16)
Combined 2.52 12.19 6.73 (3.47,11.75)
CIGAR & CIGARETTE 10/10
1-19 13.40 5.36 (0.60,19.35)
20 9.60 35.02 18.81 (6.87,40.93)
21 + 79.42 31.77(3.57,114.69)
Combined 3.30 26.94 12.43 (5.95,22.86)
CIGARETTE ONLY 101/10
1-19 3.16 5.65 4.91 (2.95, 7.67)
20 5.77 7.38 6.04 (4.27, 8.29)
21 + 6.72 15.88 9.91 (7.20,13.31)
Combined 5.46 8.53 6.90 (5.62, 8.39)
* Includes: oral mesopharynx, nasopharynx, hypopharynx, and pharynx unspecified. Based on data from CPS-I study.
Age-standardized rate ratio for smoking group compared to neversmokers.
** Number of deaths in subject group/neversmoker group.
*Based on data from CPS-I Study. Age-standardized rate ratio for smoking group compared to neversmokers.
**Number of deaths in subject group/neversmokers group.

127
Smoking and Tobacco Control Monograph No. 9
Table 14
Rate ratio of pharyngeal cancer by level of inhalation*
Age (years)
Level of Inhalation 35-49 50-64 65-79 80+ Combined (95% CI) Deaths**
PRIMARY CIGAR 12/10
None 3.20 11.31 6.86 (3.28,12.61)
Slight 12.43 4.97 (0.06,27.66)
Moderate-deep 38.67 15.47 (0.20,86.07)
Combined 2.55 12.52 6.91 (3.56,12.07)
CIGAR & CIGARETTE 10/10
None, slight 28.61 11.44 (3.69,26.70)
Moderate 4.11 9.83 5.99 (0.67,21.62)
Deep 9.09 38.71 20.03 (4.03,58.52)
Combined 3.18 25.45 11.77 (5.64,21.65)
CIGARETTE ONLY 111/10
None, slight 5.92 7.06 5.79 (3.58, 8.84)
Moderate 6.04 8.98 8.16 (6.24,10.49)
Deep 6.53 8.40 9.59 (6.42,13.78)
Combined 6.04 8.24 7.34 (6.04, 8.84)
*Based on data from CPS-I study. Age-standardized rate ratio for smoking group compared to neversmokers.
**Number of deaths in subject group/neversmoker group.
and salivary gland cancer was observed. The data clearly establish cigar
smoking as a cause of oral cancer.
CANCER OF Burch et al. (1981) report a case-control study of 204 laryngeal cancer
THE LARYNX cases between 1977 and 1979 in southern Ontario compared to
matched neighborhood controls. The summary RR for cigar smokers,
estimated by logistic regression, is reported as 2.9, compared to 6.1 (3.0-12.5)
for cigarette smokers. But the criterion for the cigar category (primary,
secondary, or ever-cigar) is not stated, and the confidence interval for cigar
smokers is not reported and cannot be estimated since the numbers of cases
are not given.
Freudenheim et al. (1992) conducted a case-control study of 250 cases of
laryngeal cancer and matched neighborhood controls in western New York.
No significant trend related to cigar use is shown. Cigar use is reported in
cigar-years, without distinguishing between heavy use for a shorter period
and light use over many years. The categories of tobacco use (ever-cigarette/
ever-cigar/ever-pipe) appear to overlap, not distinguishing between mixed
cigarette and cigar smokers, secondary cigar smokers, etc; the overlapping
categories prevent clear conclusions with respect to cigar use.
Muscat and Wynder (1992) report a case-control study of laryngeal
cancer with 194 subjects and 184 age-matched hospital controls between
1985 and 1990, a subset of a larger study. Compared to neversmokers, an OR
of 4.3 (1.7-16.4), adjusted for age and alcohol use, is reported for combined
pipe and cigar smokers, apparently primary and secondary cigar/pipe smokers
combined.

Chapter 4
128
Table 15
Rate ratio of cancer of the tongue*
Age (years)
35-49 50-64 65-79 80+ Combined (95% CI) Deaths**
By Level of Cigars/Cigarettes per Day
PRIMARY & SECONDARY CIGAR 9/2
1-2
3-4 13.67 22.51 (4.52,65.76)
5 + 23.96 45.91 34.94 (12.76,76.05)
Combined 11.91 14.83 18.14 (8.37,34.82)
CIGARETTE ONLY 61/2
1-19 14.16 6.85 10.51 (5.03,19.32)
20 14.07 7.89 15.54 (8.69,25.63)
21 + 33.67 41.38 37.53 (26.28,51.96)
Combined 21.24 14.97 19.61 (15.00,25.19)
By Level of Inhalation
PRIMARY & SECONDARY CIGAR 9/2
None 5.23 9.61 13.72 (4.42,32.02)
Slight 21.92 23.80 22.86 (2.57,82.53)
Moderate-deep 45.03 22.51 (0.29,125.26)
Combined 12.09 11.40 16.98 (7.31,33.45)
CIGARETTE ONLY 61/2
None, slight 12.83 9.29 11.06 (4.76,21.79)
Moderate 22.26 13.61 17.93 (12.56,24.83)
Deep 24.57 23.06 36.72 (21.75,58.03)
Combined 21.12 14.32 19.11 (14.65,24.50)
Table 16
Rate ratio of cancer of the salivary glands*
Age (years)
35-49 50-64 65-79 80+ Combined (95% CI) Deaths**
By Level of Cigars/Cigarettes per Day
CIGARETTE ONLY 14/11
1-19 3.90 1.36 1.33 (0.43, 3.11)
20 1.03 1.38 2.64 1.18 (0.43, 2.57)
21 + 3.92 0.36 (0.07, 1.04)
Combined 0.40 2.86 1.55 1.13 (0.62, 1.90)
By Level of Inhalation
CIGARETTE ONLY 15/11
None, slight 2.54 2.42 1.61 (0.52, 3.76)
Moderate 0.67 3.93 0.82 0.72 (0.31, 1.41)
Deep 1.71 0.88 0.47 (0.05, 1.71)
Combined 0.39 3.22 1.47 1.12 (0.62, 1.84)
*Based on data from CPS-I study. Age-standardized rate ratio fro smoking group compared to neversmokers.
**Number of deaths in subjet group.neversmoker group.
*Based on data from CPS-I study. Age-standardized rate ratio fro smoking group compared to neversmokers.
**Number of deaths in subjet group.neversmoker group.

129
Smoking and Tobacco Control Monograph No. 9
Table 17
Cancer of the larynx and cigar smoking : mortality ratios by type of smoking (males only)
Never- Mixed, Cigar
Studies Sample Size* Smoker Cigar & Cigarette Cigarette
Case-Control Odds Ratio (OR)
Burch (1981) 204/204 ever 2.9 6.1 (3.0-12.5)
Freudenheim (1992) 250/250 NS
Muscat (1992) 194/184 4.3* (1.7-16.4) 13.8 (2.3-27.1)
Prospective Rate Ratio (RR)
Kahn 293,000 1.0 10.33 9.95
CPS-I 442,455/15,072/7 1.0 10.02 (4.0-20.6) 19.09 (7.7-39.3) 19.68 (16.1-23.8)
* For prospective studies reviewed, the number of cigar smokers and number of deaths in this group are also given.
** Cigar and pipe combined

Chapter 4
130
The CPS-I results for laryngeal cancer are given in Tables 18 and 19. The
RRs for combined levels of cigars per day and combined levels of inhalation
are lower than for cigarette smokers, but the RRs for smokers of five or more
cigars per day, and the RRs for those cigar smokers reporting deep inhalation,
are markedly elevated. However, these rates are determined by small
numbers of cases in both the cigar smokers and neversmokers, and therefore
the confidence intervals on these rates are wide, though generally strongly
significant.
Summary The risk of laryngeal cancer is significantly elevated among cigar smokers,
approaching the RR for cigarette smokers for smokers of five or more cigars
per day or cigar smokers who inhale moderately or deeply. The data, while
limited by the number of deaths from laryngeal cancer, support a positive
relationship between number of cigars smoked per day and laryngeal cancer
risk. The data taken as a whole support cigar smoking as a cause of laryngeal
cancer.
CANCER OF The esophagus is exposed to the carcinogens from tobacco smoke
THE ESOPHAGUS which collect on the surface of the mouth and are swollowed
with saliva. It is also exposed to smoke which is deposited in the mucus
cleared from the lung and swallowed, as well as to systemically absorbed
carcinogens.
The Franceschi et al. study (1990), noted above, includes a case-control
comparison of 288 esophageal cancer cases. The 7 cigar and pipe smoker
cases produce an OR of 6.7 (2.3-19.8) compared to neversmokers; cigarette
smokers have an OR of 3.8 (2.2-6.6) in this study.
Tables 21 and 22 provide the rates of esophageal cancer for the cigar
smoking categories and cigarette-only smokers from the CPS-I data. The
rates are comparable across cigars and cigarettes, with a positive gradient for
numbers of cigars/cigarettes smoked each day. A step-wise Poisson regression
analysis confirmed a significant association of absolute rates of pharyngeal
cancers for primary cigar smokers with age (F=19.3, p<.0001), inhalation
(F=12.1, p=.001), and cigars per day (F=7.3, p=.01).
Summary The risk of esophageal cancer is several times higher among cigar smokers
than among neversmokers, with RR of occurrence similar to that for cigarette
smokers. A dose-response effect is confirmed with higher rates for cigar
smokers with higher numbers of cigars per day or with deeper inhalation.
The data establish cigar smoking as a cause of esophageal cancer.
BLADDER AND In a case-control study of 75 bladder cancer cases of both sexes
URINARY SYSTEM in northern New Jersey primarily focused on industrial chemical
CANCERS exposure, Najem et al. (1982) found a significant risk of bladder
cancer for individuals with a history of cigarette smoking with an OR of 2.0
(1.1-3.7) compared to neversmokers. They found no relationship between
cigar smoking and risk for bladder cancer.
In a Danish case-control study of bladder cancer cases of both sexes,
165 male and 47 female, matched to 165 male and 94 female randomly-

131
Smoking and Tobacco Control Monograph No. 9
Table 18
Rate ratio of cancer of the larynx by level of cigar/cigarettes per day*
Age (years)
Daily Use 35-49 50-64 65-79 80+ Combined (95% CI) Deaths**
PRIMARY CIGAR 7/4
1-2 6.64 6.45 (0.72,23.27)
3-4
5 + 21.08 28.22 26.03 (8.39,60.74)
Combined 6.76 10.75 10.02 (4.01,20.64)
CIGAR & CIGARETTE 7/4
1-19 19.89 15.48 12.71 (1.43,45.90)
20 24.00 20.28 16.14 (1.81,58.26)
21 + 94.58 32.53 39.91 (8.02,116.61)
Combined 33.72 21.31 19.09 (7.65,39.33)
CIGARETTE ONLY 105/4
1-19 12.24 7.66 8.70 (4.75,14.59)
20 29.36 27.58 25.69 (18.66,34.48)
21 + 43.58 25.38 23.59 (17.33,31.37)
Combined 30.65 19.34 19.68 (16.10,23.83)
Table 19
Rate ratio of cancer of the larynx by level of inhalation*
Age (years)
Level of Inhalation 35-49 50-64 65-79 80+ Combined (95% CI) Deaths**
PRIMARY CIGAR 7/4
None 8.70 9.53 10.60 (3.87,23.07)
Slight
Moderate-deep 106.52 53.26 (0.70,296.32)
Combined 6.84 10.99 10.32 (4.13,21.26)
CIGAR & CIGARETTE 7/4
None, slight 54.83 10.30 18.86 (5.07,48.28)
Moderate 22.38 5.59 (0.07,31.13)
Deep 161.85 80.93 (9.09,292.18)
combined 32.44 20.08 18.15 (7.27,37.40)
CICARETTE ONLY 107/4
None, slight 28.19 18.94 22.19 (14.74,32.07)
Moderate 27.88 13.03 13.49 (10.01,17.78)
Deep 30.59 39.79 27.54 (18.44,39.56)
Combined 29.21 19.57 19.36 (15.87,23.39)
*Based on data from CPS-I Study. Age-standardized rate ratio for smoking group compared to neversmokers.
**Number of deaths in subject group/neversmoker group.
*Based on data from CPS-I study. Age-standardized rate ratio fro smoking group compared to neversmokers.
**Number of deaths in subjet group.neversmoker group.

Chapter 4
132
Table 20
Esophageal cancer and cigar smoking: rate ratios by type of smoking (males only)
Rate Ratio
Never- Mixed, Cigar
Studies Sample Size* Smoker Cigar & Cigarette Cigarette
Case-Control
Sadowsky (1953) 104/615 4.8 3.3 3.8
Wynder (1957) 39/115 3.1 0.4 2.6
Pernu (1960) 202/713 5.9 2.7
Schwartz (1961) 249/249 8.6 11.7
Wynder & Bross (1961) 150/150 3.6 3.7 2.8
Martinez (1969) 120/360 2.0 2.2 1.5
Martinez (1970) 346/346 2.0 2.5 1.7
Franceschi (1990) 288/1,272 6.7** (2.3-19.8) 3.8 (2.2-6.6)
Prospective Rate Ratio (RR)
Hammond & Horn (1958) 187,783 1.0 5.00 5.06
Doll & Peto (1976) 41,000 1.0 3.70** 9.0 4.70
Hammond (1966) 440,559 1.0 3.97** 4.17
Kahn (1966) 293,000 1.0 5.33 6.17
CPS-I 442,455/15,072/20 1.0 3.60 (2.2-5.6) 3.57 (2.3-5.2) 3.966 (3.4-4.6)
* For prospective studies reviewed, the number of cigar smokers and number of deaths in this group are also given.
** Cigar and pipe combined.

133
Smoking and Tobacco Control Monograph No. 9
Table 21
Rate ratio of cancer of the esophagus by level of cigar/cigarettes per day*
Age (years)
Daily Use 35-49 50-64 65-79 80+ Combined (95% CI) Deaths**
PRIMARY CIGAR 19/30
1-2 1.86 2.62 2.28 (0.74, 5.33)
3-4 4.71 2.46 7.73 3.93 (1.43, 8.55)
5 + 2.34 7.19 5.19 (2.23,10.22)
Combined 2.80 3.94 4.72 3.60 (2.17, 5.62)
SECONDARY CIGAR 7/30
1-2 2.64 (0.03,14.67)
3-4 3.12 1.56 (0.02, 8.68)
5 + 10.44 4.99 5.63 (1.81,13.14)
Combined 3.73 2.70 3.52 (1.41, 7.25)
CIGARETTE ONLY 162/30
1-19 1.83 2.69 2.73 2.41 (1.61, 3.46)
20 1.03 4.47 5.24 4.30 (3.32, 5.48)
21 + 0.98 6.23 5.55 5.60 (4.35, 7.10)
Combined 1.18 4.67 4.44 1.80 3.96 (3.37, 4.62)
Table 22
Rate ratio of cancer of the esophagus by level of inhalation*
Age (years)
Level of Inhalation 35-49 50-64 65-79 80+ Combined (95% CI) Deaths*
PRIMARY CIGAR 19/30
None 2.59 4.27 2.93 3.40 (1.90, 5.61)
Slight 1.90 (0.02,10.58)
Moderate, deep 14.91 10.31 14.84 (2.98,43.37)
Combined 2.84 4.01 4.98 3.69 (2.22, 5.76)
SECONDARY CIGAR 7/30
None 4.29 2.69 4.15 (1.34, 9.68)
Slight 4.45 2.22 (0.03,12.37)
Moderate, deep 8.95 2.69 (0.04,14.94)
Combined 3.81 2.78 3.62 (1.45, 7.46)
CIGARETTE ONLY 170/30
None, slight 3.21 3.22 2.21 2.94 (1.97, 4.23)
Moderate 1.36 5.18 4.92 4.06 (3.30, 4.94)
Deep 1.30 4.86 5.18 4.95 (3.55, 6.72)
Combined 1.15 4.75 4.46 1.66 3.97 (3.39, 4.61)
*Based on data from CPS-I Study. Age-standardized rate ratio for smoking group compared to neversmokers.
**Number of deaths in subject group/neversmoker group.
*Based on data from CPS-I study. Age-standardized rate ratio fro smoking group compared to neversmokers.
**Number of deaths in subjet group.neversmoker group.

Chapter 4
134
Table 23
Bladder and urinary system cancer: mortality rate ratio by type of smoking (males only, except as noted)
Odds Ratio (OR)
Never- Mixed, Cigar
Sample Size* Smoker Cigar & Cigarettes Cigarette
Najem (1982) 75/142 ns 2.0 (1.1-3.7)
Mommsen (1983) male 165/165 2.3 (0.7-7.4) 3.5 (1.5-7.9)
Mommsen (1983) female 3.2 (1.3-7.7)
Morrison (1984) male 1435/1852 ns 1.9 (1.2-2.7)
Morrison (1984) female 2.4 (1.6-3.2)
Hartge (1985) 2982/5782 1.33 (.92-1.94) 3.36 (2.8-4.0)
Jensen (1987) 388/787 2.5 (0.2-28.4) 3.6 (2.2-5.8) 2.9 (1.8-4.8)
Slattery (1988 332/686 2.46 (1.01-5.95) 3.69 (2.58-5.26)
Burch (1989) 826/792 0.97 (.69-1.36) ever 2.65 (1.82-3.86)
Kunze (1992) 531/531 1.4 (0.9-2.4) 3.6 (2.4-5.4)
highest consumption category
Prospective Studies Rate Ratio (RR)
Kahn (1966) 293,000 1.0 0.94 2.15
CPS-I primary 442,455/15,072/26 1.0 1.38 (0.89-2.04) 2.48 (1.42-4.03) 3.17 (2.83-3.54)
CPS-I secondary 442,455/7,349/9 1.0 1.23 (0.56-2.33)
*For prospective studies reviewed, the number of cigar smokers and number of deaths in this group are also given.

135
Smoking and Tobacco Control Monograph No. 9
selected matched contols, Mommsen and Aagaard (1983) found significant
risk associated with current cigarette smoking, with OR's: male, 3.5 (1.5-7.9);
female, 3.2 (1.3-7.7). The reference group is not indicated, and may be
neversmokers or not-current-smokers of cigarettes. For cigars or cigarillos
only, an OR of 2.3 (0.7-7.4) is indicated for men, with insufficient data for
women. If previous and current smoking habits are both included, the OR
associated with cigar/cigarillo smoking becomes 1.4 (0.9-2.2) for men and
3.3 (1.3-8.5) for women; combining men and women results in a OR of
1.9 (1.3-2.8). The OR for women and combined sexes are significant,
but the OR for men is not significant.
Morrison et al. (1984) reported a large international case-control study
of 1,435 bladder cancer cases in Boston, Manchester UK, and Nagoya Japan,
with controls matched by sex and age in electoral registers. They found
significant risk associated with ever cigarette smoking across the three sites
with an OR approximately twice that for neversmokers, an OR of 1.9 (1.2-2.7)
for men and 2.4 (1.6-3.2) for women. There was a marked trend with number
of cigarettes per day. This study found no relationship between cigar
smoking and bladder cancer. Data for numbers of cigar smoking cases and
controls is not provided.
Hartge, Hoover and Kantor (1985) report on a large case-control study
of bladder cancer, with 2,972 patients and 5,782 controls, cases from
10 geographic areas of the US and controls randomly selected from the
general population weighted to age, sex, and geographic distribution of
cases. The focus of this study was risk related to pipes, cigars, and smokeless
tobacco. For primary cigar smokers (never smoked cigarettes) an OR of
1.33 (0.92-1.94) was calculated in comparison to neversmokers, adjusted for
race, age, and residence; for primary pipe smokers, an OR of 1.23 (0.75-2.00);
for smokers of pipes and cigars but no cigarettes, an OR of 1.40 (1.01-1.93).
In comparison, an OR of 3.36 (2.8-4.0) was observed for current cigarette
smokers. Further explorations among the primary cigar smokers regarding
level of inhalation, duration of cigar smoking, weekly consumption, and
lifetime dose are inconclusive, without trend and not significant.
Similarly, Jensen et al. (1987), reporting on a case-control study of
388 bladder cancer cases of both sexes in Copenhagen, Denmark, found no
significant relationship between cigar/cigarillo smoking and bladder cancer,
for ever cigar/cigarillo smokers, cigar/cigarillo only smokers, or by amount
of cigars/cigarillos smoked per day. An overall OR of 2.9 (1.8-4.8) was found
for cigarette-only smokers of both sexes combined.
Slattery et al. (1988) conducted a population based case-control study
of 332 white men compared to 686 controls selected by random digit dialing
and matched by age and sex; all were residents of Utah. This study focused
on the effect of cigarette smoking on the risk of bladder cancer associated
with coffee, tea, alcohol and other forms of tobacco. Strong associations
were found for cigarette smoking and bladder cancer, including positive
trends with duration of smoking, cigarettes per day, lifetime packs, and
inhalation, with an OR of about 4.0 for heavy users. These values were

Chapter 4
136
similar for both current and ex-smokers of cigarettes. For primary cigar
smokers who had never smoked cigarettes, an OR of 2.46 (1.01-5.95) was
calculated; whereas, for those cigar smokers who had ever smoked cigarettes,
an OR of 0.99 (0.61-1.60) was determined.
Burch et al. (1989) report a case-control study in Alberta and Ontario,
Canada between 1979 and 1982, comparing 826 cases and 792 neighborhood
controls matched for age and sex. They found significant associations for
cigarette smoking with an OR of 2.65 (1.82-3.86) for current cigarette smokers.
Gradients are reported with age first smoked, duration, cigarettes per day and
total pack years. The only cigar comparison reported is ever/never smoked
cigars, without stratifying by cigarette history; this comparison provides an
OR of 0.97 (0.69-1.36), with no trend indicated.
In a case-control study of 531 male and 144 female matched pairs in
Germany, Kunze et al. (1992) found smoking of cigars did not alter the risk
of bladder cancer. Controlling for cigarette smoking, the rates by lifetime
consumption of cigars shows positive trend, but the OR's are not significant.
The results of the tabulations for bladder cancer in the CPS-I data are
given in Tables 24 and 25, with tables by level of consumption and level of
Table 24
Rate ratio of cancer of the urinary bladder and urinary system, by level of
cigar/cigarettes per day*
Age (years)
Daily Use 35-49 50-64 65-79 80+ Combined (95% CI) Deaths**
PRIMARY CIGAR 25/102
1-2 1.29 0.79 0.78 (0.29, 1.71)
3-4 1.63 1.44 2.42 1.68 (0.77, 3.18)
5 + 2.75 1.42 3.32 2.03 (0.97, 3.73)
Combined 1.87 1.18 1.72 1.38 (0.89, 2.04)
SECONDARY CIGAR 9/102
1-2 4.79 0.65 1.02 (0.20, 2.97)
3-4 9.02 0.63 2.36 (0.76, 5.50)
5 + 0.52 0.32 (0.00, 1.80)
Combined 4.30 0.59 1.23 (0.56, 2.33)
CIGAR & CIGARETTE 16/102
1-19 0.77 4.00 1.42 (0.38, 3.65)
20 6.00 3.57 4.84 (2.41, 8.66)
21 + 1.75 1.10 (0.01, 6.10)
Combined 1.99 1.82 4.60 2.48 (1.42, 4.03)
CIGARETTE ONLY 318/102
1-19 2.98 1.97 3.11 2.35 (1.85, 2.94)
20 1.03 4.94 2.95 3.80 3.39 (2.82, 4.03)
21 + 3.94 5.46 3.72 4.63 4.16 (3.43, 4.99)
Combined 1.99 4.67 2.76 3.50 3.17 (2.83, 3.54)
*Based on data from CPS-I study. Age-standardized rate ratio for smoking group compared to neversmokers.
**Number of deaths in subject group/neversmoker group.
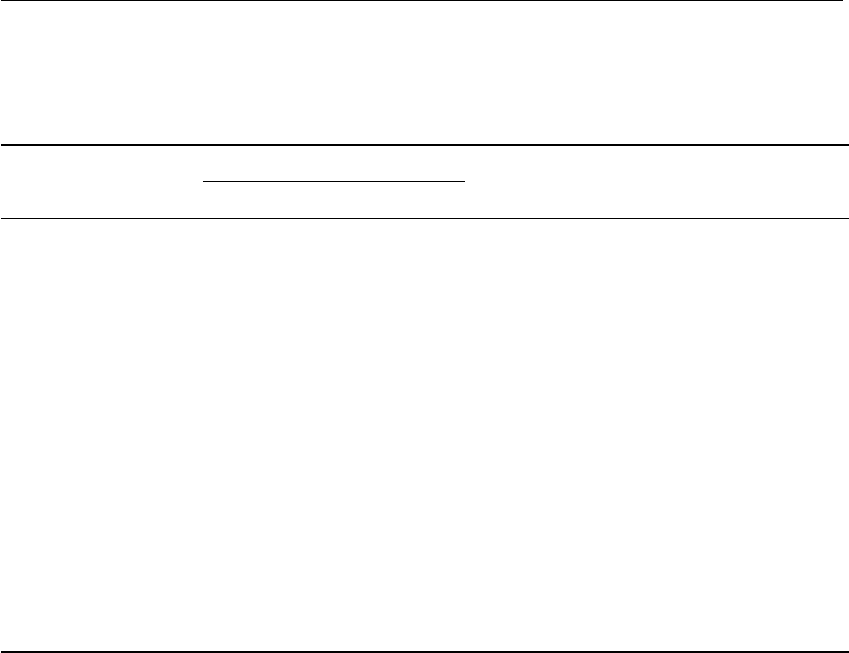
137
Smoking and Tobacco Control Monograph No. 9
Table 25
Rate ratio of cancer of the urinary bladder and urinary system, by level of inhalation*
Age (years)
Level of Inhalation 35-49 50-64 65-79 80+ Combined (95% CI) Deaths*
PRIMARY CIGAR 24/102
None 3.02 1.20 1.83 1.57 (1.00, 2.36)
Slight
Moderate-deep 2.42 1.52 (0.02, 8.44)
Combined 2.42 1.12 1.56 1.38 (0.88, 2.05)
SECONDARY CIGAR 9/102
None 2.97 0.63 0.77 (0.21, 1.98)
Slight 3.57 0.82 2.87 (0.58, 8.40)
Moderate-deep 11.41 1.45 (0.16, 5.25)
Combined 4.40 0.61 1.26 (0.58, 2.40)
CIGAR & CIGARETTE 17/102
None, slight 1.31 2.68 2.30 (1.15, 4.12)
Moderate 3.44 0.61 12.74 3.82 (1.23, 8.92)
Deep 4.58 (0.06,25.46)
Combined 1.91 1.73 5.49 2.62 (1.53, 4.20)
CIGARETTE ONLY 331/102
None, slight 6.08 3.17 2.14 3.00 2.51 (1.98, 3.15)
Moderate 1.35 4.49 2.73 5.02 3.48 (2.98, 4.03)
Deep 1.30 6.46 3.71 2.15 3.67 (2.92, 4.55)
Combined 1.93 4.74 2.68 3.70 3.17 (2.84, 3.53)
*Based on data from CPS-I study. Age-standardized rate ratio for smoking group compared to neversmokers.
**Number of deaths in subject group/neversmoker group.
inhalation respectively. Generally the age-adjusted rates calculated for cigars
are not significant. There is a positive trend with numbers of cigars for
primary cigar smokers, but no trend is seen with increasing depth of
inhalation. On the other hand, we do see significant rates and significant
trends for cigarette-only smokers, both cigarettes per day and inhalation
presenting a convincing pattern of increasing risk with increasing exposure.
Summary Although a few studies have indicated a significant relationship between
cigar smoking and bladder cancer, several other studies have not found
convincing evidence that smoking cigars increases the risk of bladder cancer.
PANCREATIC Farrow and Davis (1990) conducted a case-control study of 148 married
CANCER male pancreatic cancer cases from three counties in Washington state,
compared to 188 controls also married men, matched by age and selected
by a random digit dialing procedure. For current cigarette smokers, an OR
of 3.2 (1.8-5.7) was found, compared to neversmokers. Ever use of cigars
produced an OR of 0.7 with confidence interval that included 1.0. No data
are shown for primary cigar-only smokers.
Bueno de Mesquita et al. (1991) carried out a population-based case-
control study of 176 pancreatic cancer cases of both sexes matched to 487
controls from the Netherlands. For combined categories of cigarette smokers,

Chapter 4
138
Table 26
Pancreatic cancer and cigar smoking: rate ratios by type of smoking (males only, except as noted)
Odds Ratio (OR)
Never- Mixed, Cigar
Sample Size* Smoker Cigar & Cigarettes Cigarette
Case-Control Studies
Farrow (1990) 148/188 NS 3.2 (1.8-5.7)
Bueno de Mesquita (1991)
ever cigar 176/487 0.8 (0.5-1.3) 2.0 (1.2-3.1)
Muscat (1997) male 484/954 3.1 (1.4-6.9) 1.6 (1.1-2.4)
Muscat (1997) female 2.3 (1.4-3.5)
Prospective Studies Rate Ratio (RR)
Kahn (1966) 293,000 1.0 1.52 1.84
CPS-I primary 442,455/15,072/57 1.0 1.62 (1.22-2.11) 2.43 (1.72-3.34) 2.07(1.90-2.25)
CPS-I secondary 442,455/7,349/20 1.0 1.80 (1.10-2.78)
*For prospective studies reviewed, the number of cigar smokers and number of deaths in this group are also given.

139
Smoking and Tobacco Control Monograph No. 9
an OR of 1.96 (1.23-3.12) was found, compared to neversmokers. Ever use of
cigars by 36 subjects produced an OR of 0.8 (0.5-1.3), not providing any
evidence of increased risk.
Muscat et al. (1997) gathered case-control data on 484 male and female
pancreatic cancer cases and 954 non-tobacco related matched hospital
controls at several hospitals. Their results include for current male cigarette
smokers an OR of 1.6 (1.1-2.4) and current female cigarette smokers
2.3 (1.4-3.5), compared to same-sex neversmokers. Trend with increasing
consumption is shown, particularly for women. For male pipe/cigar smokers
an overall OR of 2.1 (1.2-3.8) was determined. For male cigar only smokers a
OR of 3.1 (1.4-6.9) was determined, compared to never and former cigarette
smokers combined. These cigar only smokers may include former cigarette
smokers, as well as lifetime cigar only smokers.
Tables 27 and 28 present the results of tabulation of pancreatic cancer
cases in the CPS-I data. Overall significance is shown for cigar-only and
secondary cigar smokers, as well as for cigarette smokers. For all groups,
positive trend is shown with numbers of cigars per day and levels of
inhalation. The levels of cigars/cigarettes per day in Table 27 and levels
of inhalation in Table 28 show values for cigar smokers similar to those
for cigarette smokers. A step-wise Poisson regression analysis confirmed
Table 27
Rate ratio of pancreatic cancer, by level of cigar/cigarettes per day*
Age (years)
Daily Use 35-49 50-64 65-79 80+ Combined (95% CI) Deaths**
PRIMARY CIGAR 56/198
1-2 1.52 0.78 1.79 1.18 (0.69, 1.89)
3-4 2.03 2.76 1.51 (0.86, 2.45)
5 + 2.71 2.72 2.21 (1.40, 3.32)
Combined 1.48 1.72 1.69 1.62 (1.22, 2.11)
SECONDARY CIGAR 20/198
1-2 0.51 0.56 (0.06, 2.01)
3-4 0.64 3.36 1.90 (0.82, 3.74)
5 + 1.56 2.12 12.23 3.71 (1.78, 6.83)
Combined 0.92 1.74 3.60 1.80 (1.10, 2.78)
CIGAR & CIGARETTE 38/198
1-19 10.71 1.79 3.02 2.74 2.67 (1.67, 4.04)
20 1.66 2.44 1.74 (0.83, 3.20)
21 + 2.13 3.35 2.35 (0.86, 5.12)
Combined 4.26 1.81 2.89 2.10 2.43 (1.72, 3.34)
CIGARETTE ONLY 549/198
1-19 3.75 1.85 1.77 1.07 1.69 (1.41, 2.00)
20 3.58 2.34 2.34 1.30 2.17 (1.89, 2.47)
21 + 3.95 2.39 2.67 1.59 2.41 (2.08, 2.77)
Combined 3.76 2.24 2.24 1.20 2.07 (1.90,2.25)
*Based on data from CPS-I study. Age-standardized rate ratio for smoking group compared to neversmokers.
**Number of deaths in subject group/neversmoker group.

Chapter 4
140
Table 28
Rate ratio of pancreatic cancer by level of inhalation*
Age (years)
Level of Inhalation 35-49 50-64 65-79 80+ Combined (95% CI) Deaths**
PRIMARY CIGAR 56/198
None 1.43 1.60 1.67 1.55 (1.12, 2.07)
Slight 2.05 2.45 2.16 (0.99, 4.10)
Moderate-deep 2.26 3.09 2.26 (0.45, 6.60)
Combined 1.59 1.76 1.60 1.66 (1.25, 2.16)
SECONDARY CIGAR 19/198
None 1.24 1.41 2.59 1.55 (0.80, 2.72)
Slight 1.86 1.92 (0.52, 4.92)
Moderate-deep 1.04 4.37 2.53 (0.51, 7.39)
Combined 0.94 1.79 2.80 1.69 (1.02, 2.64)
CIGAR & CIGARETTE 40/198
None, slight 10.55 1.73 3.14 2.64 2.69 (1.72, 4.00)
Moderate 1.80 1.72 1.42 (0.68, 2.62)
Deep 1.60 5.80 3.42 (1.25, 7.45)
Combined 4.11 1.74 2.95 1.88 2.40 (1.71, 3.27)
CIGARETTE ONLY 569/198
None, slight 2.41 2.14 0.95 1.99 (1.66, 2.36)
Moderate 3.71 2.16 2.24 1.01 2.01 (1.79, 2.25)
Deep 5.05 2.19 2.24 2.95 2.38 (1.98, 2.83)
Combined 3.66 2.22 2.25 1.19 2.06 (1.90, 2.24)
*Based on data from CPS-I study. Age-standardized rate ratio for smoking group compared to neversmokers.
**Number of deaths in subject group/neversmoker group.
a significant association of absolute rates of pancreatic cancers for primary
cigar smokers with age (F=32.1, p<10
-6
), inhalation (F=17.5, p<.0001), and
cigars per day (F=5.0, p=.03).
Summary Cigar smokers have higher rates of pancreatic cancer than nonsmokers,
particularly those who smoke higher number of cigars per day. Regression
analysis confirms significant relationships with the factors of age, inhalation,
and cigars per day for primary cigar smokers. These data suggest that cigar
smoking is a cause of pancreatic cancer.
CORONARY Matroos, Magnus and Strackee (1979) report a case-control study
HEART DISEASE conducted in the Netherlands comparing 397 cases of acute
myocardial infarction and 102 cases of fatal coronary attack, which taken
together are referred to as acute coronary events, to 891 neighborhood
controls matched by sex and age. Compared to noncurrent smokers
(neversmokers plus former smokers), cigar smokers as a group had an OR of
3.1 (2.0-5.1); the OR for cigarette smokers of 1 pack/day was 2.1 (1.5-2.8) and
for 2 packs/day was 2.0 (1.0-3.8), both lower than cigar smokers. The OR
of coronary events for cigar inhalers compared to non-current smokers was
3.4 (1.8-7.1); the OR for non-inhaling cigar smokers was 2.9 (1.8-5.2). For
cigar smokers, OR's for coronary events were not significantly different when

141
Smoking and Tobacco Control Monograph No. 9
Table 29
Coronary heart disease and cigar smoking: rate ratios by type of smoking (males only)
Odds Ratio (OR)
Never- Mixed, Cigar
Sample Size* Smoker Cigar & Cigarettes Cigarette
Case-Control Studies
Matroos (1979) coronary events 499/891 3.1 (2.0-5.1) 2.1 (1.5-2.8)
Kaufman (1987) MI, age 40-54 572/934
Primary cigar 1-4 cigars/day 0.9 (0.3-2.7)
Primary cigar 5+ cigars/day 1.7 (0.6-4.8)
Secondary cigar 1-4 cigars/day 1.5 (0.6-3.6)
Secondary cigar 5+ cigars/day 4.5 (2.2-9.2)
Prospective Rate Ratio (RR)
Hammond & Horn (1958) 187,783 1.0 1.28 1.70
Doll & Peto (1976) 41,000 1.0 1.03** 1.28 1.62
Best (1966) 78,000 1.0 0.99 1.60
Hammond (1966) age 45-54 440,559 1.0 1.15 2.81
Hammond (1966) age 55-64 1.35 1.84
Hammond (1966) age 65-74 0.93 1.45
Hammond (1966) age 75-84 1.10 1.24
Kahn (1966) 293,000 1.0 1.04 1.74
Gyntelberg (1981) first MI 5,212
Cigar Smokers 427 1.0 2.4 (1.4-3.8) 2.1 (1.7-2.7)
Cheroot 1,208 1.0 2.8 (2.1-3.6)
>6 Cheroots/day 315 1.0 4.2 (2.6-6.3)
Jajich (1984) elderly 2,674/265/32 1.0 1.67 (1.13-2.36) 1.94 (1.59-2.34)
Carstensen (1987) 25,129/1,256/42 1.0 1.16 (0.83-1.57) 1.48 (1.33-1.64)
Nyboe (1991) first MI 12,196 (see Table 30)
Ben-Shlomo (1994) secondary 19,018/658/42 1.0 0.91 (0.65-1.23) 1.74 (1.63-1.86)
Wald & Watt (1997) primary 21,520/1,309/33 1.0 0.98** (0.67-1.44) 2.27 (1.81-2.84)
Wald & Watt (1997) secondary 21,520/522/25 1.29** (0.88-1.99)
CPS-I primary 442,455/15,072/1527 1.0 1.05 (1.00-1.11) 1.29 (1.21-1.38) 1.54 (1.52-1.57)
CPS-I secondary 442,455/7,349/612 1.0 1.09 (1.01-1.18)
* For prospective studies reviewed, the number of cigar smokers and number of deaths in this group are also given.
** Cigar and pipe combined.

Chapter 4
142
hypertension was present or absent. An association between angina and
coronary events was not demonstrated for cigar smokers.
Kaufman et al. (1987) analyzed interview data in a case-control study of
572 men with non-fatal first myocardial infarction compared to 934 hospital
controls with non-tobacco related hospital admissions. Subjects and controls
were restricted to ages 40-54; both subjects and controls had to be either
never-cigarette smokers or to have stopped smoking cigarettes for at least
2 years. Thus a comparison was afforded between primary and secondary
pipe and cigars smokers. The estimated RR's of MI for subjects who had never
smoked cigarettes were elevated but not significant for smokers of 5 or more
cigars per day, pipe only, or cigars and pipe. For former cigarette smokers,
those who had smoked 5 or more cigars per day showed an elevated RR of
4.5 (2.2-9.2); the RR for those who had smoked fewer than 5 cigars or pipes
were slightly elevated but not significant.
In a prospective study of 5,249 Danish men followed for 7 years,
Gyntelberg et al. (1981) found the highest rates of myocardial infarction for
smokers of 6 or more cheroots/day (315 subjects), with a RR of 4.2 (2.6-6.3),
compared to neversmokers. Overall, cheroot smokers (1,208 subjects) had
a RR of 2.8 (2.1-3.6), all cigarette smokers (2,125 subjects) 2.1 (1.7-2.7), and
smokers of more than 10 cigarettes/day (875 subjects) 2.5 (1.2-5.2). A
multiple logistic regression analysis showed that cheroot smoking was a
significant factor for risk of MI. No information on previous smoking habits
was obtained, and smoking categories were allowed to overlap, so the cheroot
smokers would include both former and present cigarette and pipe smokers.
The authors also note that 75 percent of cheroot smokers indicate inhalation,
comparable to the rate of inhalation among cigarette smokers (74 percent).
The RR's presented do not appear to be age adjusted.
Jajich, Ostfeld and Freeman (1984) report on a prospective mortality
study of coronary heart disease in 2674 Chicago residents, aged 65 through
74, balanced for sex and black/white races drawn from a probability sample of
persons receiving old age assistance, followed for 4.5 years during 1965-1970.
Crude mortality ratios show a significant RR of 1.67 (1.13-2.36) for cigar/pipe
smokers in comparison to neversmokers, while current cigarette smokers had
a significant RR of 1.94 (1.59-2.34). However, when the analysis was adjusted
for other factors, cigar/pipe smoking was not significant, though current
cigarette smoking was significant.
In the Swedish prospective study (Carstensen 1987, see lung cancer) an
age-adjusted RR of 1.16 (0.83-1.57) for ischaemic heart disease is calculated
for cigar-only smokers compared to 1.48 (1.33-1.64) for cigarette smokers.
There is no trend for increased risk with increasing consumption of cigars,
given in grams/day. Though inhalation data was recorded, no analysis is
presented for cigar smokers. Categorization as cigar only smokers is made
by present behavior at the time of the initial survey questionaire, and may
include former cigarette and pipe smokers.

143
Smoking and Tobacco Control Monograph No. 9
Nyboe et al. (1991) studied the risk of first acute myocardial infarction
in a population-based prospective study of 12,196 Danish subjects of both
sexes, aged 30 or more. Their analysis finds highly significant effects related
to amount of tobacco per day and inhalation of smoke. There was no
statistically significant difference related to type of tobacco, whether plain
or filtered cigarettes, cigars/cheroots or pipes. They found no relationship
to duration of smoking in the past. Rates for former smokers were the same
as for neversmokers, and did not decrease with length of time since cessation
of smoking. The overall rates by grams/day (all tobacco) and inhalation are
reproduced in Table 30. The conversion rates used were 1 cigarette = 1 gm,
1 cheroot = 3 gm, 1 cigar = 5 gm, and pipe tobacco by weight. The RR's in
Table 30 are not stated to be age adjusted; the RR's for women are higher not
because absolute rates are higher, but because the rate for the comparison
neversmoker group is lower.
In the British prospective study discussed above (Ben-Shlomo et al., 1994,
see all-cause mortality) the secondary cigar smoker group (n=658) produced
an age-adusted RR for death from coronary heart disease of 0.91 (0.65-1.23)
when compared to neversmokers, while current cigarette smokers (n=7,921)
had a RR of 1.74 (1.63-1.86). Smoking categories are based on questions at
the beginning of the study, with no reclassification during the 18-years of
follow-up.
Wald and Watt (1997), in the follow-up study of 21,520 men discussed
previously, report a RR of ischaemic heart disease of 0.98 (0.67-1.44) for
primary cigar/pipe smokers and 1.29 (0.88-1.99) for secondary cigar/pipe
smokers who switched from cigarettes at least 20 years before the beginning
of the study, compared to a RR of 2.27 (1.81-2.84) for current cigarette
smokers. These rates are consistent with total tobacco consumption, levels
of inhalation, and carboxyhaemoglobin levels reported.
The tables for Coronary Heart Disease from the CPS-I data (Tables 31 and
32) show rate ratios compared to neversmokers by numbers of cigars/
Table 30
Estimated effect of tobacco smoking (all forms) on risk of acute myocardial
infarction among females and males*
RR of First Acute MI
Smoking group Females Males
Nonsmokers 1.0 1.0
Noninhalers 1.5 1.2
Inhalers
1-14 gm/day 3.6 1.6
15-29 gm/day 4.6 2.1
>30 gm/day 9.4 2.9
*Nyboe, 1991, p.444.

Chapter 4
144
Table 31
Rate ratio of coronary heart disease by level of cigar/cigarettes per day*
Age (years)
Daily Use 35-49 50-64 65-79 80+ Combined (95% CI) Deaths**
PRIMARY CIGAR 1,505/8,202
1-2 0.72 0.97 0.99 0.99 0.98 (0.91, 1.07)
3-4 2.08 1.09 1.05 1.02 1.06 (0.96, 1.16)
5 + 3.07 1.33 1.11 0.94 1.14 (1.03, 1.24)
Combined 1.77 1.12 1.04 0.99 1.05 (1.00, 1.11)
SECONDARY CIGAR 609/8,202
1-2 0.44 1.11 1.19 0.76 1.06 (0.92, 1.21)
3-4 1.67 1.22 1.24 0.68 1.10 (0.95, 1.27)
5 + 2.43 1.60 1.07 0.69 1.10 (0.96, 1.26)
Combined 1.46 1.32 1.17 0.72 1.09 (1.01, 1.18)
CIGAR & CIGARETTE 862/8,202
1-19 0.90 1.63 1.06 0.93 1.15 (1.04, 1.27)
20 4.02 2.15 1.31 1.08 1.47 (1.31, 1.64)
21 + 2.29 1.82 1.55 1.51 1.61 (1.36, 1.89)
Combined 2.34 1.84 1.19 0.98 1.29 (1.21, 1.38)
CIGARETTE ONLY 1,5659/8,202
1-19 3.10 1.80 1.36 1.08 1.40 (1.36, 1.45)
20 3.92 2.15 1.48 1.21 1.58 (1.54, 1.62)
21 + 4.58 2.28 1.53 1.22 1.65 (1.60, 1.69)
Combined 4.01 2.11 1.45 1.14 1.54 (1.52, 1.57)
*Based on data from CPS-I Study. Age-standardized rate ratio for smoking group compared to neversmokers.
**Number of deaths in subject group/neversmoker group.
cigarettes per day and by level of inhalation. The lowest levels of each table
for cigar smokers are not significantly different from neversmokers; however,
the rates for higher levels of cigars per day and moderate and deep inhalation
are significantly elevated.
The coronary heart disease data for primary cigar smokers from the CPS-I
study was subjected to a Poisson step-wise regression analysis in order to test
the association of the factors of chronological age, reported inhalation level,
and number of cigars per day. The independent variable tested was the
absolute rates of coronary heart disease mortality. The analysis produced the
following significant factors (Table 33): The level of inhalation is significant
in determining the rate of coronary disease. The square and square root
transformations of this arbitrary scale for inhalation were also tried, but in
this case the flat scale (0,1,2,3) fit best. The number of cigars per day was
also marginally significant, in this case the log transformation of the data fit
better than the flat scale of number of cigars.
Summary The studies of cigar smoking and coronary events present a pattern of
slightly elevated rates among cigar smokers who smoke heavily or inhale
deeply. The Danish study (Nyboe, 1991) and the CPS-I data provide evidence
of increasing rates with increasing numbers of cigars smoked each day; these

145
Smoking and Tobacco Control Monograph No. 9
Table 32
Rate ratio of coronary heart disease by level of inhalation*
Age (years)
Level of Inhalation 35-49 50-64 65-79 80+ Combined (95% CI) Deaths*
PRIMARY CIGAR 1461/8202
None 1.65 1.13 1.01 0.90 1.01 (0.96, 1.07)
Slight 2.79 1.10 1.13 1.51 1.23 (1.07, 1.41)
Moderate-deep 0.82 1.61 1.44 1.37 (1.07, 1.75)
Combined 1.79 1.11 1.04 0.99 1.05 (1.00, 1.11)
SECONDARY CIGAR 586/8,202
None 1.54 1.06 1.11 0.79 1.02 (0.92, 1.13)
Slight 0.69 1.55 1.23 0.47 1.10 (0.93, 1.30)
Moderate-deep 2.44 1.91 1.30 0.42 1.23 (0.99, 1.51)
Combined 1.49 1.31 1.15 0.69 1.08 (0.99, 1.17)
CIGAR & CIGARETTE 910/8,202
None, slight 1.42 1.42 1.03 1.05 1.12 (1.02, 1.24)
Moderate 3.57 2.12 1.43 0.74 1.43 (1.28, 1.58)
Deep 1.99 2.33 1.66 0.90 1.62 (1.37, 1.90)
Combined 2.37 1.83 1.20 0.97 1.29 (1.21, 1.38)
CIGARETTE ONLY 16,241/8,202
None, slight 3.46 1.94 1.40 1.06 1.45 (1.41, 1.50)
Moderate 3.88 2.03 1.43 1.17 1.52 (1.49, 1.55)
Deep 4.46 2.43 1.56 1.27 1.71 (1.66, 1.76)
Combined 4.00 2.11 1.44 1.13 1.53 (1.51, 1.56)
*Based on data from CPS-I Study. Age-standardized rate ratio for smoking group compared to neversmokers.
**Number of deaths in subject group/neversmoker group.
studies, plus those by Wald and Watt (1997) and Gyntelberg (1981), present
evidence for elevated rates for those inhaling cigar smoke. These data
establish that cigar smokers who smoke several cigars per day or who inhale
are at increased risk for coronary heart disease.
CHRONIC OBSTRUCTIVE Data from the prospective Cophenhagen City Heart Study
PULMONARY DISEASE (Lange 1992, see all-cause mortality) provides Chronic
(COPD) Obstructive Pulmonary Disease (COPD) rates for male and
female smokers of cigars and cheroots, with neversmokers as the comparison
group. Cheroots are commonly smoked by women as well as men in Denmark.
Table 33
Results of step-wise poisson regression of absolute rates of coronary heart disease deaths
Variable Coeffecient SE F-test Probability
(Constant) –0.05063 0.00269
Age (years) 0.09950 0.0000345 651.6 <10
–10
***
Inhalation (0-3) 0.2258 0.000397 20.8 0.00002***
Cigars per day 0.1443 0.000589 3.9 0.05*
***p<0.0001; **p<0.01; *p<.005.

Chapter 4
146
Table 34
COPD and cigar smoking: rate ratios by type of smoking (males only except as noted)
Never- Primary Mixed, cigar
Prospective Studies Sample size* Smoker Cigar & cigarette Cigarette
Hammond & Horn (1958) 187,783 1.0 1.29 2.85
Doll & Peto (1976) 41,000 1.0 9.33** 11.33 24.67
Best (1966) emphysema 78,000 1.0 3.33 5.85
bronchitis 78,000 1.0 3.57 11.42
Hammond (1966) emphysema 440,559 1.0 1.37** 6.55
Kahn (1966) 293,000 1.0 0.79 10.08
Lange (1992) male 6,511/808/4 1.0 3.7 (1.1-12) 6.4 (2.0-20) plain
Lange (1992) male 7.9 (2-3-27) filter
Lange (1992) female 7703/770/4 1.0 10 (2.3-48) 15 (3.1-65) plain
Lange (1992) female 16 (3.6-70) filter
Ben-Shlomo (1994) secondary 19,018/658/10 1.0 1.43 (0.68-2.63) 3.24 (2.86-3.65)
CPS-I primary 442,455/15,072/30 1.0 1.42 (1.0-2.0) 7.95 (6.1-10.2) 11.70 (11.1-12.3)
CPS-I secondary 442,455/7,349/33 1.0 4.39 (3.0-6.2)
*For prospective studies reviewed, the number of cigar smokers and number of deaths in this group are also given.
** cigar and pipe combined

147
Smoking and Tobacco Control Monograph No. 9
The overall RR for women cigar and cheroot smokers for mortality due to
COPD is 10 (2.3-48) and for men 3.7 (1.1-12). These rates are calculated to be
0.7 and 0.5 of the rate for cigarette smokers, both significantly lower.
However, when considering only those subjects reporting inhalation of
cigars/cheroots, the rate compared to smokers of cigarettes with inhalation is
2.1 times greater for women (0.8-5.3) and 0.9 (0.5-1.6) for men.
In the Whitehall prospective study (Ben-Shlomo, 1994), the secondary
cigar smoker group (n=658) produced an age-adusted RR for death from
COPD of 1.43 (0.68-2.63) when compared to neversmokers, while current
cigarette smokers (n=7,921) had a RR of 3.24 (2.86-3.65). Smoking categories
are based on questions at the beginning of the study, with no reclassification
during the 18 years of follow-up.
Tables 35 and 36 show the rate ratio for COPD for the various smoking
groups by numbers of cigars/cigarettes per day and by inhalation in the CPS-I
data. There is a positive gradient of rates with levels of inhalation across all
groups. The trend of increasing rates with increasing numbers of cigars/
cigarettes is less convincing, except for cigarettes where inhalation is usual.
The confidence intervals for rates of COPD for all primary cigar combinations
Table 35
Rate ratio of COPD by level of cigars/cigarettes per day*
Age (years)
Daily Use 35-49 50-64 65-79 80+ Combined (95% CI) Deaths**
PRIMARY CIGAR 30/119
1-2 1.61 1.84 1.39 (0.74, 2.38)
3-4 2.02 1.44 2.27 1.78 (0.89, 3.18)
5 + 1.00 1.16 1.03 (0.37, 2.23)
Combined 0.88 1.43 1.74 1.42 (0.96, 2.03)
SECONDARY CIGAR 33/119
1-2 1.48 3.19 2.64 (1.06, 5.44)
3-4 1.84 6.16 4.33 (2.07, 7.97)
5 + 8.96 5.03 8.39 6.68 (3.82,10.85)
Combined 4.25 4.79 3.71 4.39 (3.02, 6.16)
CIGAR & CIGARETTE 63/119
1-19 7.04 3.27 9.87 5.82 (3.77, 8.60)
20 12.12 10.39 16.50 12.44 (8.26,17.98)
21 + 9.01 9.76 6.84 (3.27,12.58)
Combined 8.92 6.09 10.83 7.95 (6.11,10.17)
CIGARETTE ONLY 1,376/119
1-19 6.89 9.71 8.32 8.86 (7.96, 9.84)
20 12.06 13.57 10.72 12.51 (11.48,13.60)
21 + 13.92 18.61 8.99 15.04 (13.73,16.45)
Combined 11.45 13.09 9.18 11.70 (11.09,12.34)
*Based on data fromCPS-I study. Age-standardized rate ratio for smoking group compared to neversmokers.
**Number of deaths in subject group/neversmoker group.
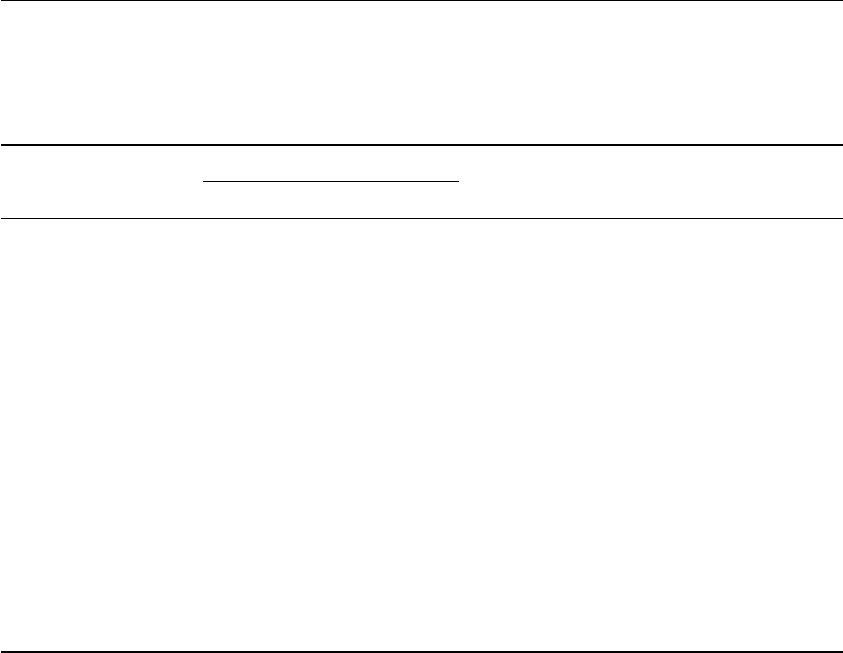
Chapter 4
148
Table 36
Rate ratio of COPD by level of inhalation.*
Age (years)
Level of Inhalation 35-49 50-64 65-79 80+ Combined (95% CI) Deaths**
PRIMARY CIGAR 27/119
None 1.00 1.94 1.09 (0.66, 1.70)
Slight 1.98 3.15 2.05 (0.66, 4.77)
Moderate-deep 6.39 6.31 4.52 (0.91,13.22)
Combined 0.61 1.38 1.65 1.32 (0.87, 1.92)
SECONDARY CIGAR 32/119
None 2.72 4.65 3.36 (1.96, 5.39)
Slight 2.21 4.46 17.14 7.68 (3.31,15.14)
Moderate-deep 11.51 7.07 5.84 (2.34,12.02)
Combined 3.79 4.93 3.84 4.42 (3.02, 6.24)
CIGAR & CIGARETTE 65/119
None, slight 4.05 4.22 6.78 4.92 (3.08, 7.45)
Moderate 13.34 7.89 8.99 9.17 (6.09,13.25)
Deep 12.77 9.26 41.19 19.00 (10.63,31.34)
Combined 8.96 6.06 9.69 7.61 (5.87, 9.70)
CIGARETTE ONLY 1,445/119
None, slight 8.17 9.10 8.46 8.80 (7.85, 9.85)
Moderate 11.52 13.69 10.00 12.28 (11.42,13.18)
Deep 14.41 19.51 10.62 16.07 (14.49,17.78)
Combined 11.56 13.06 9.29 11.74 (11.14,12.36)
*Based on data from CPS-I Study. Age-standardized rate ratio for smoking group compared to neversmokers.
**Number of deaths in subject group/neversmoker group.
include 1.0, so none of these rates are significantly different from the rate for
neversmokers, though the trend with inhalation is marked.
The CPS-I data was subjected to a step-wise Poisson analysis of variance
for each combination of factors in order to assess the association of the
various factors to the absolute rates of mortality caused by COPD. This
analysis yielded the following significant factors (Table 37): There is a
strongly significant effect related to age. The square of inhalation was a
stronger factor than inhalation or square root of inhalation, showing a
highly significant relationship to the rates of mortality. The analysis does
not show an effect related to numbers of cigars per day.
Summary The Lange study (1992) and the regression analysis of the CPS-I data
support the hypothesis that rates of COPD for cigar smokers who inhale are
significantly elevated. From the CPS-I analysis, the number of cigars smoked
daily is less significant in determining risk of COPD than the degree of
inhalation. The data taken as a whole support the conclusion that cigar
smoking can cause COPD in smokers who inhale deeply.
149
Smoking and Tobacco Control Monograph No. 9
Table 37
Results of step-wise poisson regression of absolute rates of COPD
Variable Coeffecient SE F-test Probability
(Constant) –9.6843 0.0226
Age (years) 0.1763 0.000291 46.5 <10
–8
***
Inhalation
2
(0-3) 0.7509 0.00117 39.4 <10
–7
***
Cigars per day — 0.2 0.89 NS
***p<0.0001; **p<0.01; *p<0.05.
CEREBRO-VASCULAR The Whitehall prospective study (Ben-Shlomo, 1994),
DISEASE (CVD) produced a RR of CVD of 1.00 (0.77-1.28) for the secondary
cigar smoker group, compared to neversmokers, while current cigarette
smokers had a RR of 1.74 (1.64-1.83).
In a prospective study of 7,735 British men followed for 12.75 years,
Wannamethee et al. (1995) found elevated rates of major stroke events (fatal
and non-fatal) in both primary pipe or cigar smokers and secondary smokers.
The age-adjusted RR for primary pipe or cigar smokers was 2.4 (0.8-7.6). For
secondary pipe or cigar smokers the RR was 3.2 (1.5-6.8). Both are similar to
the rates for light cigarette smokers 3.6 (1.8-6.9) (1-19 cigarettes per day). For
comparison, the cigarette-only smokers show a RR of stroke of 4.1 (2.2-7.4).
When the secondary pipe or cigar smokers are stratified into normotensive
and hypertensive groups, the RR for the normotensive group is 7.8 (2.1-30.0)
and for the hypertensive group 1.9 (0.7-5.2), compared to neversmokers in
the same normotensive/hypertensive group.
Haheim et al. (1996) report on risk of fatal stroke in the Oslo study,
analyzing data on 16,173 men followed for 18 years, beginning in 1972. In
their analysis, all smoking groups have significantly increased risk of stroke.
The RRs adjusted for age, diastolic blood pressure and blood glucose level
were 3.6 (1.05-12.3) for cigar/pipe only smokers; 6.7 (2.4-18.5) for cigarette-
only smokers; 9.8 (3.3-29.6) for smokers of cigarettes and pipe/cigar.
Smoking groups were divided according to smoking habits at the beginning
of the study, so the cigar/pipe group includes some proportion of secondary
smokers who formerly smoked cigarettes. No information is presented on
inhalation habits.
The results of the tabulations of CPS-I data for cigar smokers are given
in Tables 39 and 40. None of the cigar tables are convincing—neither the
RR's for primary cigar smokers by level of cigars per day nor the RR's by depth
of inhalation for primary cigar smokers are significant or show any trend,
though the results for cigarette-only smokers are significantly elevated.
Summary It is difficult to reconcile the results from the European studies and the
CPS-I results. The analyses for the Wannamethee (1995) and Haheim (1996)
studies present strong evidence that there is increasing stroke frequency
related to smoking cigars and pipes. These RRs are adjusted for age as well

Chapter 4
150
Table 38
Cerebrovascular disease and cigar smoking: rate ratios by type of smoking (males only)
Rate Ratio (RR)
Never- Mixed, Cigar
Prospective Studies Sample Size* Smoker Cigar & Cigarette Cigarette
Hammond & Horn (1958) 187783 1.0 1.31 1.30
Doll & Peto (1976) 41000 1.0 1.15* 1.21 1.34
Best (1966) 78000 1.0 1.28 0.88
Hammond (1966) 440559 1.0 1.09* 1.40 1.41
Kahn (1966) 293000 1.0 1.08 1.52
Ben-Shlomo (1994) secondary 19018/658/64 1.0 1.00 (0.77-1.28) 1.74 (1.64-1.83)
Wannamethee (1995) primary 7735/187/4 1.0 2.4*† (0.8-7.6) 4.1 (2.2-7.4)
Wannamethee (1995) secondary 7735/561/16 1.0 3.2*† (1.5-6.8)
Haheim (1996) 16173/1623/7 1.0 3.6* (1.05-12.3) 9.8* (3.3-29.6) 6.7 (2.4-18.5)
CPS-I, primary 442455/15072/435 1.0 0.96 (0.87-1.06) 1.12 (0.97-1.29) 1.24 (1.20-1.29)
CPS-I, secondary 442455/7349/134 1.0 0.92 (0.77-1.09)
* For prospective studies reviewed, the number of cigar smokers and number of deaths in this group are also given.
** Cigar and pipe combined
† Major stroke event—fatal or non-fatal

151
Smoking and Tobacco Control Monograph No. 9
Table 39
Rate ratio of cerebrovascular disease, by level of cigar/cigarettes per day*
Age (years)
Daily Use 35-49 50-64 65-79 80+ Combined (95% CI) Deaths**
PRIMARY CIGAR 431/2,556
1-2 1.87 1.24 1.02 0.95 1.01 (0.88, 1.17)
3-4 3.30 1.35 1.10 0.89 1.05 (0.88, 1.23)
5 + 0.74 0.81 0.79 0.79 (0.64, 0.97)
Combined 1.64 1.11 0.98 0.90 0.96 (0.87, 1.06)
SECONDARY CIGAR 133/2,556
1-2 1.46 0.93 0.88 0.95 (0.71, 1.26)
3-4 1.95 0.94 0.69 0.92 (0.67, 1.24)
5 + 3.42 1.06 0.93 0.79 0.89 (0.64, 1.22)
Combined 1.17 1.45 0.93 0.79 0.92 (0.77, 1.09)
CIGAR & CIGARETTE 190/2,556
1-19 2.14 1.76 1.15 0.62 0.99 (0.80, 1.20)
20 2.41 2.49 1.19 1.39 1.40 (1.08,1.79)
21 + 10.16 2.72 1.26 1.94 1.71 (1.16, 2.45)
Combined 4.32 2.19 1.15 0.82 1.12 (0.97, 1.29)
CIGARETTE ONLY 2,932/2,556
1-19 2.99 1.67 1.30 0.96 1.19 (1.12, 1.27)
20 3.16 2.03 1.26 0.97 1.22 (1.15, 1.29)
21 + 3.66 2.47 1.38 0.87 1.27 (1.19, 1.36)
Combined 3.32 2.11 1.31 0.95 1.24 (1.20, 1.29)
*Based on data from CPS-I study. Age-standardized rate ratio for smoking group compared to neversmokers.
**Number od deaths in subject group/neversmoker group.
as other factors such as diastolic blood pressure and body mass, whereas
the CPS-I results presented are only age-adjusted. The Haheim cigar data
is probably mixed primary and secondary cigar/pipe smokers. The CPS-I
primary cigar data are primarily individuals who report that they do not
inhale (78 percent), while inhalation information is not provided by the
other studies. If inhalation rates are much higher in the European studies,
this could explain some of the differences found in the RR of stroke between
the two groups of studies.
AORTIC Risk ratios of aortic aneurysm are shown to be elevated for both cigarette-
ANEURYSM only and cigar-only smokers by two prospective studies. The results for
the CPS-I data are given in Tables 42 and 43, by level of cigars/cigarettes per
day and by level of inhalation. Though the trend with increasing level for
cigar smokers is not clear, the overall result is highly significant: 1.76 (1.29-
2.35) for primary cigar smokers, 2.82 (1.91-4.00) for secondary cigar smokers,
3.32 (2.34-4.58) for cigar and cigarette smokers, and 4.96 (4.62-5.31) for
cigarette only smokers. The cigarette-only smokers do show a strong positive
trend both with increasing consumption of cigarettes per day and with
increasing levels of inhalation.

Chapter 4
152
Table 40
Rate ratio of cerebrovascular disease by level of inhalation
Age (years)
Level of Inhalation 35-49 50-64 65-79 80+ Combined (95% CI) Deaths*
PRIMARY CIGAR 410/2,556
None 1.13 0.86 0.95 0.88 0.91 (0.82, 1.02)
Slight 2.11 1.00 0.90 1.06 (0.79, 1.39)
Moderate-deep 13.98 1.69 1.08 1.16 1.22 (0.74, 1.91)
Combined 1.65 1.10 0.96 0.89 0.95 (0.86, 1.04)
SECONDARY CIGAR 132/2,556
None 0.81 1.09 0.84 0.95 (0.76, 1.18)
Slight 4.50 2.31 0.60 0.72 0.83 (0.55, 1.20)
Moderate-deep 2.86 0.80 0.54 0.88 (0.52, 1.38)
Combined 1.20 1.49 0.95 0.79 0.93 (0.78, 1.11)
CIGAR & CIGARETTE 202/2,556
None, slight 4.22 2.00 1.17 0.64 1.03 (0.85, 1.25)
Moderate 4.19 1.88 1.08 1.42 1.31 (1.01, 1.67)
Deep 3.54 3.58 1.22 0.86 1.30 (0.88, 1.86)
Combined 4.18 2.21 1.15 0.82 1.12 (0.97, 1.29)
CIGARETTE ONLY 3,083/2,556
None, slight 2.81 2.12 1.34 1.04 1.29 (1.21, 1.38)
Moderate 3.25 2.07 1.26 0.83 1.16 (1.10, 1.22)
Deep 3.66 2.25 1.35 1.08 1.33 (1.22, 1.43)
Combined 3.31 2.12 1.31 0.96 1.25 (1.20, 1.29)
Baed on data from CPS-I study. Age-standardized rate ratio for smoking group compared to neversmokers.
*Number od deaths in subject group/neversmoker group.
The step-wise Poisson analysis of absolute rates of mortality due to aortic
aneurysm of primary cigar smokers in the CPS-I study shows a significant
effect for the factors of age (F=66.1, p<10
-10
) and the square of inhalation
(F=45.3, p<10
-8
), but no significant effect for number of cigars per day (F=2.1,
p=.15). The moderate-deep inhalers for primary cigar do show an elevated
effect of RR=4.94 (1.59-11.52) in Table 43, a rate similar to the level for
cigarette-only smokers.
Summary The CPS-I study provides evidence that the risks of aortic aneurysm are
elevated for smokers, both for cigar smokers and cigarette smokers. Among
cigar smokers, the RR's for inhalers approach the risks observed for cigarette
smokers. The data from CPS-I support cigar smoking as a cause of aortic
aneurysm.

153
Smoking and Tobacco Control Monograph No. 9
Table 41
Aortic aneurysm and cigar smoking: rate ratios by type of smoking (males only)
Rate Ratio (RR)
Never- Mixed, Cigar
Prospective Stufies Sample Size* Smoker Cigar & Cigarette Cigarette
Kahn (1966) 293,000 1.0 2.06 5.24
CPS-I primary 442,455/15,072/46 1.0 1.76 (1.29-2.35) 3.32 (2.34-4.58) 4.96 (4.62-5.31)
CPS-I secondary 442,455/7,349/31 1.0 2.82 (1.91-4.00)
*For prospective studies reviewed, the number of cigar smokers and number of deaths in this group are also given.
Chapter 4
154
Table 42
Rate ratio of aortic aneurysm by level of cigar/cigarettes per day*
Age (years)
Daily Use 35-49 50-64 65-79 80+ Combined (95% CI) Deaths**
PRIMARY CIGAR 46/149
1-2 2.67 1.69 1.35 1.82 (1.11, 2.81)
3-4 0.96 1.57 0.88 (0.35, 1.82)
5 + 3.44 2.17 2.87 2.62 (1.58, 4.09)
Combined 2.17 1.61 1.76 1.76 (1.29, 2.35)
SECONDARY CIGAR 31/149
1-2 2.78 3.62 3.03 (1.51, 5.43)
3-4 4.60 3.39 2.80 (1.34, 5.16)
5 + 5.59 2.64 2.64 (1.26, 4.85)
Combined 4.31 3.14 2.82 (1.91, 4.00)
CIGAR & CIGARETTE 37/149
1-19 3.23 4.07 2.59 3.48 (2.13, 5.38)
20 2.24 3.49 2.32 (1.15, 4.14)
21 + 3.68 5.58 3.72 (1.36, 8.10)
Combined 2.97 4.17 1.99 3.32 (2.34, 4.58)
CIGARETTE ONLY 805/149
1-19 3.78 3.11 4.38 3.03 3.75 (3.25, 4.31)
20 7.11 4.23 6.15 3.94 5.17 (4.62, 5.77)
21 + 4.93 5.33 8.28 4.50 6.65 (5.90, 7.46)
Combined 5.54 4.36 5.92 3.49 4.96 (4.62, 5.31)
Table 43
Rate ratio of aortic aneurysm by level of inhalation
Age (years)
Level of Inhalation 35-49 50-64 65-79 80+ Combined (95% CI) Deaths*
PRIMARY CIGAR 45/149
None 2.06 1.59 1.78 1.73 (1.22, 2.39)
Slight 1.23 1.39 1.00 (0.20, 2.92)
Moderate-deep 7.93 4.02 4.94 (1.59,11.52)
Combined 2.20 1.65 1.68 1.77 (1.29, 2.37)
SECONDARY CIGAR 30/149
None 2.82 2.97 2.18 (1.22, 3.59)
Slight 8.00 3.28 3.52 (1.69, 6.47)
Moderate-deep 3.87 3.99 2.94 (0.95, 6.87)
Combined 4.41 3.23 2.67 (1.80, 3.82)
CIGAR & CIGARETTE 37/149
None, slight 2.57 2.15 2.49 2.32 (1.30, 3.82)
Moderate 3.08 6.71 4.17 (2.38, 6.77)
Deep 3.01 8.20 4.92 (1.80,10.72)
Combined 2.85 3.93 1.78 3.12 (2.20, 4.31)
CIGARETTE ONLY 827/149
None, slight 2.84 3.73 3.59 3.46 (2.94, 4.06)
Moderate 6.76 4.50 6.55 2.87 5.17 (4.71, 5.65)
Deep 5.19 4.83 8.17 4.88 6.57 (5.68, 7.55)
Combined 5.39 4.26 5.85 3.45 4.89 (4.56, 5.23)
Based on data from CPS-I study. Age-standardized rate raio for smoking group compared to neversmokers.
*Number of deaths in subject group/neversmoker group.
*Based on data from CPS-I study. Age-standardized rate raio for smoking group compared to neversmokers.
**Number of deaths in subject group/neversmoker group.

155
Smoking and Tobacco Control Monograph No. 9
CONCLUSIONS
1. Regular cigar smoking causes cancer of the lung, oral cavity, larynx,
esophagus, and probably cancer of the pancreas.
2. Heavy cigar smokers, and those who inhale deeply, are at increased risk
for coronary heart disease and can develop chronic obstructive
pulmonary disease (COPD). Data from CPS-I suggest that cigar smokers
have an increased risk for aortic aneurysm.
3. On average, cigar smokers are less likely to inhale cigar smoke than are
cigarette smokers to inhale cigarette smoke, and this reduced inhalation
of tobacco smoke probably explains the lower risks of coronary heart
disease, COPD, and lung cancer seen among cigar smokers compared to
cigarette smokers.
4. The risks of cancers of the oral cavity and esophagus are similar among
cigarette and cigar smokers, probably due to the similar doses of tobacco
smoke delivered to these areas by smoking cigars and cigarettes.
5. Former cigarette smokers who currently smoke cigars are more likely to
inhale deeply than cigar smokers who have never smoked cigarettes, and
their risks are intermediate between cigarette smokers and cigar smokers
who have never smoked cigarettes.
6. Cigarette smokers who switch to smoking only cigars have lung cancer
risks that are lower than continuing cigarette smokers, but these risks
appear to be substantially greater than those for individuals who have
quit smoking all tobbaco products.
REFERENCES
Abelin, T., Gsell, O.R. Relative risk of pulmonary
cancer in cigar and pipe smokers. Cancer
20:(8)1288-1296, 1967.
Ben-Shlomo, Y., Smith, G.D., Shipley, M.J., Marmot,
M.G. What determines mortality risk in male
former cigarette smokers? American Journal of Public
Health 84:1235-1242, 1994.
Benhamou, S., Benhamou, E., Flamant, R. Lung cancer
risk associated with cigar and pipe smoking. Cancer
37:825-829, 1986.
Best, E.W.R., McGregor, J.T. A Canadian study of
smoking and health. Ottawa, Department of National
Health and Welfare, 1966.
Blot, W.J., McLaughlin, J.K., Winn, D.M., Austin, D.F.,
Greenberg, R.S., Preston-Martin, S., Bernstein, L.,
Schoenberg, J.B., Stemhagen, A., Fraumeni, J.F., Jr.
Smoking and drinking in relation to oral and
pharyngeal cancer. Cancer Research 48:3282-3287,
1988.
Breslow, N.B., Day, N.E. Statistical Methods in Cancer
Research. The Analysis of Cohort Studies. Volume 1.
IARC Scientific Publication No. 32. International
Agency for Research on Cancer, 1980.
Breslow, N.B., Day, N.E. Statistical Methods in Cancer
Research. The Design and Analysis of Cohort Studies.
Volume 2. IARC Scientific Publication No. 82.
International Agency for Research on Cancer, 1987.
Broders, A.C. Squamous-cell epithelioma of the lip.
A study of five hundred and thirty-seven cases.
Journal of the American Medical Association
74:(10)656-664, 1920.
Bueno de Mesquita, H.B., Maisonneuve, P., Moerman,
C.J., Runia, S., Boyle, P. Life-time history of
smoking and exocrine carcinoma of the pancreas:
A Population-based Case-Control Study in the
Netherlands. International Journal of Cancer 49: 816-
822, 1991.
Burch, J.D., Howe, G.R., Miller, A.B., Semenciw, R.
Tobacco, alcohol, asbestos, and nickel in the
etiology of cancer of the larynx: A Case-Control
Study. Journal of the National Cancer Institute
67:(6)1219-1224, 1981.
Burch, J.D., Rohan, T.E., Howe, G.R., Risch, H.A., Hill,
G.B., Steele, R., Miller, A.B. Risk of bladder cancer
by source and type of tobacco exposure: A Case-
Control Study. International Journal of Cancer 44:622-
628, 1989.

Chapter 4
156
Carstensen, J.M., Pershagen, G., Eklund, G. Mortality
in relation to cigarette and pipe smoking: 16 years’
observation of 25000 Swedish men. Journal of
Epidemiology and Community Health 41:166-172,
1987.
Chow, W.H., McLaughlin, J.K., Hrubec, Z., Nam, J.M.,
Blot, W.J. Tobacco use and nasopharyngeal
carcinoma in a cohort of US veterans. International
Journal of Cancer 55:538-540, 1993.
Doll, R., Peto, R. Mortality in relation to smoking:
20 years’ observations on male British doctors.
British Medical Journal 2:(6051)1525-1536, 1976.
Ebenius, B. Cancer of the lip. A clinical study of 778
cases with particular regard to predisposing factors
and radium therapy. Acta Radiologica
24:(Supplement 48)1-232, 1943.
Farrow, D.C., Davis, S. Risk of pancreatic cancer in
relation to medical history and the use of tobacco,
alcohol and coffee. International Journal of Cancer
45:816-820, 1990.
Franceschi, S., Talamini, R., Barra, S., Baron, A.E.,
Negri, E., Bidoli, E., Serraino, D., La Vecchia, C.
Smoking and drinking in relation to cancers of the
oral cavity, pharynx, larynx, and esophagus in
northern Italy. Cancer Research 50:6502-6507, 1990.
Franceshci, S., Barra, S., La Vecchia, C., Bidoli, E.,
Negri, E., Talamini, R. Risk factors for cancer of the
tongue and the mouth: a case-control study from
northern Italy. Cancer 70:(9)2227-2233, 1992.
Freudenheim, J.L., Grahman, S., Byers, T.E., Marshall,
J.R., Haughey, B.P., Swanson, M.K., Wilkinson, G.
Diet, smoking, and alcohol in cancer of the larynx:
a case-control study. Nutrition and Cancer 17:33-45,
1992.
Garfinkel, L. Selection, follow-up, and analysis in the
American Cancer Society prospective studies.
National Cancer Institute Monograph 67 49-52, 1985.
Gyntelberg, F., Pedersen, P.B., Lauridsen, L., Schubell,
K. Smoking and risk of myocardial infarction in
Copenhagen men aged 40-59 with special reference
to cheroot smoking. Lancet 1:(8226)987-989, 1981.
Haheim, L.L., Holme, I., Hjermann, I., Leren, P.
Smoking habits and risk of fatal stroke: 18 years
follow up of the Oslo study. Journal of Epidemiology
and Community Health 50:621-624, 1996.
Hammond, E.C. Smoking in relation to the death rates
of one million men and women. In: Epidemiological
Approaches to the Study of Cancer and Other Chronic
Diseases, Haenszel, W. (Editor). National Cancer
Institute Monograph 19. National Institutes of
Health pp. 127-204, 1966.
Hammond, E.C., Horn, D. Smoking and death rates—
report on forty-four months of follow-up of 187,783
men. I. Total mortality. Journal of the American
Medical Association 166:(10) 1159-1172, 1958.
Hartge, P., Hoover, R., Kantor, A. Bladder cancer risk
and pipes, cigars and smokeless tobacco. Cancer
55:901-906, 1985.
Herling, S., Kozlowski, L.T. The importance of direct
questions about inhalation and daily intake in the
evaluation of pipe and cigar smokers. Preventive
Medicine 17:73-78, 1988.
Higgins, I.T.T., Mahan, C.M., Wynder, E.L. Lung
cancer among cigar and pipe smokers. Preventive
Medicine 17:116-128, 1988.
International Agency for Research on Cancer. Tobacco
Smoking. Monographs on the Evaluation of the
Carcinogenic Risk of Chemicals to Humans. Volume
38. IARC Scientific Publication No. 32., 1986.
Jajich, C.L., Ostfeld, A.M., Freeman, D.H., Jr. Smoking
and coronary heart disease mortality in the elderly.
Journal of the American Medical Association
252:(20)2831-2834, 1984.
Jensen, O.M., Wahrendorf, J., Blettner, M., Knudsen,
J.B., Sorensen, B.L. The Copenhagen case-control
study of bladder cancer: role of smoking in invasive
and non-invasive bladder tumours. Journal of
Epidemiology and Community Health 41:30-36, 1987.
Joly, O.G., Lubin, J.H., Caraballoso, M. Dark tobacco
and lung cancer in Cuba. Journal of the National
Cancer Institute 70:(6)1033-1039, 1983.
Kahn, J.A. The Dorn study of smoking and mortality
among U.S. veterans: report on eight and one-half
years of observation. In: Haenszel, W. (Editor).
Epidemiological Approaches to the Study of Cancer
and Other Chronic Diseases. National Cancer Institute
Monograph 19:1-125, 1966.
Kaufman, D.W., Palmer, J.R., Rosenberg, L., Shapiro, S.
Cigar and pipe smoking and myocardial infarction
in young men. British Medical Journal 294:1315-
1316, 1987.
Keller, A.Z. Cellular types, survival, race, nativity,
occupations, habits and associated diseases in the
pathogenesis of lip cancers. American Journal of
Epidemiology 91:(5)486-499, 1970.
Kunze, E., Chang-Claude, J., Frentzel-Beyme, R. Life
style and occupational risk factors for bladder
cancer in Germany. Cancer 69:(7)1776-1790, 1992.
Lange, P., Nyboe, J., Appleyard, M., Jensen, G.,
Schnohr, P. Relationship of the type of tobacco
and inhalation pattern to pulmonary and total
mortality. European Respiratory Journal 5:(9)
1111-1117, 1992.
Levin, M.L., Goldstein, H., Gerhardt, P.R. Cancer and
tobacco smoking. A preliminary report. Journal of
the American Medical Association 143:(4)336-338,
1950.
Lombard, H.L., Snegireff, L.S. An epidemiological
study of lung cancer. Cancer 12:(2)406-413, 1959.
Lubin, J.H., Richter, B.S., Blot, W.J. Lung cancer risk
with cigar and pipe use. Journal of the National
Cancer Institute 73:(2)377-381, 1984.
Martinez, I. Factors associated with cancer of the
esophagus, mouth and pharynx in Puerto Rico.
Journal of the National Cancer Institute 42:(6)1069-
1094, 1969.

157
Smoking and Tobacco Control Monograph No. 9
Martinez, I. Retrospective and prospective study of
carcinoma of the esophagus, mouth, and pharynx in
Puerto Rico. Boletin de la Asociacion Medica de Puerto
Rico 62:(6)170-178, 1970.
Matroos, A., Magnus, K., Strackee, J. Fatal and nonfatal
coronary attacks in relation to smoking in some
Dutch communities. American Journal of Epidemiology
109:(2)145-151, 1979.
Merletti, F., Boffetta, P., Ciccone, G., Mashberg, A.,
Terracini, B. Role of tobacco and alcoholic beverages
in the etiology of cancer of the oral cavity/
oropharynx in Torino, Italy. Cancer Research
49:4919-4924, 1989.
Mills, C.A., Porter, M.M. Tobacco smoking habits and
cancer of the mouth and respiratory system. Cancer
Research 10:539-542, 1950.
Mills, C.A., Porter, M.M. Tobacco smoking, motor
exhaust fumes, and general air pollution in relation
to lung cancer incidence. Cancer Research 17:(6)981-
990, 1957.
Mommsen, S., Aagaard, J. Tobacco as a risk factor in
bladder cancer. Carcinogenesis 4:(3)335-338, 1983.
Morrison, A.S., Buring, J.E., Verhoek, W.G., Aoki, K.,
Leck, I., Ohno, Y., Obata, K. An international study
of smoking and bladder cancer. Journal of Urology
131:(4)650-654, 1984.
Muscat, J.E., Stellman, S.D., Hoffmann, D., Wynder,
E.L. Smoking and pancreatic cancer in men and
women. Cancer Epidemiology, Biomarkers and
Prevention 6:15-19, 1997.
Muscat, J.E., Wynder, E.L. Tobacco, alcohol, asbestos,
and occupational risk factors for laryngeal cancer.
Cancer 69:(9)2244-2251, 1992.
Najem, G.R., Louria, D.B., Seebode, J.J., Thind, I.S.,
Prusakowski, J.M., Ambrose, R.B., Fernicola, A.R. Life
time occupation, smoking, caffeine, saccharine, hair
dyes and bladder carcinogenesis. International Journal
of Epidemiology 11:(3)212-217, 1982.
National Cancer Institute. Changes in Cigarette-Related
Disease Risks and Their Implication for Prevention and
Control. Smoking and Tobacco Control Monograph
8. NIH Publication No. 97-4213. National Institutes
of Health, 1997.
Nyboe, J., Jensen, G., Appleyard, M., Schnohr, P.
Smoking and the risk of first acute myocardial
infarction. American Heart Journal 122:(2)438-447,
1991.
Pernu, J. An Epidemiological study on cancer of the
digestive organs and respiratory system. A study
based on 7,078 cases. Annales Medicinae Internae
Fenniae 49:(Supplement 33) 1-117, 1960.
Randig, K. Untersuchungen zur aetiologie des
bronchialkarzinoms (Investigations on the aetiology
of bronchial carcinoma). Oeffentliche
Gesundheitsdienst 16:(9)305-313, 1954.
Rothman, K.J. Modern Epidemiology. Boston/Toronto:
Little, Brown and Company, 1986.
Sadowsky, D.A., Gilliam, A.G., Cornfield, J. The
statistical association between smoking and
carcinoma of the lung. Journal of the National
Cancer Institute 13:(5)1237-1258, 1953.
Sandler, D.P., Comstock, G.W., Helsing, K.J., Shore,
D.L. Deaths from all causes in non-smokers who
lived with smokers. American Journal of Public Health
79:(2)163-167, 1989.
Schrek, R., Baker, L.A., Ballard, G.P., Dolgoff, S.
Tobacco smoking as an etiologic factor in disease.
I. Cancer. Cancer Research 10:(1)49-58, 1950.
Schwartz, D., Flamant, R., Lellouch, J., Denoix, P.-F.
Results of a French survey on the role of tobacco,
particularly inhalation, in different cancer sites.
Journal of the National Cancer Institute 26:(5)1085-
1108, 1961.
Slattery, M.L., Schumacher, M.C., West, D.W.,
Robinson, L.M. Smoking and bladder cancer.
Cancer 61:402-408, 1988.
Spitz, M.R., Fueger, J.J., Goepfert, H., Hong, W.K.,
Newell, G.R. Squamous cell carcinoma of the upper
aerodigestive tract: a case comparison analysis.
Cancer 61:203-208, 1988.
Staszewski, J. Palenie a rak wargi, jamy ustnej,
migdalkow i krtani (Tobacco smoking and its
relation to cancer of the mouth, tonsils and larynx).
Nowotwory 10:(2)121-132, 1960.
U.S. Department of Health and Human Services. The
Health Consequences of Smoking. Report of the Surgeon
General. DHEW Publication No.(HSM) 73-8704,
1973.
U.S. Department of Health and Human Services.
Smoking and Health. Other Forms of Tobacco Use.
Chapter 13. Report of the Surgeon General. DHEW
Publication No.(PHS) 79-50066, 1979.
Wald, N.J., Watt, H.C. Prosepective study of effect
of switching from cigarettes to pipes or cigars on
mortality from three smoking related diseases.
British Medical Journal 314:1860-1863, 1997.
Wannamethe, S.G., Shaper, A.G., Whincup, P.H.,
Walker, M. Smoking cessation and the risk of stroke
in middle-aged men. Journal of the American Medical
Association 274:(2)155-160, 1995.
Wicken, A.J. Environmental and personal factors in
lung cancer and bronchitis mortality in
Northern Ireland, 1960-62. Research Paper 9. London.
Tobacco Research Council 84, 1966.
Wynder, E.L., Bross, I.J. A study of etiological factors in
cancer of the esophagus. Cancer 14:(2)389-413,1961.
Wynder, E.L., Cornfield, J. Cancer of the lung in
physicians. New England Journal of Medicine
248:(11)441-444, 1953.
Wynder, E.L., Graham, E.A. Tobacco smoking as a
possible etiologic factor in bronchiogenic carcinoma:
A Study of Six Hundred and Eighty-four Proved
Cases. Journal of the American Medical Association
143:(4)329-336, 1950.

Chapter 4
158
Wynder, E.L., Hultberg, S., Jacobsson, F., Bross, I.J.
Environmental factors in cancer of the upper
alimentary tract. A Swedish study with special
reference to Plummer-Vinson (Paterson-Kelly)
syndrome. Cancer 10:(3)470-487, 1957.
Wynder, E.L., Mabuchi, K., Beattie, E.J., Jr. The
epidemiology of lung cancer. Recent trends.
Journal of the American Medical Association
213:(13)2221-2228, 1970.

159
Smoking and Tobacco Control Monograph No. 9
Appendix: Methods Used
In Analyzing CPS-I data.
AGE Many tables are presented which provide mortality risk
STANDARDIZATION ratios (RR) comparing observed rates for a particular disease
for a smoking group to rates for neversmokers. In all these tables, age
standardization has been carried out (Rothman, 1986). The differences in the
age composition of different subject groups would affect these comparisons
if no standardization were applied. For example, in the CPS-I data the age
distribution of primary cigar smokers is somewhat older than that of
cigarette-only current smokers, because of changing patterns in uptake over
time, and perhaps because of effects of differential mortality (NCI, 1997). In
order to make the groups comparable, all CPS-I rates and ratios for combined
age groups have been standardized to the age profile of the neversmoker
group, because the neversmokers are used as the reference comparison group
in determining the risk ratio for the various smoking groups. The
neversmoker subject group was selected as the reference group in preference
to a USA Population standard because the population standard is skewed to
younger age groups, where smoker mortality is lower and data from this
study are sparse. Thus, using a USA population standard would make rates of
disease for smokers appear to be lower and increase variability. In each case
rates are calculated for 5-year age groups (... 55.0-59.99, 60.0-64.99, ...) and
are standardized by weighting the contribution of the 5-year aged group
according to the proportion of the neversmoker population in that age
group. All rates given are rates of primary cause of mortality, as specified
by the primary cause of death from the death certificate. Confidence
intervals are calculated using the methods described in Breslow and Day
(1980, p. 131; 1987, p. 69).
STEP-WISE To test for a significant association of the factors of numbers of cigars
POISSON per day, level of inhalation, and chronological age to rates of mortality
REGRESSION for a specific disease, the absolute rates for each combination of factors
were subjected to a step-wise regression analysis using Poisson regression
(Breslow and Day, 1987). The objective of the regression analyses was not to
propose a biological model or predict rates of mortality, but to assess the
relative significance of factors and combinations of factors.
The factors were grouped as follows:
cigars per day value used in analysis
1-2 cpd 2
3-4 cpd 4
5+ cpd 7
depth of inhalation value used in analysis
none 0
slightly 1
moderately 2
deeply 3

Chapter 4
160
chronological age value used in analysis
40-44.99 42.5
45-49.99 47.5
50-54.99 52.5
55-59.99 57.5
Age was advanced during the 12 years of follow-up, with the data
tabulated into cells of current combinations of values. If smoking behavior
changed at the time of follow-up interviews, subjects were reclassified or
deleted from subject groups appropriately. All cells with at least 20 person-
years-of-observation (PYO) were retained for the analyses. For the primary
cigar subjects, there were typically 60-70 cells of combinations of factors
which met the minimum criteria for inclusion. Some portion of these cells
had at least one death, and hence a positive rate estimate for the disease.
When no death had occured for a combination of factors, no rate estimate
was possible, but these cells were also included with a 0.0 rate used. All cells,
including those with no deaths, were included in the regression in order not
to overestimate rates.
Several transformations of each variable were included, in order to test
the significance of possible variations. For the variable age, both the flat
values and log(age) were tested. For cigars per day, both the flat values and
log(cpd) were tested. For depth of inhalation, the flat values, as well as the
square and square root transformations, were tested. All regressions were
weighted to the square root of the observed PYO for the cell, thereby
weighting each cell in proportion to the confidence attached to the estimate
provided by that cell.
Data preparation was done in SAS; tabulation into cells of factors,
calculation of rates and standardization was done in Pascal; statistical
analysis of data was done in S-Plus.

161
Smoking and Tobacco Control Monograph No. 9
Indoor Air Pollution From Cigar Smoke
James L. Repace, Wayne R. Ott, and Neil E. Klepeis
INTRODUCTION
Smoking in enclosed spaces exposes occupants to indoor air pollution
from the by-products of tobacco combustion in confined spaces where airborne
contaminant removal is slow and uneven. This chapter investigates the factors
determining the indoor environmental tobacco smoke exposure from cigar
smoking. Mathematical models allow the prediction of the levels of indoor
pollutants, such as environmental tobacco smoke (ETS).
The physical design of the cigar, leaf type and composition, and wrapper
type may all affect the cigar emissions (Schmeltz et al., 1976) (Chapter 3). For a
given composition, the mass of a cigar consumed during smoking is the primary
determinant of the quantity of its emissions. The greater mass of tobacco in
cigars relative to cigarettes leads to a prolonged smoking time and greater total
emissions when a single cigar is smoked compared to a single cigarette. An
alternate means of comparing emissions from cigars with those of cigarettes is to
compare the emission per minute or per gram of tobacco burned. Both the
emission rates and the number of minutes a tobacco product is smoked need to
be considered when comparing the contribution of cigars and cigarettes to ETS.
The emissions of cigars differ from those of cigarettes due to differences in
construction and engineering and differences in tobacco leaf (Chapter 3). The
number of puffs taken to smoke a large cigar is dependent on the size of the cigar
and may be as high as 100, whereas for a cigarette, it is approximately 10 (Rickert
et al., 1985).
MATHEMATICAL ETS concentrations of indoors can be predicted with reasonable
MODELS FOR CIGAR accuracy by application of a mass balance model (Leaderer, 1990).
ETS CONCENTRATIONS This model shows that the average concentration, Z
ave
, of ETS
pollutants in indoor air is directly proportional to the pollutant mass emission
rate and inversely proportional to the rate at which a unit volume of indoor air is
cleared of ETS (Ott et al., 1992; Leaderer, 1990; Repace, 1987a,b).
Ott et al.(1992) have shown that the time-averaged ETS concentration Z
ave
(in units of µg/m
3
), is given by:
Z
ave
= g
c
n
ave
/φν (1)
where g
c
is the cigar emission rate in units of µg/min, n
ave
is the average number
of cigars being smoked during the averaging time ∆T, where the generation
rate need not be uniform, i.e., the number of cigars being smoked at any instant
may vary. We define n
ave
= t
s
/∆T where t
s
is the total duration of smoking (Repace
et al., 1996). The quantity φ = qφ
v
is the effective air exchange rate in units of hr
-1
,
φ
v
is the air exchange rate due to ventilation alone, and v is the space volume in
units of m
3
. The term q is an empirically-derived factor (q > 1) expressing the
Chapter 5
162
increase in removal over ventilation alone due to such processes as surface
sorption of particulate matter (Repace, 1987). The estimation accuracy of this
equation improves as the correction term ∆Z/φ∆T becomes small compared to
Z
ave
, where ∆Z is the difference between the initial and final observed concentra-
tions (Ott et al., 1996).
For each individual cigar (Repace, 1987), the change over time of the ETS
pollutant concentration during smoking, assuming a uniform generation rate,
is given by Z(t), the concentration at time t where e is the base of natural
logarithms:
Z(t) = Z
eq
(1 - e
-
φt
) (2)
After a long time period, the pollutant concentration approaches an equilibrium
value Z
eq
, but most cigars typically are extinguished before reaching their
equilibrium value. The equilibrium value is a function of the emissions space
volume and ventilation rate and is defined by the equation.
Z
eq
= g
c
/φν (3)
Once smoking has ended, at a time t
s
, the concentration will decay as:
Z(t) = Z(t
s
) e
-
φ
(t - t
s
)
(4)
where Z(t
s
) is given by Equation 2 with t = t
s
. Equations 2 through 4 are
illustrated in Figure 1.
Equations 1 through 4 allow the results from field surveys and chamber
experiments to be generalized, estimating concentrations for pollutants from ETS
in a variety of indoor settings. These predictions require determination of the
values of n
ave
, g
c
, ν, and φ. It is possible to determine φ by experiment and to
measure or estimate ν, and to determine φ
v
from either measurement or estima-
tion from tables of ventilation rates (Repace, 1987). The emission factor, g
c
, must
be measured for the ETS constituent of interest.
CIGAR EMISSIONS: The chemical composition of cigar smoke is described elsewhere
MACHINE SMOKING in this monograph (Chapter 3).
Sidestream smoke is the major contributor to ETS for cigarettes (Adams et al.,
1987; Surgeon General (SG), 1986); there is little available data on the relative
amounts of sidestream and exhaled mainstream smoke for cigars. On a per-cigar
basis, large cigars deliver substantially higher amounts of carbon monoxide (CO)
and other sidestream gas-phase constituents than little cigars or cigarettes, and
substantially higher amounts of sidestream ammonia (Schmeltz, et al., 1976).
Armitage et al. (1978) collected the exhaled mainstream and sidestream smoke of
seven male habitual smokers of both little cigars and cigarettes and reported
that the sidestream nicotine emissions averaged 30.9 percent + 5.4 percent of
total cigar nicotine, while exhaled mainstream smoke averaged 12.7 percent + 9.0
percent. The cigar butt retained 20.1 percent + 8.8 percent, while the smoker
retained the remainder, in an amount similar to cigarette smoking.

163
Smoking and Tobacco Control Monograph No. 9
Figure 1.
Growth and decay of the concentration (in normalized units) of an ETS pollutant as a function of
time (in hours) as predicted by the mass balance model (solid line), respectively given by Equations 2
and 4 in the text. In this example, the air exchange rateφ = 0.84 hour
-1
, is equivalent to the ASHRAE
Standard for an office, and is slightly higher than the average closed window air exchange rate for a
home. Smoking begins at time
t
= 0, and ends at time
t
s
= 3 hours. The figure represents the concen-
tration from three cigars of 1 hour duration each smoked over a 3-hour period; the average number
of cigars smoked during the 3-hour period, is thus 1, from Equation 1. The concentration at the end
of the three hour smoking period is calculated by Equation 2 as
Z
(3) = 0.93
Z
eq
. The dashed curve
shows the concentration which would occur if smoking continued; after a long time, the equilibrium
concentration
Z
eq
, described by Equation 3 in the text, is approached. The actual decay of concen-
tration after smoking ceases is given by Equation 4.

Chapter 5
164
CIGAR EMISSIONS: Machine smoking in chambers under standard conditions can
HUMAN SMOKING provide a comparison of the relative emissions of various tobacco
products. However, in order to understand how differences among tobacco
products affect ETS concentrations, we must also measure emissions and
concentrations when cigars are smoked by human smokers who, unlike
machines, smoke idiosyncratically.
Emissions of RSP, CO, Repace and Lowrey (1982) measured Respirable Suspended
and Nicotine from Cigars Particles RSP (particles less than 3.5 microns in aerodynamic
diameter) and CO emissions of a popular-priced, mass-market cigar (Marsh-
Wheeling Stogie, length ≈5-1/2”, ring size ≈38, mass ≈7 g) smoked in a well-
mixed volume ν = 51 m
3
in a mechanically ventilated office building. The
logarithms of the RSP and CO concentrations plotted versus time show a straight-
line decay pattern from which the air exchange rate can be calculated (Figure 2).
The cigar was smoked by a regular cigar smoker for 20 minutes, yielding a
predicted equilibrium of Z
eq
= 830 µg/m
3
for RSP and 13.4 ppm (15,340 µg/m
3
)
for CO, calculated using Equation 3. The total calculated RSP emissions were
G
RSP
= 51m
3
x 830 µg/m
3
x 20 min / 16 min = 52.9 mg, and the RSP emission rate
was g
RSP
= G
RSP
/t
s
= 52.9 mg/20 min = 2.65 mg/min. For CO, the total emissions
were G
CO
= (51 m
3
x 15,340 µg/m
3
x 20 min) / 13.7 min = 1142 mg, using τ =1/φ
= 13.7 min (φ = 4.38 hr
-1
) yielding a CO emission rate of g
CO
= G
CO
/t
s
= 57.12 mg/
min. Neither the fraction of the cigar smoked nor the after-smoking weight was
recorded.
In 1978, by comparison, a single king-sized Marlboro was smoked by a
smoker for t
s
= 5.33 mins in a ν = 29 m
3
unventilated but well-mixed bedroom
with the windows and door closed (Repace and Lowrey, 1980). The value of Z
eq
=
1773 µg/m
3
for ETS-RSP was calculated using Equations 2 and 4, and the mean
residence time for the RSP was τ = 16.39 mins (R
2
= 0.80). Using Equation 3 (with
φ =1/τ ), the total RSP emissions were calculated to be G
RSP
= 29 m
3
x 1773 µg/m
3
x
5.33 min / 16.39 min = 16.72 mg per cigarette, and the RSP emission rate was g
RSP
= G
RSP
/t
s
= 3.14 mg/min. The cigarette RSP emission rate is actually higher than
the cigar, although the total RSP emissions of the cigar are much greater due to
the four-fold greater smoking duration and larger mass of tobacco in the cigar.
Leaderer and Hammond (1991) measured the emissions of 10 U.S. brands of
cigarettes and 1 cigar (a cigarillo -- B. Leaderer, personal communication, 1997)
as smoked by human smokers. From data presented in the paper, an estimated
total of 440 U.S. cigarettes and 40 cigars were smoked in this study. The average
smoking duration for the cigarettes was 7.5 mins; the average duration for the
cigars was not specified, but appears to be the same as for the cigarettes. The RSP
emissions of the 10 brands of cigarettes representing 48 percent of the sales-
weighted U.S. market in 1987, averaged G
RSP
/M
cig
= 27 + 3.4 mg/g, where an
average of M
cig
= 0.63 + 0.023 g of tobacco was smoked per cigarette. This results
in an emission rate of 2.27 mg of RSP per minute. The total average cigar emis-
sions were G
cigar
= 48 + 9.1 mg/g. The physical characteristics of the cigar were not
specified; however, a cigarillo typically contains less than 1.3 g of tobacco. The

165
Smoking and Tobacco Control Monograph No. 9
Figure 2.
Growth and decay of RSP and CO from a cigar smoked by a smoker in a mechanically ventilated 51
m
3
office at the U.S. Naval Research Laboratory’s main computer building in Washington D.C. in
1978. The effective air exchange rates of RSP and CO are similar (about 4 ach) due to the effect of
three mixing fans. By contrast, when the ventilation and mixing fans were not used, the effective air
exchange rate for RSP was 1 ach, and for CO, 0.43 ach (Repace and Lowrey, 1982).

Chapter 5
166
steady-state chamber nicotine concentration for the cigars was essentially the same
as for the cigarettes, whereas the RSP emissions were 28 percent higher for the
cigar.
Klepeis et al. (in press) report cigar smoking in two locations: a residence and
an office. These experiments consisted of the smoking of a cigar by a person in
both locations, and by a smoking machine in the latter. The effects on real-time
pollutant concentrations of various cigar durations, smoking styles, and ventilation
rates were measured.
In some of the experiments, two-minute average RSP concentrations were
measured with a TSI Model 8510 piezobalance. For one experiment, particle-bound
polycyclic aromatic hydrocarbon (PAH) concentrations were measured with an
EcoChem PAS 1002i Realtime PAH monitor (West Hills, CA).
The ventilatory air exchange rate was determined using Equation 4 by
observing the exponential decay of CO concentration after smoking had
stopped, thus including only the removal from air flow in and out of the room. In
contrast, the effective air exchange rate for RSP or PAH, which includes
mechanisms of RSP or PAH removal such as deposition and ventilation, was
measured by observing the exponential decay of RSP and PAH concentrations.
Together with the room volume and the observed pollutant time series, these decay
rates provided a means to calculate CO and RSP emission factors for each cigar.
In the residence, Klepeis et al. (in press) report results for a single cigar smoked
by a human smoker on two separate days in a 97 m
3
parlor. Measurements of the
particle size distribution showed that the bulk of the cigar aerosol mass was in the
particle-size range 0.1 to 2.5 µm. A regular cigar smoker smoked the cigar for 1 to 2
hours. Once the levels had declined to near background, a different smoker
smoked a cigarette for 9 minutes providing a comparison of the cigar and cigarette
emissions under the similar conditions (Figure 3).
The upper curves of Figure 3 show the real-time PAH concentrations of the
cigar and cigarette and the lower curves show the real-time RSP concentrations.
The mass balance model predicts the pollutant concentration time series with
reasonable accuracy (Figure 3, bottom) (Klepeis, et al., in press).
The ratio of CO to RSP concentrations is 1 ppm of CO per 165 µg/m
3
of RSP
for a Santona cigar smoked on day 1 (Table 1). The ratio of particulate PAH to RSP
concentrations is 1 µg/m
3
of particulate PAH per 238 µg/m
3
of RSP for a Paul
Garmirian cigar smoked on day 2. By contrast, for a Marlboro cigarette, the ratio is
1 µg/m
3
of particulate PAH per 137 µg/m
3
of RSP. However, the total PAH
emissions for the cigar are twice that of the cigarette due to the much longer
smoking duration and mass of the cigar.
In a field study of a 521 m
3
sports tavern, investigators machine-smoked four
Dutch Masters Corona Deluxe cigars in 11 minutes, two at a time. Figure 7 shows
the results for CO (Mage and Ott 1996, Ott et al. 1996). This experiment used the
decay of cigar CO to determine the ventilatory air exchange rate of the tavern,
φ
v
= 7.5 ach. Similarly, the decay rate of RSP (less background) yielded the effective
air exchange rate for cigar RSP, φ = 7.63 ach. They used three CO monitors and two

167
Smoking and Tobacco Control Monograph No. 9
Figure 3.
The time series, i.e., growth and decay of PAH and RSP concentration with time, measured in a
naturally ventilated San Francisco residence while a Paul Garmarian cigar and a Marlboro cigarette
were smoked sequentially by two different persons on March 9, 1997. The upper plot shows the
source activity pattern (rectangles) and the PAH data, while the bottom plot shows the simulta-
neously measured RSP data and the RSP time series predicted by the mass balance model (Klepeis et
al., in press).

Chapter 5
168
Figure 4.
Relative Emissions, Cigars versus Cigarettes: For each of the measured compounds, large cigars
produce greater total emissions than cigarettes. For CO, RSP, PAH, and Cadmium, the emissions
ratios are for ETS. For all others except benzene, they are for sidestream smoke. For benzene, they
are for mainstream smoke. (Brunnemann et al. 1977; Appel et al. 1990; Brunnemann, Stahnke, and
Hoffmann 1978; Brunnemann, Yu, and Hoffmann 1979; Brunnemann Adams and Hoffmann 1979;
Brunnemann and Hoffmann 1978; Klepeis et al. in press; Brunnemann and Hoffmann, 1975.)
169
Smoking and Tobacco Control Monograph No. 9
Table 1
CO, RSP, and Nicotine Emission Factors
1
Measured in Various Cigar and Cigarette Studies
Source
3
Ave Source
4
Total ETS
5
Mass ETS emissions
2
Experiment Description Duration Emission Rate Source Emissions Smoked per Mass Smoked
Klepeis et al. (in press)
1 Sante Fe Fairmont cigar 7.8 min 140 mg CO/min 1.1 g CO 6 g 190 mg CO/g
smoked by a machine in
49.6 m
3
office (4/6/96); 4.5 ach
1 Sante Fe Fairmont cigar 24 min 50 mg CO/min 1.2 g CO 6.1 g 200 mg CO/g
smoked by a machine in a
49.6 m
3
office (4/7/96); 0.12 ach
1 AyC Grenadiers cigar 10 min 87 mg CO/min 890 mg CO 4.9 g 180 mg CO/g
smoked by a machine in a
49.6 m
3
office (4/27/96); 0.12 ach
1 AyC Grenadiers cigar 11.5 min 67 mg CO/min 780 mg CO 4.9 g 160 mg CO/g
smoked by a machine in a
49.6 m
3
office (4/29/96); 4.5 ach
1 Santona cigar smoked by a person in 76 min 14 mg CO/min 1.1 g CO 8.8 g 130 mg CO/g
a 97 m
3
parlor of a (1.3 hrs) residence
(3/1/97); 2.0 ach; 2.5 eff ach for RSP
1.0 mg 78 mg RSP 8.9 mg RSP/g
RSP/min
1 Paul Garmirian cigar 90 min 0.95 mg RSP/min 86 mg RSP 10.8 g 8.0 mg RSP/g
smoked by a person in a (1.5 hrs)
97 m
3
parlor of a residence
(3/9/97); 0.9 ach; 1.2 eff ach 0.0042 mg 0.38 mg PAH 0.035 mg PAH/g
for RSP and 1.5 for PAH PAH/min
1 Marlboro cigarette smoked 7 min 1.9 mg RSP/min 16 mg RSP 0.4 g 40 mg RSP/g
by a person in a 97 m
3
parlor
of a residence (3/9/97); 1.3
eff ach for RSP and 2.0 for PAH
0.022 mg 0.18 mg PAH 0.45 mg PAH/g
PAH/min
Repace and Lowrey (1982) 20 min 57 mg CO/min 1.14g CO not
1 Marsh Wheeling Stogie
smoked by a person in a 51 recorded
m
3
office; 3.8 ach for RSP;
4.4 ach for CO (mechanical
ventilation). 2.7 mg RSP/min 53 mg RSP
Nelson (1994) 13.8 + 3.1 mg ETS
50 top brands of cigarettes RSP per cigarette
smoked by a person in an
unventilated room (analyzed by
Repace et al., in press) 1.8 + 0.28 mg
ETS nicotine per cigarette
Klepeis et al. (1996) 11.9 mg CO/min
Cigarette smoking in two
airport lounges 1.43 mg RSP/min
CPRT (1990) 10.3
+ 2.4 mg RSP/g
13 brands of cigars sold not not not not
in Canada
reported reported reported reported 0.13
+ 0.08 mg
nicotine/g
Mage and Ott (1996) 11 min SW, 240 mg SW, 1.2 g CO not
4 cigars smoked two at a time (all sources) CO/min per cigar recorded
by separate machines in a 521 m
3
tavern (8/24/94); 7.2 ach; results
are from two monitors, one in SW NW, 250 mg NW, 1.3 g CO
booth and one in NW booth CO/min per cigar
Notes:
1
Calculations of emission factors are based on a single-compartment mass balance model, which assumes uniform mixing.
2
Experi-
ment descriptions include the type of cigar or cigarette source, the location where smoking took place, the room volume, and the air exchange
rate and/or effective air exchange rate, which includes all removal mechanisms (both are in units of air changes per hour).
3
Ave Source
Emission Rate is the average emission rate over the time the source(s) was(were) on and over all the individual sources that were ever active.
4
Total Source Emissions is the total mass emitted over all sources.
5
Mass Smoked is the measured difference between the mass of the
unsmoked cigar(s) or cigarette(s) source and the mass after smoking.
6
Emissions per Mass Smoked is Total Source Emissions divided by
Mass Smoked. 1 ppm = 1.145 mg/m
3
at 25
o
C and 1 ATM.
Source: Because of the exceptional and multi-source nature of this composite table, the general reference for the “Experiment
description” column is: Klepeis et al. (in press). Specific references for horizontal data fields are noted in bold in the table.

Chapter 5
170
RSP monitors, in three locations: a central table, a Southwest corner booth and a
Northwest corner booth. The 30 minute average RSP concentration for the two
monitors was 194 µg/m
3
. The 30 minute average CO concentration for the three
locations was 1.7 ppm (Mage and Ott, 1996).
Emissions of particulate phase Available evidence suggests that cigar smoke contains
Polycyclic Aromatic Hydro- many of the same carcinogenic PAH’s that are found
carbons (PAH’s) from Cigars in cigarette smoke (SG,1979; IARC, 1986).
Real-time measurements of particle-bound PAH’s (4 or more ringed
compounds) are possible using a newly-developed photo-ionization monitor
(EcoChem, West Hills, CA). Investigators have applied this new monitor to make
real-time measurements of PAH aerosols from tobacco smoking and other sources
in homes, automobiles, and outdoor ambient conditions (Buckley and Ott, 1996;
Wilson et al., 1993; 1994; Ott et al., 1994).
Klepeis et al. (in press) used the EcoChem 1002i monitor in a 97 m
3
San
Francisco parlor with a human smoking a Paul Garmirian cigar. The cigar caused
the particle-bound PAH level to increase by as much as 2500 ng/m
3
above a near-
zero background concentration, while a Marlboro cigarette increased the levels by
1700 ng/m
3
above background. Using a calibration factor of 1000 ng/m
3
per pA,
they report that the total PAH emission for the cigar was 380 µg, while the
cigarette emitted 180 µg. The emission rate and the total emissions per gram (22
µg/min, and 450 µg/g respectively) were higher for the cigarette than for the
cigar (4.2 µg/min, and 35 µg/g respectively), but the cigar emitted twice as much
total PAH as the cigarette because of its longer smoking time. The PAH concen-
trations of both the cigar and the cigarette shown in the upper part of Figure 3
generally track the RSP emissions shown in the lower part of the figure.
Figure 4 presents the total emission of various smoke constituents for cigars
contrasted with that from cigarettes. For CO, RSP, PAH, and Cd, the emissions
ratios are for ETS. For all others except benzene, they are for sidestream smoke.
MEASUREMENTS AT Klepeis et al. (in press) report results from two field experiments in
CIGAR SMOKING which an investigator wearing a concealed CO personal monitor
SOCIALS attended public social events that featured cigar smoking. The
hidden miniaturized monitoring instrument was a Langan L15 Personal Exposure
Measurer™ equipped with a battery-powered data logger (Langan, 1992). The
monitor was carried in the inside pocket of a jacket. Measurements were logged
every minute in the first field study, and every 15 seconds in the second study.
The first cigar smoking social event, a “Cigar Smoker,” was held in a
private club in suburban San Francisco. Four different types of cigars were
available at the entrance. The private club was a large house with two adjoining
rooms (a large reception hall with a mezzanine and a food preparation area)
measuring 1560 ft
2
(155 m
2
) in total area, with a volume of 570 m
3
. The event’s
sponsors opened all doors and windows to allow maximum flow of outdoor air.
The investigator wearing the monitor smoked the first cigar only partially
and then mingled with the other guests. Because the monitor was carried for
several hours while traveling to and from the party, it is possible to compare the

171
Smoking and Tobacco Control Monograph No. 9
in-vehicle and outdoor CO concentrations with those measured during the cigar
smoker (Figure 5). As many as 89 persons were present (when 50 persons were
present, there were 12 women and 38 men). Indoor CO concentrations during
the smoker ranged between 5 and 11 ppm, yielding an indoor average of about 6
ppm. The highest CO concentrations occurred on the upstairs mezzanine of the
main hall. If we adjust the observed CO concentrations by subtracting the
ambient CO levels of 1.5 ppm measured outside the building on the sidewalks,
the cigar smokers contributed about 4.5 ppm. The CO levels were similar to
those measured during the rush-hour freeway drive to the event on Route 280,
which is a major arterial roadway between San Francisco and San Jose, California.
The high air exchange rate caused by the wide-open doors and windows prob-
ably reduced the interior CO concentrations considerably.
The second concealed monitoring field study (Klepeis et al., in press) took
place at a cigar banquet held in a downtown San Francisco restaurant. This cigar
banquet featured three premium cigars per person: [a Hoyo De Monterrey
Epicure #2, (5”, ring gauge 50) (Curtis, 1995) a Romeo Y Julieta Gold Label
Churchill (7”, ring gauge 47) (Curtis, 1995) and a Partagas Series “D” #4,
(Robusto, 4-7/8”, ring gauge 50) (Curtis, 1995, Resnick, 1996). Figure 6 shows the
CO concentration time series from the point when the investigator departs from
home in Redwood City, driving North on California Highway 101 to San Fran-
cisco. The CO averages about 4 ppm on this leg of the trip.
The CO concentration spikes to about 18 ppm in the confines of the parking
garage, whereas it is only 1 ppm on the street. The guests received the first cigar
when they entered the door, which was kept open during the entire social, and
they gathered around the bar to socialize for about an hour prior to being seated
for dinner. The indoor levels in the restaurant-bar during the first hour, due to
about 24 smokers at the bar (including the investigator) were 13 to 17 ppm
(Figure 6). At 7:45 PM the patrons were all seated for dinner at individual tables
of 4 to 6 persons. After everyone was seated, waiters distributed the second
imported cigar to all and began serving the three-course dinner. The investigator
was seated with five other persons; all six smoked cigars during dinner; the
investigator’s cigar was only partially smoked. The third cigar was distributed
just before dessert; the investigator did not smoke his. Overall, more than 100
cigars were smoked during this banquet; “laser lighters” rather than matches
were used to ignite the cigars.
The indoor CO concentration averaged over the 3-hour-and-20-minute
event was 10 ppm, and about 75 percent of the 40 persons present were smoking
cigars at any instant of time. Based on measurements outdoors on downtown
sidewalks before and after the event, ambient CO concentrations were found to
be about 1 ppm, so the indoor CO concentration caused by cigar smoking was
about 9 ppm. If the cigar dinner had lasted more than 8 hours, then indoor CO
concentrations would have violated the National Ambient Air Quality Standard
(NAAQS) adopted by the Environmental Protection Agency (EPA) to protect
public health (9 ppm CO for 8 hours).

Chapter 5
172
Figure 5.
The carbon monoxide (CO) personal concentration time series measured before, during and after attendance at a “cigar party” in the San
Francisco Bay Area on January 1, 1997. The total volume of the establishment was about 570 m . At one point in the evening 89 persons
were present of whom about two thirds were estimated to be smoking cigars. Notice that the background CO levels outdoors are be-
tween 1 and 2 ppm, and that the average CO concentration while driving from San Jose to the party (5.5 ppm; 5:00 PM - 6:20 PM) is
similar to the average concentration while present at the party (5.8 ppm; 6:26 PM - 8:09 PM) (Klepeis et al. In press).

173
Smoking and Tobacco Control Monograph No. 9
Figure 6.
CO concentrations measured using a concealed personal exposure monitor at a cigar dinner party in downtown San Francisco. The
investigator carried the Langan L15 CO Personal Exposure Measurer concealed beneath his dinner jacket. Concentrations were logged
every 15 seconds, and the background value (concentration that would occur in the absence of indoor sources) was estimated as 1 ppm
(Klepeis et al. In press).

Chapter 5
174
Figure 7(b).
RSP concentration time series measured in a 548 m3 tavern at three locations after investigators
machine-smoked four cigars in the central area (Ott, Switzer, and Robinson, 1996). The RSP
concentration (PM
3.5
) was measured with two piezobalances in the middle of the room and at the
southwest corner booth. Figures 7 (a) and 7(b) suggest that when averaged over a length of time
long compared to the source duration, it doesn’t matter where you are in the tavern, illustrating both
the validity of the well-mixed assumption for the mass-balance model and the futility of spatial
separation of smokers and nonsmokers as a putative public health measure.
Figure 7(a).
CO concentration time series measured in a 548 m3 tavern at three locations after investigators
machine-smoked four cigars in the central area. The air exchange rate was 7.5 air changes per hour.
Despite the wide separation of the three monitors (approx. 6 - 7 m) the simultaneous CO exposures
at all three locations are nearly within + 10 percent of the overall average concentration (1.84 ppm),
which is used by ASTM (ASTM E 741) as a criterion for uniformity of mixing (Mage and Ott, 1996).

175
Smoking and Tobacco Control Monograph No. 9
CO concentrations recorded on the freeway while driving to and from this
cigar banquet averaged 4.5 ppm, similar to values observed on the freeway while
driving to the earlier cigar smoker social. This observation is the same as the
average in-traffic CO concentration measured on 96 trips on a year-long study of
an urban arterial highway in the San Francisco Bay Area (Ott et al., 1996). After
leaving the restaurant, the investigator walked to a San Francisco bar where
several cigarettes were being smoked but no cigars; indoor CO levels were about
4.5 ppm, much lower than at the cigar dinner.
These studies show that cigar smoking can considerably elevate indoor CO
concentrations in a restaurant, even when the doors are wide open, and the
ventilation system is operating.
DISCUSSION Klepeis et al. (in press) report that the average emission rate and total
emissions per source are not good emission factors for use in comparisons
between different cigars and/or other tobacco sources, because they depend on
smoking style, smoking duration, or the mass of the cigar smoked. Emission per
mass smoked is a better basis for use in comparisons of cigar potencies, since it
provides a normalized measure of the ability of a tobacco source to produce ETS-
pollutant concentrations. Klepeis et al. (in press) report that CO emissions per
mass smoked (Table 1) ranged from 130 mg CO/g to 200 mg CO/g for three
different brands of cigars and two different smoking styles (i.e., by a machine and
by a person) in five settings. Two different Santa Fe Fairmont cigars smoked by a
machine gave CO emissions per mass smoked that were very similar (190 and
200 mg/g). The AyC Grenadiers cigars emitted CO in amounts of 160 and 180
mg/g when smoked by a machine. A Santona cigar smoked in a residential parlor
generated CO mass emissions that were somewhat smaller (130 mg/g), which
might be due to either the different smoking style or the different cigar brand
(Table 1).
RSP emissions per mass smoked for two cigar experiments in a residential
parlor were 8.0 and 8.9 mg RSP/g (Klepeis et al., in press). These RSP emission
factors are comparable to the results found for the 13 brands of medium and
large cigars smoked in a Canadian Report (CPRT, 1990) described above, which
averaged 10.3 + 2.39 mg RSP/g. By contrast, the RSP emissions per mass smoked
for a cigarette in the same residence was 40 mg/g, which is five times larger than
the emissions per mass smoked for the cigar.
Emissions of PAH per mass smoked were calculated for both the cigar and the
cigarette in the second residential experiment of Klepeis et al.(in press) from
Figure 3. Although the errors in estimation of the PAH background levels intro-
duce additional uncertainty (about 20 to 30 percent error), cigarettes appear to
generate more PAH than cigars (PAH emissions of 0.45 versus 0.035 mg/g).
Cigars appear to emit less RSP and PAH per mass burned than cigarettes, but
cigars contain more tobacco than cigarettes and also tend to be smoked for much
longer time periods (10 minutes or less for a cigarette versus an hour or more for
cigars).

Chapter 5
176
The Effects of Cigar Using the mathematical models presented earlier, the concentration
Smoking On Indoor of ETS in an enclosed space will be directly proportional to the
Air Pollution smoker density (g
c
n
ave
/ν) and inversely proportional to the effective
air exchange rate φ. The effective air exchange rate for nonreactive gases is the
same as the air exchange rate due to building ventilation plus infiltration, and for
particles may be somewhat higher due to surface sorption or air cleaning (Repace,
1987).
Ventilation rates for mechanically ventilated buildings are recommended by
the American Society of Heating, Refrigerating and Air Conditioning Engineers
(ASHRAE, 1990) and are typically incorporated into local building codes. In
buildings without ventilation systems, closed-window air exchange rates are
determined by the tightness of the building structure, and open-window
ventilation rates may be comparable to or higher than in mechanically ventilated
buildings. Typical closed-window residential air exchange rates are of the order
of 0.75 ach. Typical mechanical air exchange rates designed for commercial
buildings are a function of the density of human occupancy, and range from 0.84
air changes per hour (ach) for office buildings to 7 ach for restaurants.
If the ventilation rate φ
v
is determined by the building structure and
condition and the building volume is fixed, the concentration of ETS in a
building will be determined by the number of smokers, their smoking rate, and
the emission rate of the tobacco product.
The concentrations of certain ETS constituents can be compared to the National
Ambient Air Quality Standards (NAAQS) for regulated outdoor air pollutants. The
NAAQS for particulate matter <10 µm (PM
10
) is 50 µg/m
3
on an annual basis, and on
a 24-hour basis, 150 µg/m
3
, with one exceedance allowed per year. Recently the U.S.
EPA adopted a new fine particle standard. This proposed EPA NAAQS for PM
2.5
,
(particle size < 2.5 µm) is 15 µg/m
3
averaged on an annual basis, or 65 µg/m
3
on a
24-hr average basis with one allowed violation (i.e., no more than one day at each
monitor in a location may exceed the specified daily standard concentration).
The RSP level from a single Paul Garmirian cigar smoked in a San Francisco
residence (Klepeis et al., in press) averaged 160 µg/m
3
over a 4.7- hour period (Table
1), or 31 µg/m
3
averaged over a 24-hour period. By comparison, the Marlboro
cigarette smoked in the same San Francisco residence averaged 65 µg/m
3
over a
period of 2.75 hours, or 7 µg/m
3
averaged over 24- hour period.
The current NAAQS for carbon monoxide is 9 ppm, an 8 hour time-weighted
average (TWA)(USEPA, 1996). The average CO concentration measured during
the cigar party (5.8 ppm) (Figure 3) is slightly greater than encountered on a
California freeway (5.5 ppm), despite the fact that all the doors and windows
were open.
On a per-cigarette basis, Ott et al. 1992, Rosanno and Owens 1969, and
Rickert et al. 1984 report total CO emissions ranging from 40 to 70 mg per
cigarette for sidestream smoke. On a rate basis, Ott et al. (1992) report an average
CO emission rate of 9.4 mg CO/min for cigarettes, which is much lower than the
14 to 140 mg /min emission rates that Klepeis et al. (in press) found for cigars.

177
Smoking and Tobacco Control Monograph No. 9
On a mass basis, Klepeis et al. (in press) report that CO emissions for cigars are
between 100 and 200 mg/g (Table 1). If the mass of a cigarette smoked is about
0.4 g, as it was for one of the experiments of Klepeis et al. (in press), then the
cigarette CO emissions per mass smoked would also be in the range of 100 to 175
mg /g. However, the larger total mass of a cigar results in the total CO emissions
of cigars studied by Repace and Lowrey (1982) and Klepeis et al. (in press) (Table
1) averaging more than 1000 mg/cigar, placing the total cigar CO emissions
about 1000/50 = 20 times that of a cigarette.
The cigar RSP emissions reported by Klepeis et al. (in press) and Repace and
Lowrey (1982) for 3 cigars averaged about 77 mg per cigar. By contrast, (Table 1)
data from Nelson (1994) as analyzed by Repace et al. (in press) show ETS-RSP
emissions of about 14 + 3 mg/cig for the top 50 brands of cigarettes; an RSP
datum, 16 mg/cig reported by Klepeis et al.(in press) for a single Marlboro is
consistent with these results. This suggests that total RSP emissions of large
cigars are 5 to 6 times greater than cigarettes.
From the limited data available (Table 1) it appears that the total PAH
emissions of a large Paul Garmirian cigar (380 µg) is only twice that of a Marlboro
cigarette (180 µg) because the PAH emission rate for the Marlboro was 5 times as
large as for the cigar. The total PAH emissions for the cigar, however, were twice
as great as the cigarette because of the more than ten-fold larger smoking time for
the cigar. (Table 1 and Figure 2).
Cigar size and the extended smoking time compensate for the cigar’s lower
emission rate for RSP and PAH and enhance the delivery of CO to the indoor
environment. Smoking a single cigar can result in a much higher exposure of
nonsmokers to CO, RSP, and PAH than smoking a single cigarette.
CONCLUSIONS
1. ETS from cigar smoke is a major and increasing source of exposure to indoor
air pollution.
2. When smoked in confined indoor spaces at typical smoking and ventilation
rates, cigars may produce concentrations of certain regulated ambient air
pollutants, including CO and RSP, which can violate federal air quality
standards and add to the level of these compounds already in the ambient air
from other combustion sources.
3. Measurements of the CO concentrations at a cigar party in a hall and at a
cigar banquet in a restaurant showed carbon monoxide levels comparable to
those observed on a crowded California freeway.
4. The smoking of one cigar generates more Respirable Suspended Particles
(RSP) and Polycyclic Aromatic Hydrocarbons (PAH) than the smoking of one
cigarette due to the larger mass of tobacco contained in a cigar, but the
amount of PAH and RSP generated per gram of tobacco burned appears to be
somewhat lower for cigars compared to cigarettes.

Chapter 5
178
Adams, J.D., O’Mara-Adams, K.J., Hoffmann, D.
Toxic and carcinogenic agents in undiluted
mainstream and sidestream smoke of different
types of cigarettes. Carcinogenisis 8: 729-731,
1987.
Armitage, A., Dollery C., Houseman T., Kohner E.,
Lewis P.J., Turner, D. Absorption of nicotine
from small cigars. Clinical Pharmacol Ther 23:
143-151, 1978.
Brunnemann, K.D., Hoffmann, D. Chemical Studies on
Tobacco Smoke LIX Analysis of volatile nitro-
samines in tobacco smoke and polluted indoor
environments: environmental aspects of n-nitroso
compounds. Walker EA, Castegnaro M., Giciute
L., and Lyle R.E., eds. Lyon, France: IARC
Scientific Publications No. 19. 343-356, 1978.
Brunnemann, K.D., and Hoffmann, D. Chemical
Studies on Tobacco Smoke XXIV. Gas chromato-
graphic determination of ammonia in cigarette
and cigar smoke. J Chromatogr Sci 13: 159-163,
1975.
Brunnemann, K.D., Stahnke, G., Hoffmann, D.
Chemical Studies on Tobacco Smoke. LXI. Volatile
pyridines: quantitative analysis in mainstream and
sidestream smoke of cigarettes and cigars. Analyti-
cal Letters A11: 545-560, 1978.
Brunnemann, K.D., Yu, L., Hoffmann, D. Assessment
of carcinogenic volatile n-nitrosamines in
tobacco and in mainstream and sidestream
smoke from cigarettes. Cancer Res 37: 3218-
3222, 1977.
Buckley, T.J., Ott, W.R. Demonstration of real-time
measurements of PAH and CO to estimate in-
vehicle exposure and identify sources. Proc
International Symposium Measurements of Toxic
and Related Air Pollutants, U.S. EPA/AWMA,
Research Triangle Park, NC, May 1996.
Cigar Aficionado Bi-Monthly Magazine. M. Shanken
Communications, 387 Park Ave. South, N.Y.,
N.Y. 10016 May/June Issue, 1997.
CPRT Laboratories Inc. Final Report - Development
of methods for the characterization of toxic
constituents in cigars, pipe tobacco and
smokeless tobacco. SSC Contract No. H4078-1-
C230/01-SS. Submitted to The Tobacco Branch,
Health Canada. (M. Kaiserman, personal
communication, 1997)
Curtis, B. Bob Curtis’s Cigar Database (8/21/95).
http://www.netins.net/showcase/fujicig/
bcdb.hmtl. (21 August 1995)
Daley, P.S., Lundren, D.A. The performance of
piezoelectric crystal sensors used to determine
aerosol mass concentrations, Am. Ind. Hyg.
Assoc. J. 26: 518-532, 1975.
Hoffmann, D, Adams J.D., Brunnemann, K.D., Hecht,
S.S. Assessment of tobacco-specific N-nitro-
samines in tobacco products. Cancer Research
39: 2505-2509, 1979.
IARC Monographs on the Evaluation of Carcinogenic
Risks to Humans Tobacco Smoking, Vol 38,
IARC, Lyon, 1986.
Klepeis, N.E., Ott, W.R., Repace, J.L. The effect of
cigars on indoor air quality. Journal of Exposure
Analysis and Environmental Epidemiology, In
press.
Klepeis, N.E., Ott, W.R., Switzer, P. A Multiple-
smoker model for predicting air quality in public
lounges,” Environ. Sci. Technol. 30 (9), 2813 -
2820, 1996.
Langan, L. Portability in measuring exposure to
carbon monoxide, J Exposure Analysis and
Environmental Epidemiology, Suppl. 1, 223-289,
1992.
Leaderer, B. Assessing exposure to environmental
tobacco smoke. Risk Analysis 10: 19-26, 1990.
Mage, D.T., Ott, W.R. Accounting for nonuniform
mixing and human exposure in indoor
microenvironments. In characterizing sources of
Indoor AF pollution and related sink effects,
TIchenor, B.A., ed., West Conshohocken, Pa,
ASTM STP 1287, PCN 04-12870-17, 263-269,
1996.
Nelson, P. Testimony of R.J. Reynolds Tobacco
Company, OSHA Docket No. H-122, comment
8-266, Indoor Air Quality, Proposed Rule, U.S.
Occupational Safety & Health Administration,
Washington, D.C., 1994.
Ott, W.R., Switzer, P., Willits, N. Trends of in-vehicle
CO exposures on a California arterial highway
over one decade, Paper No. 93-RP-116B.04
presented at the 86th Meeting of the Air and
Waste Management Association, Denver, Co,
1996.
Ott, W.R., Wilson, N.K., Klepeis, N., Switzer, P. Real-
time monitoring of polycyclic aromatic
hydrocarbons and respirable suspended particles
from environmental tobacco smoke in a home.
Proc 1994 EPA/A&WMA Int Symposium on Meas of
Toxic and Related Air Pollutants VIP-39, Air &
Waste Mgt Assoc Pittsburgh, 887-892, 1994.
Ott, W., Langan, L., Switzer, P. A time series model
for cigarette smoking activity patterns: model
validation for carbon monoxide and respirable
particles in a chamber and an automobile, J.
Exposure Anal. Environ. Epidemiol. (2), 175-200,
1992.
Ott, W.R., Switzer, P., Robinson, J. Particle concen-
trations inside a tavern before and after
prohibition of smoking: evaluating the
performance of an indoor air quality model, J
Air Waste Manag Assoc 46: 1120-1134, 1996.
REFERENCES

179
Smoking and Tobacco Control Monograph No. 9
Ott, W.R., Vreman, H.J., Switzer, P., Stevenson, D.K.
evaluation of electrochemical monitors for
measuring carbon monoxide concentrations in
indoor, in-transit, and outdoor microenviron-
ments, presented at the International Symposium
on the Measurement of Toxic and Related Air
Pollutants of the Air and Waste Management
Association, Research Triangle Park, N.C., 1995.
Repace, J.L., Lowrey, A.H. Indoor air pollution, tobacco
smoke, and public health. Science 208: 464, l980.
Repace, J.L., Lowrey, A.H. tobacco smoke, ventilation,
and indoor air quality, ASHRAE Transactions 88:
Part I, 895, l982.
Repace, J.L. Indoor concentrations of environmental
tobacco smoke: models dealing with effects of
ventilation and room size. In: Environmental
Carcinogens Methods of Analysis and Exposure
Measurement, Vol. 9: Passive Smoking. (I.K.
O’Neill, K.D. Brunnemann, B. Dodet, and D.
Hoffmann, eds.) International Agency for
Research on Cancer, Lyon France. 25-41, 1987.
Resnick J. International Connoisseur’s Guide to Cigars.
New York: Black Dog and Leventhal Publishers,
1996.
Rickert, W.S., Robinson, J.C., Bray, D.F., Rogers, B., and
Collishaw, N.E. Characterization of tobacco
products: A Comparitive Study of the Tar,
Nicotine, and Carbon Monoxide Yields of Cigars,
Manufactured Cigarettes, and Cigarettes Made
from Fine-cut Tobacco. Preventive Medicine 14:
226-233, 1985.
Rickert, W.S., Robinson, J.C., Collishaw, N. Yields of
tar, nicotine, and carbon monoxide in the
sidestream smoke from 15 brands of Canadian
cigarettes,” Am J Pub Health, 74 (3), 228-231, 1984.
Rosanno, A.J., Owens, D.F. Design procedures to
control cigarette smoke and other air pollutants,
ASHRAE Trans., 75, 93-102, 1969.
Schmeltz, .I, Brunnemann, K.D., Hoffmann, D., Cornell,
A. On the chemistry of cigar smoke: Comparison
Between Experimental Little and Large Cigars.
Beitrage zur Tabakforschung: 8: 367-377, 1976.
Sem, G.J., Tsurubayashi, K. A New mass sensor for
respirable dust measurement, Am. Ind. Hyg. Assoc.
J., 36, 791-800, 1975.
Sem, G.J., Tsurubayashi, K., Homma, G.J. performance
of the piezoelectric microbalance respirable aerosol
sensor, Am. Ind. Hyg. Assoc. J. 38, 580-588, 1977.
Switzer, P., Ott, W. R. Derivation of an indoor air
averaging time model from the mass balance
equation for the case of independent source inputs
and fixed air exchange rates,” J. Exposure Anal.
Environ. Epidemiol., 2 (2), 113-135, 1977.
U.S. Department of Health, Education, and Welfare.
Smoking and Health. A Report of the Surgeon General.
U.S. Department of Health Education, and
Welfare, Public Health Service, Office of the
Assistant Secretary for Health, Office on Smoking
and Health. DHEW Publication No. (PHS) 79-
50066, 1979.
U.S. Department of Health and Human Services. The
Health Consequences of Involuntary Smoking. A Report
of the Surgeon General. DHHS (CDC) 87-8398,
Washington, D.C., 1986.
USEPA National Ambient Air Quality Standards for
PM10, PM2.5, and CO. Federal Register:
Wallace LA. Indoor particles: a review. J Air Waste
Manage Assoc 46:98-126, 1996.
Wilson, N.K., Barbour, R.K., Chuang, J.C., and Mukund,
R. Evaluation of a real-time monitor for fine
particle-bound PAH in air. Polycyclic Aromatic
Compounds 5: 167-174, 1994.
Wilson, N.K., Barbour, R.K., Burton, R.M., Chuang, J.C.
Mukund, R. Evaluation of a Real-Time monitor for
particle-bound PAH in air. Proc. 1993 U.S. EPA/
A&WMA Int. Symp. on Meas. of Toxic & Related Air
Pollutants. Air &Waste Mg Assoc, Pittsburgh, Pa,
451-456, 1993.

181
Smoking and Tobacco Control Monograph No. 9
Pharmacology and Abuse Potential of Cigars
Reginald V. Fant and Jack E. Henningfield
INTRODUCTION Cigar tobacco contains the highly addictive drug nicotine in
concentrations similar to those observed in cigarettes; however, since most
cigars contain more tobacco, they also contain more nicotine than cigarettes.
Most cigar smokers do not inhale cigar smoke, and those who do inhale far
less than typical cigarette smokers (Chapter 4). The pH of the smoke from
most cigars is sufficiently alkaline to enable efficient absorption of nicotine
through the oral and nasal mucosa. These basic observations, along with the
behavioral observation that some cigar smokers report symptoms of
dependence and withdrawal similar to those of cigarette smokers, have led
the American Psychiatric Association to include cigars along with cigarettes in
their manual listing drug dependence and other disease states (American
Psychiatric Association, 1987). This chapter will review the scientific
evidence supporting the categorization of cigars as dependence-producing
nicotine delivery devices.
EARLY OBSERVATIONS The history of tobacco use includes accounts of cigar
OF ADDICTIVE EFFECTS smoking by native Americans dating back more than
1000 years. In fact, when the term addiction was applied to describe the
enslavement of some people to their tobacco in the late 1700’s, the main
forms of tobacco smoking were cigar and pipe smoking (Murray et al., 1991).
The cigarette, which is now the most commonly used nicotine delivery
device, did not make its appearance in common use until the 1840’s (McKim,
1986).
It has long been recognized that cigars contain and deliver psychoactive
doses of nicotine. The concept that tobacco strain, growing conditions, and
manipulation of the pH of nicotine preparations could greatly affect the
amount of nicotine available from cigars was reported by Graham and
Carr in 1924. In 1925, Mendenhall noted that the experiments in which a
pipe or cigar was smoked were more likely to have subjects report feelings
of being dizzy or sick than experiments in which subjects smoked cigarettes,
presumably because the cigars and pipes delivered more nicotine than
cigarettes. In 1931, Lewin reported on the psychoactive effects of cigars,
noting the ceremonial use of cigars to produce a strong psychosis during
which a young man can “see spirits which prophesy his future and endow
him with strength, knowledge and happiness” (from Phantastica: Narcotic
and Stimulating Drugs, Their Use and Abuse reprinted in English by E. P.
Dutton and Company, 1964). Lewin concluded that the pharmacological
effects of tobacco, smoked or unsmoked, were primarily due to the nicotine
released from the tobacco and absorbed by the person. Other pharmacologic
effects of cigar smoking, including tolerance, pleasure, and tranquilization
were described by Gies et al. in 1921, who concluded that these effects
contributed to the habitual use of cigars. Interestingly, Gies and colleagues
(1921) listed cigars before cigarettes in the order of greatest to least degree of
psychoactive and toxic potency.

Chapter 6
182
Other psychological and physiological effects of cigar smoking have
also been referenced in classic early psychopharmacology research. Bates
reported on the cardiovascular (Bates, 1922a), as well as the cognitive and
psychomotor (Bates, 1922b) effects of cigar smoking. Bates showed that
smoking increased systolic and diastolic blood pressure, as well as heart rate.
Mixed results of cigar smoking and cigar smoke deprivation were seen on
psychomotor and cognitive performance tasks which included arithmetic
and dart throwing. Dixon (1928) also reported on the cardiovascular effects
of cigar smoking as well as the on the cognitive-enhancing effects of cigar
smoking and the lowered cognitive performance produced by deprivation
from cigars. In 1927, Dixon reported on the psychoactive and performance
effects of cigar smoking and stated that “acquired tolerance to nicotine is
probably the same as that of morphine” (p. 20). Thus the concept that many
of the effects of cigar smoking are due to nicotine has been understood for
well over 70 years.
NICOTINE DOSING Cigars contain and deliver a wide range of biologically-active
CAPABILITY OF chemicals, several of these such as nicotine, acetaldehyde, and
CIGARS carbon monoxide can serve to modify behavior. However, of all
the chemicals known to be common across most cigar brands, nicotine is the
only known dependence-producing drug present in substantial quantities.
This section examines the nicotine dosing capabilities of cigars in greater
detail to determine how cigars compare to products known to readily cause
nicotine addiction, namely cigarettes and smokeless tobacco.
The nicotine delivery of cigars is a complex issue due to the variability
in size, nicotine content, and pH of various cigar brands. Henningfield et al.
(1996) examined characteristics of ten cigar brands selected from a cigar
retailer in Baltimore. Table 1 summarizes the results of this study. The
weight of the cigars examined ranged from 0.77 to 22 g, and the nicotine
content of these products ranged from 10 to 444 mg. The pH of the tobacco
in solution also varied greatly, with values ranging from 6.2 to 8.2. By
contrast, cigarettes typically weigh less than 1 g and contain an average of
8.4 mg nicotine (Benowitz et al., 1983), and cigarette tobacco is generally
mildly acidic with pH values ranging from 5.5 to 6 (Brunneman and
Hoffmann, 1974). Additionally, in 1996, 98.2 percent of cigarettes produced
in the United States had filters which prevent the direct contact of the
cigarette tobacco with the lips and the buccal mucosa (United States
Department of Agriculture, 1997).
The data in Table 1 indicate that cigars contain amounts of nicotine
ranging (on the low end) from that equivalent to a single cigarette to (on
the high end) that equivalent to an entire pack of cigarettes. With the
exception of cigars that are similar in size to cigarettes, most cigars contain
nicotine in quantities equivalent to several cigarettes. In addition, the higher
pH of cigar tobacco and cigar smoke may result in a higher proportion of the
nicotine contained in a cigar being in free unprotonated form and more
available for absorption via the mouth, nose, and throat than is the case with
cigarettes.

183
Smoking and Tobacco Control Monograph No. 9
Table 1
Physical characteristics of ten cigars selected at random from a cigar retailer in Baltimore, MD,
November 1995* (Reprinted from Henningfield et al., 1996)
Total
Nicotine Nicotine
Length Diameter Weight Concentration Content Tobacco
Code (mm) (mm) (g) (mg/g) (mg) pH
A 68 8 0.77 14.95 16.59 6.2
B 79 8 1.12 9.00 10.08 6.6
C 124 17 9.56 17.40 166.30 6.8
D 125 12 4.20 4.70 19.74 7.6
E 138 17 12.60 8.43 106.22 7.3
F 148 12 5.78 10.74 62.07 7.2
G 149 16 10.06 7.75 77.79 8.0
H 170 17 15.37 16.35 251.30 6.7
I 198 21 22.00 22.00 444.00 7.1
J 214 20 21.29 8.90 189.50 8.2
* Nicotine content was determined by the HPLC method. Smoke pH was not assessed; however, the pH of the tobacco
was determined by suspending 2 g of tobacco in 10 ml of water, mixing, then testing at fixed intervals up to 60 min.
INHALATION OF The manner in which a person smokes a cigar also affects nicotine
CIGAR SMOKE delivery. Some cigar smokers regularly inhale smoke, whereas
others inhale very little (Turner et al., 1977). The pKa of nicotine is 8.02,
which means that 50 percent of nicotine is in an unionized state, and this free
unprotonated nicotine is present in the vapor phase of cigar smoke which
contributes to the nicotine's rapid absorption through the oral mucosa (Lide,
1991). Therefore, nicotine from cigars which generate smoke with a high pH
could readily be absorbed across the buccal mucosa, and smokers would not
need to inhale the smoke deeply into the lung to absorb substantial amounts
of nicotine. Absorption of nicotine through the buccal mucosa is highly pH
dependent; absorption in the lung is less influenced by pH due to the much
larger absorptive surface area of the lung. The smoke from cigarettes and
those cigars which produce low–pH smoke must therefore be inhaled in order
to absorb substantial amounts of nicotine. In contrast, cigar smokers with a
high–pH smoke can absorb nicotine by holding the smoke in their mouth,
or they can increase their absorption by inhaling. These differences in the
absorption of nicotine from cigar and cigarette smoke are likely to contribute
to the lower rates of inhalation among cigar smokers.
A cigar can also function much like a smokeless tobacco product such
as chewing tobacco or oral snuff (i.e., “spit tobacco”) and permit extraction
of nicotine from the unburned tobacco so that it can be absorbed directly
through the buccal mucosa and lips. This is possible for two reasons which

Chapter 6
184
distinguish most cigars from most cigarettes: (1) most cigars have neither
filters nor tips and are designed and used in a manner such that tobacco
leaf material is in direct contact with the lips and to a lesser extent, with the
tongue and gums; this contact serves to moisten the leaf and enable extraction
of its nicotine; (2) most cigars are manufactured with tobacco leaf material
which has been cured and/or buffered so as to produce a mildly alkaline
tobacco which facilitates nicotine transfer.
Several studies have examined the absorption of nicotine from cigar
smoke in human cigar smokers as well as in animals exposed to cigar smoke.
Armitage and Turner (1970) examined delivery of nicotine by cigars and
cigarettes through the oral mucosa in cats. The authors found that
pharmacologic responses to the smoke were greater following cigar smoke
exposer than following cigarette smoke exposer despite the fact that more
nicotine was present in the cigarette smoke (4.4 mg versus 4.0 mg after 30
puffs of cigarette and cigar smoke, respectively). The authors interpreted these
results to mean that more nicotine was absorbed from the cigar smoke due to
the higher pH values in the cigar smoke (pH = 5.4 for cigarette and 8.5 for cigar
smoke). Armitage and Turner (1970) also describe a separate experiment in
which carotid blood levels of nicotine were measured after placing solutions of
nicotine with pH values of 6, 7, and 8 in the mouths of cats. The authors
found that absorption of nicotine in the first 2.5 min was 8 times higher
following the pH 8 solution compared to the pH 6 solution.
Pechacek et al. (1985) examined serum thiocyanate levels, a chemical
marker for inhaled tobacco smoke, in cigarette smokers, ex-cigarette-smoking
cigar and pipe smokers, and never-cigarette-smoking cigar and pipe smokers.
The authors found that cigarette smokers inhaled the greatest amount of
tobacco smoke, followed by ex-cigarette smokers, then never-cigarette-smoking
smokers of cigars and pipes. The authors suggest that most cigarette smokers
inhale, whereas only some cigar smokers inhale, and that inhalation among
cigar smokers is influenced by former cigarette smoking status. Serum
thiocyanate levels were also related to the number of cigars smoked per day;
subjects who smoked four or more cigars per day had serum thiocyanate levels
comparable to cigarette smokers who smoked ten cigarettes per day. However,
most of these heavy (> 4 per day) cigar smokers also tended to be ex-cigarette-
smokers.
Similar results were found in a study by Turner et al. (1986) in
which carboxyhemoglobin was used as the biological marker of inhaled
tobacco smoke. Turner et al. found that the mean concentration of
carboxyhemoglobin was 4.8 percent of the total hemoglobin among cigarette
smokers, compared to 0.9 percent among never-cigarette- smoking cigar
smokers and 6.8 percent former-cigarette smoking cigar smokers.
Combined data from more than 8,000 tobacco smokers, of whom more
than 1,000 smoked cigars or pipes, from the Multiple Risk Factor Intervention
Trial (MRFIT) confirmed significant levels of tobacco exposure (based on serum
thiocyanate) and smoke inhalation (based on expired air carbon monoxide)
among cigar smokers as compared to non tobacco users (Ruth and Neaton,

185
Smoking and Tobacco Control Monograph No. 9
1991). Not surprisingly, overall levels of nicotine and smoke exposure were
lower and more variable among cigar smokers than among cigarette smokers.
Another analysis of data from MRFIT indicated that switching from cigarette
smoking to cigar or pipe smoking resulted in decreased smoke exposure, but
that levels remained significantly higher than those observed during tobacco
abstinence (Ockene et al., 1987). The former cigarette smokers were also
more likely to report inhaling cigar or pipe smoke into the lung than were
cigar smokers who had never smoked cigarettes. The MRFIT data on cigar
smoke inhalation patterns by former cigarette smokers are consistent with
those reported in Chapter 2 and show that less than 15 percent of cigar
smokers who never smoked cigarettes reported inhaling smoke into the lung,
more than 20 percent of former cigarette smokers and approximately
two-thirds of concurrent cigar and cigarette smokers reported inhaling.
These data confirm that some cigar smokers who formerly or currently
smoke cigarettes are likely to obtain regular doses of nicotine by inhalation
of smoke directly into the lung.
RATE OF NICOTINE Armitage et al. (1978) examined the absorption of nicotine from
ABSORPTION small cigars labeled with 14C-nicotine. The authors found that
the amount of nicotine delivered to the smoker’s mouth during cigar
smoking was greater that that during cigarette smoking, but the proportion
retained by the subject was similar for cigars and cigarettes. Arterial nicotine
concentrations were comparable for the two products, but the rise in arterial
plasma nicotine levels was faster for cigarettes than for the small cigars. This
difference in rates of delivery is probably due to the route of absorption since
cigarette smoke is delivered largely through the lung, whereas cigar smoke is
delivered through both the oral and lung routes, mostly buccal in subjects
where there is little inhalation. Nicotine delivery to the brain is slower when
nicotine is absorbed across the oral mucosa compared to absorption across
the alveolar surfaces of the lung (Benowitz et al., 1988). In addition,
absorption through the pulmonary route is more complete than through
the oral route, which accounts for the fact that, whereas more nicotine was
actually delivered to the mouth by the small cigars than by the cigarettes,
similar amounts were actually retained.
Inhalation parameters have a dramatic affect on nicotine delivery. A
study which examined the absorption of nicotine from non-inhaled cigar
smoke found nicotine delivery to be slower than that observed following
cigarette smoke inhalation (Russell et al., 1980). The authors studied the
nicotine absorption from a single small cigar (6.2 g) and found an increase
in plasma nicotine of 16.5 ng/ml after 1 hour of smoking the single cigar
(Medallion Petit Corona).
Despite the acidic pH of cigarette smoke, inhalation into the lung can
produce arterial nicotine concentrations as much as ten times greater than
those concurrently observed in venous blood. Arterial levels achieving
values of nearly 100 ng/ml have been reported with smokers smoking a
single cigarette (Henningfield et al., 1993).

Chapter 6
186
In summary, cigars have the capability to provide high levels of nicotine
exposure, whether or not their smoke is inhaled. Furthermore, measures
of physiologic response (e.g., Gies, 1921; Bates, 1922a, 1922b), as well as the
toxicological consequences of cigar smoking (Chapter 3 and 4), demonstrate
that humans can be exposed to high levels of nicotine through their
consumption of cigars. On the other hand, the extraordinary variability
in cigar nicotine content, the pH of tobacco and tobacco smoke , and
inhalation patterns of cigar smokers imply that a wide range of levels of
absorption, and potentially of dependence, would be expected to occur.
Drug Addiction: “Drug addiction” is the common term for the various medical
Basic Concepts and social disorders related to the compulsive ingestion of
and Definitions psychoactive chemicals. The term “drug addiction” is often used
interchangeably with the term “drug dependence” even though the term
“drug dependence” is the preferred technical term in the scientific and
medical literature. In this report, the terms “addiction” and “dependence”
will be used interchangeably to refer to the syndrome of drug seeking
behavior that meets criteria described in Table 2.
The occurrence of an abstinence-induced withdrawal syndrome may
also play a role in the development of drug dependence. A drug withdrawal
syndrome reflects an adaptation of behavioral and physiologic processes such
that physiologic, cognitive and behavioral functioning are impaired when
the drug is no longer present. This effect of drug exposure can complicate the
process of achieving and maintaining drug abstinence, and the symptoms
Table 2
1988 Surgeon General’s report criteria for drug dependence (US DHHS, 1988)
Primary Criteria:
Highly controlled or compulsive use
Psychoactive effects
Drug-reinforced behavior
Additional Criteria:
Addictive behavior often involves:
stereotypic patterns of use
use despite harmful effects
relapse following abstinence
recurrent drug cravings
Dependence-producing drugs often produce:
tolerance
physical dependence
pleasant (euphoriant) effects

187
Smoking and Tobacco Control Monograph No. 9
can be so unpleasant as to precipitate relapse in those who do achieve
abstinence (Jaffe, 1985; US DHHS, 1988). Drug addiction can be powerful
even in the absence of a withdrawal syndrome, however. In fact, the
majority of people monitored in surveys by the National Institute on Drug
Abuse who regularly use addictive drugs (including cocaine and marijuana)
report that they have not experienced withdrawal, even though many of
these people feel dependent and have been unable to maintain abstinence
(US DHHS, 1988).
NICOTINE Tolerance to the effects of nicotine is demonstrated by the fact that
DEPENDENCE most cigarette smokers increase their consumption of cigarettes over
time. Daily use increases over several years and then stabilizes. Only 10 to
15 percent of cigarette smokers smoke fewer than five cigarettes per day
(Shiffman, 1989; Giovino, 1991). Between 1/3 and 1/2 of people that try
even one cigarette develop an escalating pattern of use. This rate is much
higher than that seen with other addictive drugs (US DHHS, 1994). Current
epidemiological data suggest that the majority of adult cigar smokers
maintain patterns of intermittent use and smoke fewer cigars per day than is
seen in cigarette smokers (Chapter 2).
The extensive studies of time course and symptomology of withdrawal
symptoms that have been conducted in cigarette smokers have not been
duplicated in cigar smokers; however, several lines of evidence suggest
that it may be possible for cigar smokers to develop a similar syndrome
of withdrawal. Withdrawal symptoms from cigarettes, which primarily
involve lung-delivered nicotine, are generally similar in nature, but higher
in magnitude when compared to withdrawal symptoms associated with
smokeless tobacco use, which primarily involve bucally-absorbed nicotine
(Figure 1) (Centers for Disease Control and Prevention, 1994). A pattern of
increasing severity of symptom development with increasing frequency of
use is present for use of both cigarettes and smokeless tobacco. Other
research on withdrawal from cigars and smokeless tobacco confirms the
similarities in withdrawal symptoms across nicotine delivery formulations.
However, it appears that formulations which deliver nicotine very slowly
(e.g., nicotine patch and smokeless tobacco), or in generally low daily
doses (e.g., nicotine gum as typically used), result in weaker syndromes
of abstinence-associated withdrawal. Discontinuation of smokeless
tobacco results in less reliable and/or weaker syndromes of withdrawal
than discontinuation of cigarette smoking (e.g., Hatsukami et al., 1987;
Henningfield, et al., 1997). These observations raise the possibility that
withdrawal syndromes may be associated with regular heavy cigar smoking
(which typically involves less lung exposure to nicotine than cigarette
smoking). However, comparisons are complicated by the extraordinarily
wide variation in nicotine delivery characteristics across cigars and smoke
inhalation patterns of cigar smokers along with the absence of specific data
for cigar smokers.

Chapter 6
188
Percent Ratings of “Yes”
“Find it hard to concentrate”
0 1-14 15-29 30
0
10.0
20.0
30.0
40.0
50.0
Cigarette Smokers
SLT Users
60.0
70.0
80.0
90.0
Percent Ratings of “Yes”
0 1-14 15-29 30
0.0
10.0
20.0
30.0
40.0
50.0
Cigarette Smokers
SLT Users
60.0
70.0
80.0
90.0
Percent Ratings of “Yes”
0 1-14 15-29 30
0.0
10.0
20.0
30.0
40.0
50.0
Cigarette Smokers
SLT Users
60.0
70.0
80.0
90.0
“Feel more irritable”
“Strong need/urge to smoke/chew”
Days Used in Past 30 Days
Figure 1
Symptoms of nicotine withdrawal among adolescents and young adults by the number of days
of reported use of cigarettes or smokeless tobacco within the past month. Reported withdrawal
symptoms significantly increased as a function of days used (Centers for Disease Control and
Prevention, 1994).

189
Smoking and Tobacco Control Monograph No. 9
FACTORS INFLUENCING The level of dependence of nicotine in adults has been
NICOTINE DEPENDENCE found to be inversely related to the age of initiation of
smoking when measured by diagnostic criteria of the American Psychiatric
Association (Breslau et al., 1992) or by Fagerstrom Tolerance Questionnaire
Score (Henningfield, 1987). Because cigars vary so widely in their nicotine
dosing characteristics, it is possible for an individual to obtain as much
nicotine from one or two cigars with substantial nicotine dosing capacity
as from a much larger number of smaller cigars or cigarettes. Because
nicotine may be extracted directly from lip contact with the cigar tip itself,
the common practice of keeping an unlit cigar in the mouth may also
contribute to the total daily nicotine intake of some cigar smokers.
For many people, the process of graduation from first use to addiction
is not immediate and can take months or even years (US DHHS, 1988).
Initial experiences with tobacco, as with other addictive substances, are often
negative, requiring social pressures and other factors to maintain exposure
until the addiction develops (Haertzen et al., 1983). Over the course of many
months, tolerance develops such that dysphoric subjective effects become
minimal and much higher doses are needed to obtain the desired euphoric
effects. At that point, mood, behavior, physiologic function, and cognition
require the continued presence of nicotine to enable the person to feel
normal — the person has become dependent.
With respect to cigarette smoking, 80 to 90 percent of all current
cigarette smokers smoke more than five cigarettes and the vast majority of
these individuals display symptoms of nicotine dependence. Some
individuals who smoke fewer than six cigarettes per day appear able to smoke
with a much greater degree of volition and display few symptoms of nicotine
withdrawal upon cessation (Shiffman, 1989; US DHHS, 1988).
The proportion of cigar smokers showing clear signs of dependence
remains unknown. Lower rates of inhalation in cigar smokers and slower
absorption of nicotine through the buccal mucosa suggest that cigar smoking
may have a lower potential to induce addiction to nicotine than cigarette
smoking . In addition, it is plausible that persons who never had been
nicotine dependent and who began smoking cigars in adulthood would be
at a lower risk for developing dependence than children and adolescents
who take up tobacco use. It does appear that a much higher proportion of
adult cigar users compared to adult cigarette smokers are non daily users
(Chapter 2).
It has long been observed that drug use that is restricted to occurring
only in conjunction with social rituals may be less likely to escalate to
patterns of abuse and severe dependence (e.g., Falk, 1983). These
observations suggest that cigar smokers who do not begin smoking until
adulthood, and who were not formerly nicotine-dependent, and who smoke
only in certain settings (e.g., New Year’s Eve) might be less likely to escalate
their use and become dependent than someone who began smoking at a
younger age.

Chapter 6
190
Nicotine polacrilex gum and transdermal patch systems have low abuse
liability, in part because rapid absorption is not possible from either nicotine
delivery system. (Henningfield and Keenan, 1993; Henningfield and Stitzer,
1991; US DHHS, 1988). Cigar smoke may be inhaled, producing the same
virtually instantaneous effects of nicotine delivery produced by cigarette
smoking, or cigar smoke may be held in the nose and mouth providing a
somewhat slower rate of nicotine absorption as occurs with smokeless tobacco
products. Both routes of nicotine delivery are well-documented to lead to
dependence and withdrawal with other forms of tobacco use (cigarettes and
smokeless tobacco (US DHHS, 1986, 1988).
Henningfield and Keenan (1993) examined the pharmacokinetics of
nicotine delivered by different routes of administration as well as the changes
in subjective “liking” for the drugs. They found that nicotine delivered
intravenously and through cigarette smoke was very rapidly absorbed and
produced high scores on a question of subjective “liking” which may be
indicative of the abuse liability of the drug (Jasinski et al., 1984). Nicotine
delivered transdermally, however, was absorbed slowly and produced very
low scores of drug liking, despite the achievement of comparable venous
plasma levels. Because nicotine delivery through cigar smoke is primarily
through the oral mucosa with delivery through the pulmonary route as well
for those who inhale the smoke, it is likely that the delivery kinetics of
nicotine may be more comparable to smokeless tobacco which had scores
of subjective liking falling somewhere between those of transdermal and
cigarette delivery. These observations suggest that the risk of becoming
nicotine dependent might be somewhat lower in the cigar smokers as
opposed to cigarette smokers.
It is likely that nicotine tolerance and physical dependence to cigars may
develop among heavy regular users. However, there would be little basis to
expect that substantial levels of physical dependence would be observed in
people who rarely smoked on two or more consecutive days. Nicotine has
a half-life of approximately 2.5 hours and therefore, smoking a single cigar
or smoking with a non-daily frequency would not create a chronic exposure
to nicotine. Exposure of at least a few weeks is felt to be necessary to create
the degree of physical dependence that would enable substantial withdrawal
symptoms to develop upon cessation of use (American Psychiatric
Association, 1994). Table 3 gives DSM-IV criteria for nicotine withdrawal.
The novice cigar smoker would certainly feel a number of adverse effects
during smoking the first cigar, much as a first-time cigarette smoker would.
These effects would include the nausea and lightheadedness associated with
nicotine administration. After several cigars, however, these effects should
dissipate, allowing the cigar smoker to use more of the product.

191
Smoking and Tobacco Control Monograph No. 9
Table 3
DSM-IV criteria for nicotine withdrawal (American Psychiatric Association, 1994)
A. Daily use of nicotine for at least several weeks.
B. Abrupt cessation of nicotine use, or reduction in the amount of nicotine used, followed within 24 hours by
four (or more) of the following signs:
(1) dysphoric or depressed mood
(2) insomnia
(3) irritability, frustration, or anger
(4) anxiety
(5) difficulty concentrating
(6) restlessness
(7) decreased heart rate
(8) increased appetite or weight gain
C. The symptoms in Criterion B cause significant distress or impairment in social, occupational, or other
important areas of functioning.
D. The symptoms are not due to a general medical condition and are not better accounted for by another
mental disorder.
CONCLUSIONS
1. Cigars contain amounts of nicotine that vary from the amounts
contained in a single cigarette to the amount contained in a pack or
more of cigarettes. The amount of nicotine is usually proportional
to the amount of tobacco contained in the cigar.
2. There is substantial variability in the pH of the tobacco smoke produced
by cigars, but most cigars produce smoke that is more alkaline than
cigarette smoke. This alkaline pH facilitates nicotine absorption across
the oral mucosa and may explain why cigar smokers are less likely to
inhale than cigarette smokers.
3. There is sufficient nicotine absorption among regular heavy cigar
smokers to expect that nicotine dependence might develop, but studies
to document the frequency or intensity of nicotine dependence have not
been published.
4. The pattern of cigar use in the population (infrequent use, low number
of cigars smoked per day, and lower rates of inhalation compared to
cigarette smokers) suggest that cigar use which begins in adulthood may
be less likely to produce dependence than cigarette smoking. However,
most of the cigar smokers studied began smoking cigars as adults. The
current trend of adolescent cigar use generates a concern that prior low
adult rates of developing dependence may not apply to cigar use begun
during adolescence.

Chapter 6
192
REFERENCES
American Psychiatric Association. Diagnostic and
Statistical Manual of Mental Disorders, 3rd Edition
(revised). Washington, DC: American Psychiatric
Press, 1987.
American Psychiatric Association. Diagnostic and
Statistical Manual of Mental Disorders, 4th Edition.
Washington, DC: American Psychiatric Press, 1994.
Armitage, A., Dollery, C., Houseman, T., Kohner, E.,
Lewis, P. J., Turner, D. Absorption of nicotine from
small cigars. Clinical Pharmacology and Therapeutics,
23: 143-151, 1978.
Armitage, A.K., Turner, D.M. Absorption of nicotine in
cigarette and cigar smoke through the oral mucosa.
Nature, 226: 1231-1232, 1970.
Bates, R.L. The effects of cigar and cigarette smoking on
certain psychological and physiological functions: II.
Blood pressure and heart rate. Journal of Comparative
Psychology, 2: 431-505, 1922a.
Bates, R.L. The effects of cigar and cigarette smoking on
certain psychological and physiological functions: I.
Dart throwing. Journal of Comparative Psychology, 2:
371-423, 1922b.
Benowitz, N.L., Hall, S. M., Herning, R. I., Jacob, P.,
Jones, R. T., Osman A. L. Smokers of low yield
cigarettes do not consume less nicotine. New
England Journal of Medicine, 309: 139-142, 1983.
Benowitz, N.L., Porchet, H., Sheiner, L., Jacob, P.
Nicotine absorption and cardiovascular effects with
smokeless tobacco use: Comparison with Cigarettes
and Nicotine Gum. Clinical Pharmacology and
Therapeutics, 44: 23-28, 1988.
Breslau, N., Fenn. N., Peterson, E.L. Early smoking
initiation and nicotine dependence in a cohort of
young adults. Drug and Alcohol Dependence, 33: 129-
137, 1992.
Brunneman, K.D., Hoffmann, D. The pH of tobacco
smoke. Food and Cosmetics Toxicology, 12: 115-124,
1974.
Centers for Disease Control and Prevention. Reasons for
tobacco use and symptoms of nicotine withdrawal among
adolescent and young adult tobacco users-United States,
1993. Morbidity and Mortality Weekly Report
43(41): 745-750, 1994.
Dixon, W.E. The physiological effects of smoking.
Practitioner, 118: 20-28, 1927.
Dixon, W.E. The tobacco habit. British Journal of
Inebriety (Alcoholism and Drug Addiction), 25: 99-
121, 1928.
Falk, J.L. Drug dependence: Myth or motive?
Pharmacology, Biochemistry and Behavior, 19: 385-391,
1983.
Gies, W.J., Kahn, M., Limerick, O. V. The effect of
tobacco on man. New York Medical Journal, June 1:
809-811, 1921.
Giovino, G.A. Public-health perspectives. Henningfield,
J.E., and Stitzer, M. L. (eds.). In: New Developments in
Nicotine-Delivery Systems. New York: Cortland
Communications, pp. 3-10, 1991.
Graham, V., Carr, R. H. Chemical factors determining
the quality of tobacco. Journal of the American
Chemical Society, 46: 695-702, 1924.
Haertzen, C.A., Kocher, T.R., Miyasato, K.
Reinforcement from the first drug experience can
predict later drug habit and/or addiction: Results
with coffee, cigarettes, alcohol, barbiturates, minor
and major tranquilizers, stimulants, marijuana,
hallucinogens, heroin, opiates and cocaine. Drug and
Alcohol Dependence, 11: 147-165, 1983.
Hatsukami, D.K., Gust, S.W., Keenan R.M. Physiologic
and subjective changes from smokeless tobacco
withdrawal. Clinical Pharmacology and Therapeutics
41: 103-107, 1987.
Henningfield, J.E. Acquisition of dependence to
cigarettes and smokeless tobacco. In: Annual Report of
the Addiction Research Center. Rockville, MD: US
DHHS, p. 36, 1987.
Henningfield, J.E., Fant, R.V., Tomar, S. L. Smokeless
tobacco: An addicting drug. Advances in Dental
Research, 11: 330-335, 1997.
Henningfield, J.E., Hariharan, M., Kozlowski, L.T.
Nicotine content and health risk of cigars. JAMA,
276: 1857-1858, 1996.
Henningfield, J.E., Keenan, R.M. Nicotine delivery
kinetics and abuse liability. Journal of Consulting and
Clinical Psychology, 61: 743-750, 1993.
Henningfield, J. E., Stapelton, J. M., Benowitz, N. L.,
Grayson, R. F., and London, E.D. Higher levels of
nicotine in arterial than in venous blood after
cigarette smoking. Drug and Alcohol Dependence, 33:
23-29, 1993.
Henningfield, J.E., Stitzer, M. L. (eds.) New Developments
in Nicotine-Delivery Systems. New York: Cortland
Communications, 1991.
Jaffe, J.H. Drug addiction and drug abuse. Gilman, A.
G., Goodman, L. S., Rall, T. W. and Murad, F. (eds.)
Goodman and Gilman’s The Pharmacologic Basis of
Therapeutics, Seventh Edition. New York: MacMillan
Publishing Company, pp. 532-581, 1985.
Jasinski, D.R., Johnson, R.E., and Henningfield, J.E.
Abuse liability assessment in human subjects. Trends
in Pharmacological Science, 5: 196-200, 1984.
Lewin, L. Phantastica: Narcotic and Stimulating Drugs,
Their Use and Abuse. Reprinted in English 1964. New
York: E.P. Dutton and Company, 1931.
Lide, D.R. (ed.) CRC Handbook of Chemistry and Physics,
72nd ed. 1991-1992. Boca Raton: CRC Press, 1991.
McKim, W.A. Drugs and Behavior: An Introduction to
Behavioral Pharmacology. Englewood Cliffs, NJ:
Prentice-Hall, pp. 130, 1986.

193
Smoking and Tobacco Control Monograph No. 9
Mendenhall, W.L. A study of tobacco smoking.
American Journal of Physiology, 72: 549-557, 1925.
Murray, J., et al. New English Dictionary on Historical
Principles. Oxford: Clarendon Press, 1991.
Ockene J.K., Pechacek, T.F., Vogt, T., Svendsen, K.
Does switching from cigarettes to pipes or cigars
reduce tobacco smoke exposure? American Journal
of Public Health 77: 1412-1416, 1987.
Pechacek, T.F., Folsom, A.R., de Gaudermaris, R.,
Jacobs, D. R., Luepker, R. V., Gillum, R. F.,
Blackburn, H. Smoke exposure in pipe and cigar
smokers: serum thiocyanate measures. JAMA, 254:
3330-3332, 1985.
Russell, M.A.H., Jarvis, M.J., Feyerabend, C. A new age
for snuff? Lancet, 1: 474-475, 1980.
Ruth, K. J., Neaton, J. D. Evaluation of two biological
markers of tobacco exposure. Preventive Medicine 20:
574-589, 1991.
Shiffman, S. Tobacco ‘chippers’. Individual differences
in tobacco dependence. Psychopharmacology, 97:
539-547, 1989.
Turner, J.A. McM, McNicol, M.W., and Sillett, R.W.
Distribution of carboxyhaemoglobin
concentrations in smokers and non-smokers.
Thorax, 41: 25-27, 1986.
Turner, J.A. McM, Sillett, R.W., McNicol, M.W. The
effect of cigar smoking on carboxyhaemoglobin
and plasma nicotine concentrations in primary
pipe and cigar smokers and ex-cigarette smokers.
British Medical Journal, 2: 1387-1389, 1977.
U.S. Department of Agriculture. Tobacco Situation and
Outlook Report. Commercial Agriculture Division,
Economic Research Department, U.S. Department
of Agriculture, TBS-238, p. 5, 1997.
U.S. Department of Health and Human Services. The
Health Consequences of Involuntary Smoking. A
report of the Surgeon General. DHHS (CDC) 87-
8398, Washington, D.C. 1986
U.S. Department of Health and Human Services. The
Health Consequences of Smoking: Nicotine
Addiction: A Report of the Surgeon General, DHHS
publication No. (CDC) 88-8406. Washington DC:
U.S. Government Printing Office, 1988.
U.S. Department of Health and Human Services.
Preventing tobacco use among young people. A report of
the Surgeon General, 1994. U.S. Department of
Health and Human Services, Public Health Service,
Centers for Disease Control and Prevention, Office
on Smoking and Health (U.S. Government Printing
Office Publication No. S/N 017-001-00491-0).
Atlanta, GA: U.S. Government Printing Office,
1994.

195
Smoking and Tobacco Control Monograph No. 9
Marketing and Promotion of Cigars
John Slade
INTRODUCTION This chapter examines the recent commercial history of cigars in
the United States. Sales patterns, advertising, and apparent promotional
activities are explored. Most of the discussion of marketing activities is
descriptive, since few quantitative data are available. There is almost no
publicly available information on how the increased visibility that cigars
have achieved since about 1992 has been financed. Accordingly, what are
described in this chapter as promotional activities are not necessarily the
result of activities by commercial interests. They are, though, activities
that have probably contributed to the promotion of cigar consumption.
SALES PATTERNS Figure 1 charts the mean retail price of cigars from 1976 through
1996, adjusted for inflation. The inflation adjusted price of small cigars fell
steadily over the period, losing 52 percent of their initial average price by
1996. Inflation adjusted prices for cigarillos ended the period about where
they had begun despite a prolonged dip during the 1980’s. Large cigars
showed generally steady overall prices with some year to year fluctuations in
the 70’s and 80’s, but 1994 and 1995 were two consecutive years of
substantial increases in mean price, probably reflecting the relative growth of
the premium segment.
In a prospectus for the initial public offering of 5.4 million shares of
company stock, Consolidated Cigar Holdings Inc. pointed to several factors
which it believes have contributed to the increase in cigar sales in recent
years.
The Company believes that the growing cigar market and
increased demand for cigars continue to offer the Company
substantial growth opportunities. Recently, cigar smoking has
gained popularity in the United States, resulting in a significant
increase in consumption and retail sales of cigars, particularly for
premium cigars. Management believes that this increase in cigar
consumption and retail sales is the result of a number of factors,
including: (i) the increase in the number of adults over the age
of 50 (a demographic group believed to smoke more cigars than
any other demographic segment) and (ii) the emergence of an
expanding base of younger affluent adults who have recently
started smoking cigars and who tend to smoke premium cigars.
The Company believes the increase in cigar smoking is in large part
attributable to a positive and improving image of cigar smoking
resulting from increased publicity, including the success of Cigar
Aficionado magazine, the increased visibility of use by celebrities
and the proliferation of “Cigar Smokers” dinners and other special
events for cigar smokers. (Consolidated Cigar Holdings Inc., 1996,
p. 3)

Chapter 7
196
Figure 1
Mean retail price of various size cigars, U.S. 1976-1996, corrected for CPI (1982-1984 = 100)
Source: Maxwell, 1997
350
300
Dollars per Thousand
250
200
150
100
50
0
‘76
‘80 ‘85 ‘90 ‘95
Little
Cigarillo
Large

197
Smoking and Tobacco Control Monograph No. 9
Similarly, the CEO and the President of Culbro have stated,
The emergence and rise in popularity of cigar dinners, cigar
clubs, cigar bars and successful magazines such as Cigar Aficionado
lend additional credence to the link that now exists between
premium cigars and affluent consumers. (Culbro Corporation,
1996, p. 2)
The marketing of cigars has emphasized premium cigars; however,
when market shares of different brands are examined, inexpensive brands
of machine-made cigars actually dominate the cigar market (Table 1). The
leading brand is a machine-made variety of little cigars, Swisher Sweets,
which had a 19 percent market share in 1996. In contrast, the heavily
advertised premium brand Macanudo has only a 0.8 percent share. (General
Cigar is building Macanudo into a major name brand with a coordinated
campaign of advertising, sportswear, and ventures such as Club Macanudo
(Smoke Signals, 1997; Culbro Corporation, 1996).) Table 2 lists premium
brands of the largest U.S. cigar companies.
While there is a plethora of brands, styles, and sizes of cigars, only a
few companies sell most of them (Table 3). Just five companies, Swisher
International, Havatampa, Consolidated Cigar, Middleton, and Culbro
(General Cigar), control 95 percent of the market in the United States. Except
for Havatampa, which only sells machine-made cigars, each of the major
companies sells both premium and non-premium brands. In addition to the
major companies, a welter of small companies manufacture and import
premium cigars.
The market for little cigars is even more concentrated, with just three
companies, Swisher International, Consolidated Cigar, and Tobacco Exporters
International, controlling 86 percent of the market (Table 4). Swisher alone,
with its Swisher Sweets little cigars, has a 42 percent share. Table 4 also lists
the major brands of little cigar now on the market.
Many companies which manufacture or import cigars are involved in
other aspects of the tobacco business. Table 5 lists cigar companies which
also sell other tobacco products.
The recent rise in cigar sales has led to increased value of cigar companies
as investments. Several have made public share offerings and both popular
and trade magazines have offered information about these potential
investments (Wall Street Report, 1997; Luz, 1997; Finora, 1997).
There has been a marked increase in the number of smoke shops since
1992 (Flying High, 1997). The number of retail specialty tobacco outlets has
increased from 2,358 in 1992 to 4,948 in 1996. A sign that this increase has
drawn in many small businessmen who have not previously been involved
in the trade is the publication of an extensive article in a trade magazine
about the function of sales representatives (Scott, 1997).

Chapter 7
198
Table 1
Market share large cigars and cigarillos, United States, 1996, millions and percent
Brand Company Units Percent
Swisher Sweets Swisher Int’l 601 19.4
Phillies Havatampa Inc 462 15.0
Havatampa Havatampa Inc 258 8.3
White Owl General Cigar 184 6.0
Dutch Masters Consolidated 138 4.5
Garcia y Vega General Cigar 138 4.5
Antonio y Cleopatra Consolidated 124 4.0
King Edward Swisher Int’l 105 3.4
Muriel Consolidated 100 3.2
Backwoods Consolidated 98 3.2
Robert Burns General Cigar 87 2.8
El Producto Consolidated 53 1.7
William Penn General Cigar 44 1.4
Tijuana Smalls General Cigar 34 1.1
Macanudo General Cigar 26 0.8
Universal Swisher Int’l 24 0.8
La Corona Consolidated 13 0.4
Bering Swisher Int’l 10 0.3
Partagas General Cigar 9 0.3
Roi-Tan Consolidated 7 0.2
Canaria d’Oro General Cigar 2 0.1
Other, non-premium 340 11.0
Other, premium 233 7.5
Total 3,090 99.9
Premium brands in bold face.
Note: A premium cigar is hand-made, is comprised entirely of natural, long filler tobacco, and has a
retail price of more than $1.00.
Sources: Data on premium cigars and market share, Maxwell, 1997. Data on total U.S. consumption,
USDA, 1997.
ADVERTISING Only a small amount of conventional advertising appears for cigars.
Measured media spending increased from $1.1 million in 1994 to $4.0 million
in the first nine months of 1996 (Table 6). Most advertising for cigars appears
in magazines; 39 magazines carried cigar advertising in this 3-year period. As
of December 1996, the price for a one time insertion of a full-page, four-color
advertisement in Cigar Aficionado was $18,360 while a similar ad in Smoke cost
$7,950.
Cigar advertising employs a variety of themes. Cigars are presented as
lavish, even outrageous, yet affordable luxuries and indulgences. Other ads
depict a rich history and tradition of cigar making or appeal to nostalgia in
199
Smoking and Tobacco Control Monograph No. 9
Table 2
Premium brands of the major cigar companies
Company Premium brands
Consolidated Cigar H. Upmann
Montecristo
Don Diego
Te-Amo
Santa Damiana
Royal Jamacia
Primo Del Rey
Montecruz
General Cigar Macanudo
Partagas
Punch
Hoyo de Monterrey
Cohiba
Excalibur
Ramon Allones
Temple Hall
El Rey Del Mundo
Canaria D’Oro
Cifuentes
Bolivar
Belinda
Bances
Swisher Int’l Bering
Pléiades
Table 3
Large cigars and cigarillos, United States, 1996. Market share, company by
company, millions and percent
Company Units Percent
Swisher Int’l, Inc. 758 24.5
Havatampa 720 23.3
Consolidated Cigar 634 20.5
Culbro (General Cigar) 527 17.1
Middleton 310 10.0
M & N Standard Cigar 47 1.5
House of Windsor 30 1.0
Others 64 2.1
Total 3,090 100.0
Sources: Data on market share, Maxwell, 1997. Data on total U.S. consumption, USDA, 1997.

Chapter 7
200
Table 4
Little cigars, United States, 1996. Market share and leading brands, company by
company, millions and percent
Company Units Percent
Swisher Int’l Inc. 632 42.4
Swisher Sweets Little
Consolidated 340 22.8
Dutch Treats
Tobacco Exporters Int’l 316 21.2
Winchester
Havatampa, Inc. 139 9.3
Omega
Between the Acts
Madison
Hav-a-tampa
Lane Limited 76 5.1
Captain Black
House of Windsor 1 0.1
Little Nippers
Change in Inventory (14) (0.9)
Total 1,490 100.0
Source: Maxwell, 1997.
Table 5
Cigar companies that also manufacture tobacco products that are regulated by the
Food and Drug Administration
Company Regulated Products
Commonwealth Brands Cigarettes
Cigarette tobacco
Consolidated Cigar Cigarette tobacco
Finck Cigar Smokeless tobacco
Lane Limited Cigarette tobacco
Red Lion International Cigarette tobacco
Smokeless tobacco
Nat Sherman Cigarettes
Pinkerton Group Smokeless tobacco
Swisher International, Inc. Smokeless tobacco
UST Smokeless tobacco
Sources: Smoke 2(1):40-41, Winter 96/97; Tobacco Reporter, 1996; UST Annual Report.
Smokeless tobacco includes oral snuff.

201
Smoking and Tobacco Control Monograph No. 9
Table 6
Measured media spending for cigars, United States 1994, 1995, 1996
(first 9 months for ’96), $000’s
Company 1994 1995 1996
(9 months)
CULBRO CORP. (General Cigar)
General Cigar 60 42 n/a
Garcia Y Vega n/a n/a 24
Macanudo 234 1,503 1,597
Partagas 375 689 134
DAVIDOFF OF GENEVA, INC.
Davidoff Cigars 128 249 230
MACANDREWS & FORBES HOLDINGS (Consolidated Cigar)
Don Diego n/s 83 406
H Upmann 96 187 366
Te-Amo 193 104 303
RICHEMONT AG
Dunhill n/a 30 173
Winchester Little Cigars 107 54 150
SWISHER INTERNATIONAL INC.
Swisher Sweets Little Cigars n/a 121 296
THOMPSON CIGAR CO.
Thompson Cigars n/a 277 n/a
TRIPLE C ACQUISITION CORP.
Consolidated Cigars n/a 111 287
Total 1,193 3,450 3,966
Source: Leading National Brands, 1997.
other ways; for instance, by evoking a romantic vision of pre-revolutionary
Cuba. Many ads create a personal link with the company owners, founders,
or the artisans and the farmers who create the product and its raw material.
Some advertising seeks to expand the market for cigars by legitimizing
new users and new settings for use. The former is illustrated by the ads
which invite women to smoke cigars. An example of the latter is an ad
for a brand sold by U.S. Tobacco International, Don Tomás (U.S. Tobacco
International, 1997). The ad shows a man dressed in a terry cloth robe,
holding a coffee cup, smoking a cigar. The ad copy reads,
What time of day should you light up a cigar? We know
people who wouldn’t think of having their first cup of caffe latte
without firing up a good cigar. Then there are the traditionalists
who wait until the after dinner single malt is served to light up
their handmade Don Tomás Presidentes. When you really get
down to it, as long as the label says Don Tomás you’re in for
a treat, day or night.(p.253)

Chapter 7
202
Just by asking the question, U.S. Tobacco International legitimizes an
expansion of when cigars are smoked, especially by people who think of
themselves as not being bound by tradition. Smoking cigars with morning
coffee is not in exchange for consumption later in the day. Like promoting
soft drinks as a breakfast beverage, it is a marketing tactic which is aimed at
expanding the market.
Sexuality permeates many of the ads (Figure 2), and it can be especially
blatant in ads from some of the smaller companies. An ad for a 3.5 inch-long
cigarillo shows an attractive couple having a good time, each holding the
product. The copy reads, “For the women who say size doesn’t matter,
and the men who actually believe them” (Caribbean Cigar, 1997, p. 33).
Some ads work at a more sophisticated level. An ad for Macanudo,
which is part of a “campaign aimed at younger adult smokers” (Culbro
Corporation, 1996, p. 5), shows an attractive woman and a handsome older
man, both holding cigars and looking directly at the camera. The headline
reads, “And they thought you’d have nothing in common.” The copy creates
suggestions of professional tension and competition between the two, but
their cigars create an affirming bond that is “to be shared like wit. To be
savored like wisdom” (Cigar Aficionado, May/June 1997a, p. 9).
Figure 2
Sexuality in cigar advertisements

203
Smoking and Tobacco Control Monograph No. 9
PROMOTION By far the most important ways cigars have been presented to the
public have been through various promotional activities.
Lifestyle The resurgence of cigar use in the United States has been closely
magazines associated with the glossy lifestyle magazine, Cigar Aficionado, published
by Marvin R. Shanken. Launched in the Fall of 1992, the magazine was
targeted for what Shanken asserted was an increasing number of men who
enjoy smoking expensive cigars (Shriver, 1992). The publication has grown
from 130 pages per issue to more than 400 and has increased its publication
frequency from four to six times annually. Its circulation has grown from
40,000 (Conrad, 1996) to 400,119 (New York Times, 1997. Each issue
promotes cigar use as part of successful, indulgent living through interviews
with celebrities, sports stars, and others. Reviews of expensive cigars are
offered as well as lavish descriptions of cigar accessories such as lighters and
humidors. The editorial context is how to live life to the fullest in a style
reminiscent of Esquire, GQ or Playboy. While advertising for cigars and their
perquisites are prominent, sellers of upscale clothing, luxury cars, expensive
watches, jewelry, premium liquor, casinos, other resorts, and perfume also
feature their goods and services in this publication. Each issue has an article
about gambling.
Cigar Aficionado has launched a line of clothing and accessories named for
the magazine. A Cigar Aficionado branded fragrance for men was promoted in
time for holiday shopping (Washington Post
Magazine, 1998) (Figure 3)
Most cover stories feature profiles of
prominent people whose cigar use is illustrated on
the cover and described in the accompanying
article (Table 7) (Figure 4).
Articles romanticize Actor James Woods (Figure 5) told
cigar smoking his interviewer, “When you smoke
a cigar, time stops. And you can sort out your
thoughts. Contemplate. You can just kind of
hold it and puff it and just drift down the stream
of your thoughts for an hour or so. Thank God
for cigars. At least there is one place where I can
be quiet for a moment and actually be alone with
my thoughts” (Cigar Aficionado, 1997b, p.147,
149). There are also frequent defiant comments
about cigars in reaction to what are depicted as
puritanical or radical emblems in the culture.
Woods remarked, “Cigar smoking is the kind of
thing a feminist would whine about. . . .And
that’s a good thing” (Cigar Aficionado, 1997, p.144).
A feature story on Claudia Schiffer (Figure 6) opens with an indignant
blast at dissipation and drug use in the modeling profession:
Source: Washington Post
Magazine, 1998
Figure 3
Cigar Aficionado
fine
fragrance

Chapter 7
204
Table 7
Persons featured on covers of
Cigar Aficionado
and
Smoke
, 1993 - Winter 1998
Year Persons
Cigar Aficionado
1993 Groucho Marx
Winston Churchill
1994 Rush Limbaugh
Fidel Castro
Bill Cosby
George Burns
1995 Ron Perelman
Jack Nicholson
Linda Evangelista
Tom Selleck
1996 Matt Dillon
Arnold Schwartzenegger
Demi Moore
Danny Devito
1997 Wayne Gretzky
Janet Jones
James Woods
Claudia Schiffer
Michael Richards
1998 Denzel Washington
Smoke
1996 Pierce Brosnan
Tom Arnold
Red Hot Chili Peppers
Mel Gibson
1997 Elle Macpherson
Jeff Goldblum
Carmen Electra
Claudia Schiffer is talking tough. There’s a problem in the
world of fashion these days, she says — the fact that too often
models have to look like junkies just to be cool. “I think fashion
should be promoting beauty and health,” she says. “That doesn’t
happen if the model looks anorexic, unhealthy, tired, if the
photography makes her look as if she’s on drugs or been out
partying all night. That kind of thing can end up hurting young
women or girls who feel they have to imitate the models they see
in the magazines. That’s not what fashion is about. For me,
fashion is about beauty.” (Rothstein, 1997, p. 170)
The article and magazine cover include seven large photos of the
supermodel cum cigar in alluring poses (Rothstein, 1997). The contrast being
drawn between drug use and dissipation on the one hand and cigar use on the
other could not be more clear.
205
Smoking and Tobacco Control Monograph No. 9
Figure 4
Jack Nicholson, Matt Dillon, and Bill Cosby
The magazine has created a following. Readers send in
photographs of themselves and their cigar-related activities.
Several pages have been devoted to photos of readers showing
off cigar-related vanity license plates (Photo Gallery, 1997a;
Photo Gallery, 1997b).
From time to time, the
publisher takes on criticisms of
cigar use in the editorial he writes
for each issue, taking the
Environmental Protection Agency
(EPA) report on environmental
tobacco smoke and the proposed
Occupational Safety and Health
Administration (OSHA) rule on
tobacco smoke in the work place to
task (Shanken, 1993; Shanken,
1997c), issuing a call to action
against the “new Prohibition” in another
(Shanken, 1994), and expressing sharp
disagreement with critics of cigar use as indulging
in “scare tactics” in another (Shanken, 1997a).
Within days of the announcement from the
Centers for Disease Control that surveys show that
kids now frequently use cigars (Kaufman et al.,
Figure 5
James Woods
Source: Cigar Aficionado,
May/June 1997
Figure 6
Claudia Schiffer
Source: Cigar Aficionado,
August 1997
Source: Cigar Aficionado, Summer 1995, Spring 1996, and Autumn 1994.

Chapter 7
206
Source: Cigar Aficionado,
Spring 1993
Figure 7
Ear, nose, and throat
surgeon
1997), posted a column on the magazine’s web page proclaiming that cigars
are for adults only and not for teenagers (Shanken, 1997b). He has blasted
the American Cancer Society for publishing
public service ads about cigars and Brooks
Brothers for stopping the use of cigars as props for
models in its advertising (Shanken, 1997d).
The posture taken is that the occasional, non-
inhaled, moderate use of cigars is OK even though
potentially serious problems can sometimes arise
when cigar use is outside of these parameters.
The studied reassurance the magazine offers has
been reinforced by a column written by a cigar-
loving Ear, Nose, and Throat (ENT) surgeon, who
was photographed in surgical scrubs holding a
cigar (Pearlman, 1993) (Figure 7). A similar image
was evoked in a photograph which illustrated an
article on cosmetics and cosmetic
surgery for men. A plastic surgeon
posed in a white lab coat, holding
a cigar (Wolfson, 1997) (Figure 8).
The periodical has not only
been sanctioned by physicians, it
has been blessed by a person of the
cloth. In its second issue, the magazine published a letter from
an anonymous member of the clergy, who praised the new
publication and reflected on the importance of a cigar in
composing sermons. “In moderation, ten a week or so, cigar
smoking, I declare, is not a sin. Gentlemen, you have my
blessings. Those who do like the art and transcendental
experience of smoking a fine cigar need not worry of divine
retribution. I think God understands” (An inspired preacher,
1992).
By 1996, the success of Cigar Aficionado spawned imitation
from a tobacco trade publisher, Lockwood, in the form of
Smoke, whose subtitle is “Cigars, pipes and life’s other burning
desires.” It, too, has seen an increase in pages, from 182 in the premier issue
to 464 in the Summer 1997 issue. Smoke, which seems targeted at a
somewhat younger, more hip audience, has a similar mix of cigar features
and general lifestyle articles. Its covers also feature celebrities smoking cigars
(Table 7) (Figure 9). Another similar magzine, Cigar Monthly, has featured
various cover stories (Figure 10).
These three publications have been imitated in France (French Toast,
1996). In keeping with the style of its American cousins, the cover of the
March 1997 issue of L’Amateur de Cigare features General Charles de Gaulle
with a cigar.
Figure 8
Cosmetic surgeon
Source: Cigar Aficionado,
March/April 1997

207
Smoking and Tobacco Control Monograph No. 9
Figure 9
Mel Gibson, Carmen Electra, Jeff Goldblum, and Elle Macpherson
Source: Smoke, Anniversary Issue Winter 1996-1997, 2nd Anniversary Issue Winter 1997,
Summer 1997, and Spring 1997
Figure 10
Cigar Monthly
cover stories
Source: Cigar Monthly, April 1995,
November 1995, March
1996, July 1996, 1997

Chapter 7
208
The hedonistic themes these magazines explore are captured in the
concluding exchange from an interview published in Smoke with actress Kim
Cattrall (Cattrall, 1996).
Q. What do you think all the buzz is about cigars?
A. It’s a very large phallic symbol that men like to play with — and women
like to watch them. I understand the attraction. Just holding one, there’s
sort of a power related there.
Cigar-centered The current era of fancy cigar dinners and other entertainments
Dining and focused on cigars seems to have begun around 1988 (Luz, 1997).
Entertainment
From its own beginnings four years later, Cigar Aficionado
sponsored gala affairs and dinner parties at expensive restaurants featuring
cigars, wines, and celebrity guests. Similar events, which build word of mouth
advertising, have become widespread, and the magazine publicizes restaurants
that offer “smoker nights.” In a 1992 issue, there was a list of 32 domestic
and 4 foreign restaurants and cigar clubs that offered such events (Smoker
Nights, 1992); by Spring 1997, the number of listings had grown to 591
entries in the United States and 70 listings from outside the country (Smoker
Nights, 1997). Magazine subscribers receive formal invitations to events
sponsored by the magazine, and the magazine regularly features photographs
from these events in its pages. The popularity and acceptability of these
events is illustrated by the fact that a restaurant at Walt Disney World has
hosted cigar dinners (Scott, 1996a).
Sometimes, these events are linked to charitable causes. In New Jersey,
cigar nights have provided fund-raising settings for the Women’s Center of
Monmouth County, the Make-A-Wish Foundation of New Jersey, the Easter
Seal Society of New Jersey, and the Cerebral Palsy Association of Middlesex
County (Henderson, 1996; Henderson, 1997a; Henderson, 1997b; Robert
Kucharski, personal communication, June 5, 1997). An event called
“Celebrity Smoke ’97,” sponsored by Smoke, was produced by Celebrity
Fund-raisers, Inc. and benefitted a charity called The Miami Project (Celebrity
Smoke ’97, 1997). A $1,000-per-ticket cigar dinner and viewing of the film
“Napoleon” (accompanied by a 65 piece orchestra) is to benefit the Culinary
Institute of America at Greystone and the North Beach Homeless Project of
San Francisco (Coppola and Shanken, 1997).
In October 1994, Cigar Aficionado sponsored a dinner in Paris called the
“Dinner of the Century” (Nights to Remember, 1994). Formal invitations for
the event indicated that a portion of the ticket price would be donated to the
United Nations Children’s Fund (UNICEF). When the director of UNICEF was
informed of this unsolicited and unwanted association, an attorney for
UNICEF put the organizers on notice that they were to stop using the name of
the children’s fund in association with the dinner. Instead, a donation was
made to CaP Cure, a charity for prostate cancer research (Ron Davis, personal
communication, October 1994).

209
Smoking and Tobacco Control Monograph No. 9
Adding a charitable dimension to these events may add a sense of
mainstream mission, purpose, and respectability to what may simultaneously
be regarded as daring, flaunting of convention, and even somewhat
underground. Not only is a cigar dinner fun for itself and more so for
being a bit of a slap at puritanical attitudes, it can also be for a good cause.
Scott, writing in a trade magazine for retail tobacco shops, has described
how to organize a cigar dinner.
Cigar dinners, if planned and executed well, are an excellent
way to build your business. They work best as a promotional tool,
just like advertising. The nice thing about them, as a business
builder, is they can be operated at a break-even level. What other
advertising medium do you use that costs you nothing? The dealer
who thinks he can make a profit on cigar dinners, however, will
probably find his dinners, non-competitively priced, won’t yield
the results he wants. (Scott, 1996a, p.44)
Ed Kotoch, owner of the Tobacco Road stores in Las Vegas, says,
“Instead, think of a cigar event as a way to get to know your
customers better, especially the ones who just breeze in and out of
your store; or to meet your customers’ cigar-smoking friends whom
they bring to the dinner; or to say ‘thank you’ to a few selected and
valued customers.” (Scott, 1996a, p. 44)
The article offers detailed advice on planning, organizing, and conducting
these events. A balanced blend of entertainment, food, wine and cigars is to
be sought. Cautioning against seeking venues in restaurants owned by non-
smokers, Scott advises making sure that ventilation is adequate and even
providing additional air filters because, he notes, “cigars put out a lot of
smoke” (Scott, 1996a, p. 46). In selecting cigars for the evening, he suggests
a mix of full-bodied and mild cigars. He especially suggests
providing a selection of smaller, mild cigars for women so that
they can more easily participate in the revelry. For a ticket
price of $75-$90, Scott suggests a budget of $20-$25 for food,
$5 for tips, $15 for cigars, $10 for a gift, $15-$20 for drinks,
$5 for invitations, and complimentary tickets for the dinner
speaker and the people who represent the cigar and beverage
distributors.
Entertainments such as these serve to further embed cigar
use in the culture, socialize people to the use of cigars, and
teach novices how to use them. The luxurious settings foster
the high-class image with which the cigar industry seeks to
associate itself. In Augusta, Georgia, Mike Smith, proprietor
of Cigar Affairs, hosts cigar dinners, such as the Spring Big
Smoke (Barshafsky, 1997) (Figure 11).
Sanctioned social clubs organized around cigars have
appeared on a number of major college campuses (Barry,
1997).
Figure 11
Augusta
Source: Augusta,
September 1997

Chapter 7
210
Smoking clubs appeared in many communities in the mid-1990s.
Among the most elaborate are cigar bars identified with Macanudo brand
cigars, the Club Macanudo in Chicago and in New York (Club Macanudo,
1997). At the New York club, which offers patrons a cigar school for initiates,
a large painting of the bar hangs in the dining room. The painting features
Culbro executives Edgar M. Cullman, Sr. and his son, Edgar M. Cullman, Jr.,
as well as Marvin Shanken surrounded by famous people who smoked cigars.
Winston Churchill and John F. Kennedy are joined by Madonna, Whoopi
Goldberg, Michael Jordan, Julie Andrews, Linda Evangelista, Richard Pryor,
Jack Nicholson, Robert deNiro, Orson Wells, and Bruce Willis. Patrons are
offered menus for both food and cigars. Culbro products are featured in great
variety with prices ranging up to $40, but there are also a few offerings of
lesser quality from other major purveyors. Among the holders of humidors
at the Club are a number of New York-based magazines, including Esquire,
Vanity Fair, Business Week, Sports Illustrated, U.S. News and World Report, and
Golf Digest.
Retail establishments devoted to smoking seem in part a reaction to the
elimination of smoking from more and more indoor spaces. The fashion
brings to mind the early history of smoking in 17th century England where
customers would leave their pipes at the local tobacco shop. They would
come to the shop not just to purchase tobacco but to smoke as well.
Newspaper The resurgence in popularity of cigars has been covered, and in part
stories about fueled by, articles in newspapers. Among the twenty daily newspapers
cigars indexed by the Dialog data base, there were 325 articles over the seven-
year period 1990 - 1996 that dealt with news about cigars or feature stories
about their increasing popularity in the culture. Coverage of cigars was fairly
constant for the first 5 years of the period, and then showed an abrupt
upswing (Table 8). Uncritical stories describing this as a social or as a fashion
phenomenon have been common in newspapers as well as on television
magazine shows. Much of this coverage was stimulated by a public-relations
effort by cigar manufactures intended to promote positive stories in the news
media linking cigar use to luxury and power (Klein, 1998).
A highly successful race horse named Cigar (Figure 12) appeared on the
sports pages beginning in May 1995 with a victory at Pimlico. The horse
was featured in 103 stories in these same twenty newspapers in 1995 and
in 212 stories the following year.
Women and Cigar smoking by women has been one of the sub-themes of cigar
cigars publicity. Celebrity women and their cigars have frequently been
featured in the cigar magazines (Figure 13). Madonna smoked a cigar on
the David Letterman show in 1994 (Conrad, 1996). Feature stories in
newspapers, popular news magazines, and on television have highlighted
this as a new trend (Figure 14). A recent book describes and explains cigar
smoking for women (Edmark, 1995), and a retail trade magazine has
published an article on how to “capitalize on the marketing differences
the gender gap provides” (Ashley, 1997b, p. 162). These phenomena increase
the visibility not only of women smoking cigars, but of cigar use itself.

211
Smoking and Tobacco Control Monograph No. 9
Table 8
News and features about cigars. Twenty daily newspapers Indexed by Dialog
1990-1996
Year Number of articles
1990 23
1991 19
1992 20
1993 36
1994 24
1995 81
1996 122
Total 325
Source: Dialog
Internet Cigars are featured on the
advertising world wide web at many
and promotion sites (Mason, 1996).
There are online catalogs for
ordering as well as links that
provide background information
and ratings. Both cigar lifestyle
magazines maintain elaborate sites.
One site sponsored “Operation
Cigar Lift” for U.S. troops stationed
in Bosnia in 1996 (Smoke Signals,
1996).
Ashley has
described the ins and outs of
setting up and running a web site
for people in the retail cigar
business (Ashley, 1997a). He
describes how selling on the
Internet has transformed the way
a number of retailers operate, with
some now providing frequent
updates of their inventories online.
Websites for cigars may receive
tens of thousands of visits
monthly. The sites operated by
manufacturers not only provide
information and images about
specific brands but also link
customers with retailers who carry
the products. There are discussion
groups and news groups as well on
Figure 13
Demi Moore
Source: Cigar Aficionado,
Autumn 1996
Figure 12
The race horse, Cigar
Source: Cigar Aficionado, Winter 1996/1997
Figure 14
Jenny McCarthy
Source: Newsweek, July 21,
1997

Chapter 7
212
these sites. Sites also can offer search capabilities to people looking for
particular products or product characteristics.
Catalogs and Cigars have long been available by mail order, but the resurgence
cigar-related in popularity of expensive cigars has prompted the introduction of
items new specialty catalogs for cigar users such as one called The Cigar
Enthusiast. Accessories for cigars have begun appearing in more established
upscale catalogs such as those from Herrington, Frontgate, Huntington
Clothiers, and Hammacher Schlemmer.
The cigar craze has nourished the cottage industry that produces cigar
accessories such as lighters, cutters, ashtrays, and humidors. Oddities such
as devices which provide a place to put a lit cigar on a golf
course while the user takes a shot have appeared on the
market. A “breath cleanser” for cigar smokers is being sold
(Cigar Clear, 1996). New cigar-themed clothing companies,
selling silk screened whimsy or classical cigar art (based on
cigar box paintings and cigar bands) have appeared: The Five
Cent Cigar Co., Smoke Rings, and The Original Cigar Clothing
Company. The Nat Sherman Catalog (Figure 15) offers a
variety of cigar accessories (Figure 16)
Books (Hacker, 1996; Shanken,
1996), videos (Dees, 1996),
lithographs (Mazur, 1996), and
even compact discs related to cigars
(Schmorr, 1996) have appeared on
the market. One of these books
includes a curiously lighthearted
chapter on health effects (titled
“But will they stunt your growth?”)
which emphasizes the supposed
advantage of cigar tobacco having
fewer additives and the fact that
inhalation is optional with cigars
(because nicotine absorption from
cigar smoke, unlike that from
cigarette smoke, does not depend
on inhalation) (Scott, 1996b).
Dunhill has long offered high-end men’s
clothing and accessories in association with its
core tobacco products business.
Virtually alone among the major cigar
companies, General Cigar has borrowed other
marketing techniques prominent in the cigarette
industry for some of its mass-market cigars as well
(Coeytaux, Altman and Slade, 1995; Altman,
Levine, Coeytaux, Slade and Jaffe, 1996). General
Cigar has run a series of promotions for its White
Figure 15
The Nat Sherman Catalog
Source: Nat Sherman Catalog,
1998
Figure 16
Cigar accessories –
The Nat Sherman Catalog
Source: Nat Sherman Catalog,
1998

213
Smoking and Tobacco Control Monograph No. 9
Owl and Garcia y Vega brands which involve returning proofs of purchase for
branded t-shirts and other premiums. It has even developed a small catalog
for the Garcia y Vega brand. Moreover, General Cigar has launched a line of
expensive sportswear geared to its premium brands (Culbro Corporation,
1996). It also plans a branded line of cigar smoking accessories (Smoke
Signals, 1997). The president of the parent company, Edgar M. Cullman, Jr., is
quoted in the annual report as saying, “General Cigar’s brand extensions in
new classic sportswear set the stage for our lifestyle-driven company of
tomorrow” (Culbro Corporation, 1996, p. 8).
There have been other sporadic, small efforts at promoting mass-market
cigars, but generally, the makers of these products have not devoted large
amounts of money to their promotion in recent years. Swisher International
briefly supported a NASCAR race team for Swisher Sweets, and the makers of
the little cigar Winchester published booklets of football and baseball statistics
and schedules in 1995 that were distributed through some retail outlets.
Sportswear for Macanudo does not imitate the understated elegance of
Dunhill. Instead, Culbro features the Macanudo name prominently on each
article of clothing, so the caps, sports shirts, jackets, and sweatshirts are
themselves advertisements for the brand in much the same manner that
cigarette companies promote their brands through promotional items.
Among the ways General Cigar seeks to promote Macanudo is through
furniture. The William Allen Company of High Point, North Carolina offers
two stuffed armchairs retailing for about $2,500 each which feature the
Macanudo crest design on the upholstery. A leather chair has the crest on a
kidney pillow and the seat deck, while a mohair chair has it on the seat
cushion (William Allen, 1997). On introducing these products to a furniture
store, the Allen salesman passes out cigars and offers a $700 Macanudo
smoking jacket for sale as well.
Borrowed glory Cigars have become a common prop, on magazine covers (Mott,
1992) (Figure 17), in fashion photography, for men’s accessories such as ties,
and among popular musicians, movie stars and other
celebrities. A popular history recounts many of the famous
names, past and present, associated with cigars (Conrad, 1996).
The cigar may be intended to be provocative or to project
“power, authority and self-confidence” (Mott, 1992, p. 46).
When the Chicago Bulls won the NBA championship in 1996,
Michael Jordan and Dennis Rodman celebrated with cigars, and
their smoking was widely seen on television. George Dessart of
the American Cancer Society criticized these sports stars,
saying, “By displaying these cigars at the moment they were the
most visible athletes in the world, Michael Jordan and the
Chicago Bulls served as the worst type of role model for
millions of children worldwide. After all, if Michael Jordan and
the Chicago Bulls smoke, it must be cool and it can’t be that
bad for you” (Campaign for Tobacco-Free Kids, 1996).
Source: The New Yorker,
September 23, 1996
Figure 17
The New Yorker

Chapter 7
214
At least some of the gratuitous public cigar display so evident in recent
years may be because of commercial sponsorship. In the 50’s and 60’s,
celebrities such as Ernie Kovacs, Danny Thomas, and Sid Caesar did
commercials for Dutch Masters,
1
and Edie Adams cooed “Pick me up and
smoke me sometime” for Muriel (Kiersh, 1997, p. 105). George Burns smoked
another machine-made brand from Consolidated Cigar, El Producto Queens,
exclusively for many years. Each month, he
received 300 of the stogies from the manufacturer
for free. While it is not known if he also received
an honorarium or a sponsorship fee in addition to
the free cigars, he repeatedly refused to even try
any other brand (Kiersh, 1997). Consolidated
Cigar is trying to capitalize on this long-standing
association by creating a special series of El
Producto cigars it is calling the “George Burns
Collection” (Kiersh, 1997). It is not known if this
venture involves the payment of a licensing fee to
the Burns estate, but such considerations are
common for other products.
Cigars and Cigars have become a common prop in movies
the Movies (Independence Day, 1996; Batman and Robin,
1997). In at least one case, though, the cigars
featured in advertising were not apparent in the
movie itself. Ads for the 1996 movie The First
Wives Club (Paramount) showed Goldie Hawn,
Diane Keaton and Bette Midler
with stogies (Figure 18) while in
both the movie itself and the book
on which the movie was based,
these characters never used cigars
(Thomas, 1996). When the HBO
movie Weapons of Mass Distraction
was advertised in Cigar Aficionado,
the characters held cigars (Cigar
Aficionado, 1997c) (Figure 19).
When the same movie was
advertised in The New Yorker, the
characters’ hands were empty
(New Yorker, May 19, 1997)
(Figure 20). Cigar manufactures
paid Hollywood brokers to feature
their products in movies including
Independence Day (Klein, 1998).
Source: Cigar Aficionado, May/
June 1997
Figure 19
Weapons of Mass
Distraction–with cigars
Source: The New Yorker,
May 1997
Figure 20
Weapons of Mass
Distraction–without cigars
Source: Fairfax County TV
Guide
Figure 18
First Wife’s Club
1
This brand evokes memories of Rembrandt’s contemporaries even though tobacco was mainly
consumed in pipes throughout the low countries at that time.

215
Smoking and Tobacco Control Monograph No. 9
AVAILABILITY Inexpensive cigars are mostly sold as self-service items in grocery
stores, convenience stores and pharmacies. The growth of the premium cigar
trade has been accompanied by an increase in outlets for expensive cigars
beyond tobacconists and other specialized retailers. Major manufacturers
are seeking to expand traditional outlets for premium cigars to include
hotel shops, wine shops, restaurants, and upscale specialty and department
stores (Smoke Signals, 1997). Vending machines for premium cigars are
commercially available and have begun to appear in some locations
(Trendwatch, 1997).
DISCUSSION Cigar use began to increase after promotional activities for cigars
stepped up beginning in 1992. The cigar market was stagnant (Chapter 2)
before Cigar Aficionado was launched, even though Marvin Shanken has
said he launched the magazine in response to an increase in use of premium
cigars. In a prospectus, Consolidated Cigar Holdings attributes the increase
in cigar consumption largely to the magazine, to the use of cigars by
celebrities (Figure 21), and to the proliferation of social events that feature
cigars (Consolidated Cigar Holdings, 1996). These efforts have increased
the visibility of cigar consumption, have normalized cigar use, and have
Source: Cigar Aficionado, Spring 1993, February 1998, October 1997, Winter 1994
Figure 21
Groucho Marx, Denzel Washington, Michael Richards, and George Burns

Chapter 7
216
broken down barriers for cigars. Among the barriers that seem to have been
broken has been use by kids (Kaufman et al., 1997). These efforts have a
familiar ring. Public relations techniques to normalize and popularize
cigarette use in general and among women in particular were used by
cigarette makers earlier in the century (Kluger, 1996).
While nearly all promotional energy for cigars has been focused on
premium versions, fully 83 percent of the unit growth in the consumption of
large cigars and cigarillos has been for inexpensive, non-premium, machine-
made brands. Advertising for specific premium brands, which is directed at
expanding the market serves the dual role of promoting both cigars and a
particular brand (Montego y Cia. 1997; U.S. Tobacco International, 1997).
Moreover, despite disclaimers to the contrary (Shanken, 1997b), an inevitable
effect of fostering a somewhat outrageous fashion among adults is that its
appeal to kids will grow.
Measured marketing expenditures for cigars was only $4 million for the
first 9 months of 1996, yet the industry had more than $1.2 billion in sales.
To the extent that they exist at all, the unmeasured marketing
expenditures may be devoted to activities such as planting feature stories
about cigars in newspapers and television, securing celebrity endorsements
of cigar smoking, promoting cigar dinners, financing the expansion of retail
tobacco shops, and of restaurants, clubs and bars that encourage cigar
smoking, achieving placements in popular entertainment and in fashion
magazines, and facilitating the development of communications channels,
such as magazines, books and web sites.
It may be that individual cigar companies are working by themselves
or in concert to facilitate at least some of these public relations activities,
because the bulk of the industry is concentrated in only a few companies
(Table 3). Efforts to boost cigar use in general will mainly benefit those
companies that are already well positioned.
The more sophisticated companies, especially Culbro (General Cigar) and
Consolidated Cigar, seem to be taking integrated marketing approaches to
building franchises for their major brands. Although the use of sex and
celebrity to sell cigarettes has been forbidden by the cigarette industry’s
voluntary code since 1965, these appeals are regular features of cigar
marketing.
Additional information is needed to better characterize marketing efforts
for cigars. Specifically, there should be:
• Continued efforts to describe advertising and promotional efforts for
cigars as well as to understand the dynamics of the market and the
companies involved in it,
• Compilation of marketing expenditures for cigars as the Federal Trade
Commission already does for cigarettes and smokeless tobacco products,

217
Smoking and Tobacco Control Monograph No. 9
• A survey of prominent people who have been publicly associated with
cigar use to learn about the extent to which they have received
sponsorship fees or any other consideration from commercial cigar
interests,
• Research to learn how different segments of the public understand cigars,
especially in relationship to cigarettes. One possibility is that since cigars
are often experienced as being more acutely noxious than cigarettes, the
increased acceptability of their use may undermine public perceptions of
the harmfulness of cigarettes. The public may also have misconceptions
about the role of nicotine in cigar use. In other words, apart from the
direct toxicity of cigars, does the cigar craze undermine public health
efforts to control the cigarette epidemic?
• Research to learn which brands of cigar are popular with the young and
how marketing, price, and availability affect brand choice for this group,
and
• Research to learn the extent to which advertising and promotion for
cigars, including things as commonplace as cigar bands, reaches and
affects kids.
CONCLUSIONS
1. Cigar use began to increase in the United States after promotional
activities for cigars increased beginning in 1992.
2. Promotional activities for cigars have increased the visibility of cigar
consumption, normalized cigar use, and broken down barriers to cigar
use.
3. Although the use of sex and celebrity to sell cigarettes has been forbidden
by the cigarette industry’s voluntary code since 1965, these appeals are a
regular feature of cigar marketing.
The preparation of this chapter has been supported in part by grants
from the Robert Wood Johnson Foundation.
References
Altman, D.G., Levine, D.W., Coeytaux, R., Slade, J.,
Jaffe R. Tobacco promotion and susceptibility to
tobacco use among adolescents aged 12 through 17
in a nationally representative sample. American
Journal of Public Health 86:1590-1593, 1996.
Ashley, B. Internet frenzy: Is the web for you?
Smokeshop 24(20):66-74, March/April 1997a.
Ashley, B. Retailing cigars to women: Embracing the
nuances. Smokeshop 24(4):162-166, July/August
1997b.
Barry, S.T. Collegiate smokes. Smoke 2(2):138-150,
Spring 1997.
Barshafsky, D. The Big Smoke, Augusta, August/
September 1997.
Bennet, J. From Chelsea Clinton’s dad, pithy advice
for graduates. The New York Times, p. 1, June 7,
1997.
Campaign for Tobacco-Free Kids. Press release,
17 June 1996.
Caribbean Cigar, Company Advertisement for
Alternatives Cigars, Smoke 2 (2):33, Spring 1997.
Cattrall, K. Live nude girl? Smoke 1(2):134-5, Spring
1996.
Celebrity Smoke ’97. Smoke 2(2):354, Spring 1997.
Cigar Aficionado, 5(4):9, May/June 1997a.
Cigar Aficionado, 5(4):124-149, May/June 1997b.
Cigar Aficionado, 5(4):113, May/June 1997c.
Cigar Clear. Smoke 2(1):168, Winter 1996/97.

Chapter 7
218
Club Macanudo. Savor the good life. Cigar Aficionado
5(4):56, May/June 1997.
Coeytaux, R.R., Altman, D.G., Slade, J. Tobacco
promotions in the hands of youth. Tobacco Control:
An International Journal 4(3):253-257, 1995.
Conrad, B., III. The Cigar. San Francisco: Chronicle
Books, 1996.
Consolidated Cigar Holdings Inc. Prospectus for the
sale of 5.4 million shares of Class A Common Stock
(par value 0.01 per share), August, 15 1996.
Coppola, F.F., Shanken M.R. Advertisement for
“Napoleon” dinner. Cigar Aficionado 5(5):22, August
1997.
Culbro Corporation. 1995 Annual Report. New York:
Culbro Corporation, 1996.
Dees, R. Cigars! The New Rage! video. Advertised in
Smoke 2(2):239, Spring 1997.
Dialog file 483: Newspaper abstracts daily UMI, 1990-
1996,
Edmark, T. Cigar Chic: A Woman’s Perspective.
Arlington, TX: The Summit Publishing Group, 1995.
Federal Trade Commission. Report to Congress Pursuant
to the Federal Cigarette Labeling and Advertising Act.
Washington, D.C.: Federal Trade Commission,
1996.
Federal Trade Commission. Report to Congress Pursuant
to the Comprehensive Smokeless Tobacco Health
Education Act of 1986. Washington, D.C.: Federal
Trade Commission, 1997.
Finora, J. Bullish on cigars. Smokeshop 24(4):168-176,
July/August 1997.
Flying High. Smokeshop 24(4):122-138, July/August
1997.
Food and Drug Administration. Nicotine in cigarettes
and smokeless tobacco is a drug and these products
are nicotine delivery devices under the federal Food,
Drug, and Cosmetic Act: Jurisdictional
determination. Federal Register 61(168):44619-
45318, August 28, 1996.
French Toast. Smoke 2(1):36, winter 1996/97.
Hacker, R.C. The Ultimate Cigar Book. (2nd edition).
Beverly Hills, CA: Autumn Gold, 1996.
Henderson, M. Cigar fans puff away for Make-A-Wish.
Asbury Park Press, June 18, 1996.
Henderson, M. Stepping out. Asbury Park Press, January
5, 1997a.
Henderson, M. Night of cigars and food to benefit
Easter Seals. Asbury Park Press, January 14, 1997b.
Inspired preacher. Out of the humidor (letter to the
editor). Cigar Aficionado 1(2):9, Winter, 1992/93.
Kaufman, N.J., Emont, S.L., Trimble, C.R., Orleans,
C.T., Briton, N., Clark, T., Krakow, M., Celebucki, C.,
Cullen, D., Connolly, G., Hyland, A., Perla, J.,
Cummings, K.M., Abdella, A., Tippens, K. Cigar
smoking among teenagers — United States,
Massachusetts, and New York, 1996. Morbidity and
Mortality Weekly Report 46(20):433-440, May 23,
1997.
Kiersh, E. Saving El Producto. Cigar Aficionado
5(3):96-107, March/April 1997.
Klein, A. The Cigar Caper: the shaping of an illusion and
cigar-changing Hollywood heroes. The Sun, January 11-
13, 1998.
Kluger, R. Ashes to Ashes: America’s Hundred-year
Cigarette War, the Public Health, and the Unabashed
Triumph of Philip Morris. New York: Alfred A.
Knopf, 1996.
Luz, M. Putting your money where your smokes are.
Smoke 2(3):376- 380, Summer 1997.
Mason, S. Cigar smokers in...cyberspace. Smoke
1(1):48-51, 1996.
Maxwell, J.C., Jr. The Maxwell Consumer Report: The
Cigar Industry in 1996. Richmond, VA: Wheat First
Butcher Singer, March 21, 1997.
Mazur, R. Ruby Mazur’s cigar art. Smoke 2(1):39,
Winter 1996/97.
Montego y Cia. Advertisement for Macanudo cigars.
Cigar Aficionado 5(4):8-9, May/June 1997.
Mott, G. “It’s about freedom and pleasure”:
Marketers and editors look to cigars to make
statements. Cigar Aficionado 1(2):46-49, Winter 92/
93.
The New Yorker, May 19, 1997, p. 9.
New York Times, April 30, 1997. P. 12.
Nights to Remember. Cigar Aficionado 3(2):304-306,
December 1994.
Pearlman, M.H. A doctor’s view. Cigar Aficionado
1(3):130, Spring 1993.
Photo Gallery. Cigar Aficionado 5(4):33, May/June
1997a.
Photo Gallery. Cigar Aficionado 5(5):35, August 1997b.
Smoke 2(1):40-41, The ultimate guide to some of the
world’s finest cigars. Pinkerton Group, Inc., Winter
1996-97.
Rothstein, M. The golden girl. Cigar Aficionado
5(5):168-189, August 1997.
Schmorr, J. Whistle while you work. Smoke 2(1):38,
Winter 1996/97.
Scott, D. Eat, smoke, and be merry: The truth behind
cigar dinners. Smokeshop 23(3):44-49, May/June
1996a.
Scott, D. How to Select and Enjoy Premium Cigars...and
Save Money! Julian, CA: Coast Creative Services,
1996b.
Scott, D. Buying from independent reps. Smokeshop
24(4):218-230, July/August 1997.
Shanken, M.R. The real story. Cigar Aficionado 1(3):5,
Spring 1993.
Shanken, M.R. A big smoke in our nation’s capital.
Cigar Aficionado 3(2):19, Winter 1994.
Shanken, M.R., editor. Cigar Aficionado’s World of
Cigars. Philadelphia: Running Press, 1996.
Shanken, M.R. Scare tactics. Cigar Aficionado 5(4):19,
May/June 1997a.
Shanken, M.R. Cigars are not for teenagers. http://
www.cigaraficionado.com, May 1997b.

219
Smoking and Tobacco Control Monograph No. 9
Shanken, M.R. Bad science, bad laws. Cigar Aficionado
5(5):21, August 1997c.
Shanken, M.R. Selected weekly wrappers. Cigar
Aficionado 5(5):40, August 1997d.
Shriver, J. Cigar buffs take puffs with pride. USA Today
D1, 26 May 1992.
Smoker Nights. Cigar Aficionado 1(2):125, Winter 1992/
93.
Smoker Nights. Cigar Aficionado 5(4):420-431, May/June
1997.
Smoke Signals. Bits and pieces. Smokeshop 23(6):12,
November/December 1996.
Smoke Signals. Strong stock debut for General Cigar
IPO: Manufacturer charts course for future expansion.
Smokeshop 24(2):18, 1997.
Thomas, K. Lighting up: Tobacco has a role in most
movies. USA Today 17 November 1996, p. 1D.
Tobacco Reporter. 1997 Global Tobacco Industry Guide.
Raleigh, NC: SpecComm International, 1996.
Trendwatch. Vending humidors: Retail opportunity
or high-profile competitor? Smokeshop 24(2):32,
March/April 1997.
U.S. Department of Agriculture. Tobacco Situation and
Outlook Report. Washington, D.C.: USDA,
Economic Research Service, TBS-238, April 1997.
U.S. Tobacco International. What time of day should
you light up a cigar? Cigar Aficionado 5(3):253,
March/April 1997.
Wall Street Report. Cigar Insider 2(6):10-11, June 1997.
Washington Post Magazine, November 30, 1998, p. 48.
William Allen Company Catalog. High Point, NC:
William Allen Company, 1997.
Wolfson, N. About face: Cosmetic surgery and facial
products are not just for women anymore. Cigar
Aficionado 5(3):308-321, March/April 1997.

221
Smoking and Tobacco Control Monograph No. 9
Policies Regulating Cigars
Gregory N. Connolly
A number of Federal and State policies cover tobacco products. Table 1 presents
the Federal policy approach to the different forms of tobacco use. Table 2 pre-
sents the policy approaches of the State level. In general, Cigars are exempted
from many of the regulations that apply to other tobacco products, particularly
at the Federal level.
REGULATION OF In 1906, Congress passed the first Federal Food and Drug Law. The
CIGAR PRODUCTS Act defined medicines and preparations recognized in the United
States Pharmacopoeia (USP) or the National Formulary. Tobacco was listed in
the 1890’s edition but purportedly was deleted in the 1905 edition in exchange
for support from tobacco-state congressmen for passage of the law (Neuberger,
1963). The 1906 act was superseded by the Federal Food, Drug and Cosmetic Act
(FFDCA) passed in 1938 (Neuberger, 1963). The Act revised the definition of
drug to also include “articles intended for use in the diagnosis, care, mitigation,
treatment or prevention of disease in man or animal” and “articles (other than
food) intended to affect the structure or any function of the body of man or
other animals.”
In 1960, the Food and Drug Administration (FDA) received new authority to
regulate consumer products with passage of the Federal Hazardous Substances Act
(FHSA). Tobacco products were not specifically excluded, but FDA did not assert
jurisdiction over tobacco products at that time. In 1972, authority for FHSA was
transferred to the newly created Consumer Products Safety Commission (CPSC).
The agency was sued in 1974 for failure to consider a petition to set upper limits
on tar in cigarettes. Federal court subsequently ruled the CPSC must consider the
petition. Within 6 weeks of this decision, Congress amended the FHSA specifi-
cally excluding tobacco products, including cigars.
In 1970, Congress passed the Controlled Substances Act to prevent the abuse
of drugs, narcotics and other addictive substances. The law specifically excluded
tobacco and tobacco products from the definition of a “controlled substance” in
21 U.S.C. 802 (Cigar Association of America, 1986) thus excluding cigars. In
1976, Congress enacted the Toxic Substances Control Act and it also excluded
tobacco and tobacco products from the definition (15 USC 802C6). A summary
of Federal regulatory policies for tobacco products is included in Table 1. A
summary of state policies is included in Table 2.
In 1996, the FDA declared that nicotine in cigarettes and smokeless tobacco
was a drug and asserted jurisdiction over these products as devices for delivery of
Chapter 8
222
Table 1
Federal policies on tobacco products
Cigarettes Smokeless Tobacco Cigars
1. Labeling Requirements Package and Print Ads Package and Print Ads None
Four Rotational Three Rotational
Health Warnings Health Warnings
2. Advertising Restrictions Prohibits Advertising Prohibits Advertising Prohibits Little Cigar
on TV and Radio on TV and Radio Advertising on TV and
Radio
3. Report to Congress Biennial Biennial None
4. Nicotine/Toxic
Constituent Disclosure Nicotine, Tar, CO Nicotine None
5. Additive Reporting Confidential List Confidential List None
to DHHS to DHHS
6. Regulation as a
Drug Delivery Device FDA FDA None
7. Youth Access Synar Amendment Synar Amendment Synar Amendment
FDA 21CFR801 FDA 21CFR801
8. Taxation $0.24 Per Pack of 20 $0.027 per
container
0.00125 small cigar
(1.2 oz
) 12.75% of wholesale
price of large cigar but
not more than $0.03 a
cigar
Note: Department of Health and Human Services (DHHS)
Food and Drug Administration
Table 2
State and local policies on tobacco products
Cigarettes Smokeless Tobacco Cigars
1. Labeling Requirements Preempted Preempted California
2. Advertising Restriction Preempted Preempted None
3. Nicotine Disclosure MA, TX MA, TX TX
4. Nicotine/Toxic
Constituent Reporting MA, TX, MN MA, TX, MN TX, MN
5. Youth Access
6. Taxation 50 States 42 States 41 States
(average #0.317 per (40 state average of (36 state tax average
pack or 37.8% or 25.3% of wholesale 21.7% of wholesale
wholesale price) price) price)

223
Smoking and Tobacco Control Monograph No. 9
the drug nicotine; however, the agency did not assert jurisdiction over cigars. In
the proposed rule, little cigars were included, but deleted in the final rule that
cited insufficient evidence of use by children and insufficient evidence that cigars
were drug delivery devices under the act, as well as differences in definition of
little cigars and cigarettes for tax purposes.
1
HEALTH WARNINGS There is no Federal law requiring health warnings on cigars. At the
State level, California adopted in 1986 the Safe Drinking Water and Toxic
Substances Enforcement Act that required warnings on products that contain
chemicals that cause cancer or reproductive risks. In response to the threat of
litigation, cigar manufacturers and retailers agreed to place the following warning
label on cigars sold in the state: “Warning: This product contains/produces
chemicals known to the state of California to cause cancer and birth defects or
other reproductive harm.” Manufacturers of cigars also print the California
warnings on the packages of manufactured cigars sold nationally. Cigars sold
singly generally do not bear the California warning outside of the state.
DISCLOSURE OF CIGAR Following passage of the Federal Cigarette Labeling and
OR SMOKE PRODUCT Advertising Act in 1965, the Federal Trade Commission (FTC)
CONSTITUENTS developed a machine system for measuring tar and nicotine
yield of cigarettes and provided, in an annual report to
Tar, Nicotine, and CO Congress, the yields of tar and nicotine as the most popular
brands (Pillsbury et al., 1969). The system was not designed to predict actual tar
and nicotine intake among humans, only to provide a relative measure between
brands. The system was modified in 1981 to include carbon monoxide (CO).
Cigarette manufacturers disclose tar and nicotine yield of their brands in adver-
tisements under a 1971 consent agreement with the FTC. Cigarette manufactur-
ers generally list tar and nicotine levels on packages of low-yield cigarettes, but
not on packages containing cigarettes with greater than 8 milligrams of tar.
Cigar manufacturers are not required to report tar, nicotine, and CO content
of their products to the Federal Government. Texas and Minnesota require
nicotine reporting of cigars. The International Committee for Cigar Smoking
Studies, which represents cigar manufacturers, concluded that it is technically
possible to smoke cigars by machine (International Committee, 1974). However,
the committee notes that, given the range in cigar size and variability of the
products, it is very difficult to produce valid tar deliveries, and that ranking cigars
by tar content is virtually meaningless and of minimal value to the consumer.
Texas requires cigar manufacturers to disclose nicotine yield of its products
to the Department of Health based on standards to be adopted by the Depart-
ment (Vernon’s Texas Codes Annotated, 1998). Minnesota requires cigar manu-
facturers to disclose “hazardous substances contained in the burned or unburned
state, which may include certain components of tar and carbon monoxide”
(Minnesota Secretary of State Office, 1997). Massachusetts also requires compa-
nies to report nicotine yield of cigarettes and smokeless tobacco products to
consumers based on what the user is expected to take within the body.
1
44424-federal regulation vol. 61 no. 168 8/28/80.

Chapter 8
224
.
Small cigars and packaged cigars bear the following statement on the
package in response: “These cigars are predominantly a natural tobacco with
non-tobacco ingredients added.” This has been done in response to California
law (Wilson, 1988). Cigar manufacturers are not required by Federal law to
disclose added constituents or nicotine and tar contents. The manufacturers have
neither voluntarily developed a protocol nor voluntarily disclosed their addi-
tives.
Added Ingredients Cigarette manufacturers are required to report ingredients added to
tobacco to the Secretary of the Department of Health and Human Services
(DHHS). The list does not provide the level of the additive or the brand that it is
placed in, and is kept confidential by DHHS. DHHS is authorized to report to
Congress on its research on additives and health risks, but has yet to do so since
it received the authority in 1984. DHHS has no authority to regulate or remove
harmful additives.
When the FDA asserted jurisdiction over cigarettes and smokeless tobacco as
drug delivery devices, it considered requiring disclosure of ingredients added to
these products, but decided not to do so. The comprehensive Smokeless Tobacco
Health Education Act of 1986 requires similar ingredient reporting to DHHS for
smokeless tobacco products and requires manufacturers to report nicotine yield,
but does not require nicotine content to be listed on advertisements or packages.
Cigarette and smokeless tobacco manufacturers voluntarily released their list of
additives in 1994 in response to public concerns. Cigar manufacturers have not
done so.
Massachusetts requires cigarette and smokeless tobacco manufacturers to file
an annual report with the Department of Public Health that lists added ingredi-
ents by brand in descending order by weight or other measure (Phillips, 1997).
Cigars are not included.
Texas requires reporting of ingredients added to cigars and Minnesota
requires reporting of constituents in the cigar or cigar smoke that are on the
state’s “hazardous substances” list.
ADVERTISING Federal advertising restrictions on cigarettes and smokeless tobacco
RESTRICTIONS products include the prohibition of electronic advertising, including
television, radio, and any other form of electronic communication regulated by
the Federal Communications Commission (FCC). Cigarettes and smokeless
tobacco are not directly advertised by large manufacturers on the Internet,
however, there are over 150 cigar websites on the Internet, many of which sell or
advertise cigars (Cigar Association of America, 1986).
In 1973, the Little Cigar Act (PL93-109) banned broadcast advertising of
“Little Cigars” defined as “any roll of tobacco wrapped in leaf tobacco or any
substance containing tobacco as to which one thousand units weigh not more
than 3 pounds.” The ban did not extend to large cigars and cigarillos which can
still be advertised on electronic medium today.

225
Smoking and Tobacco Control Monograph No. 9
The advertising and promotion of cigarette and smokeless tobacco products
have also been restricted through voluntary measures, adopted by their respective
trade associations, the Tobacco Institute and the Smokeless Tobacco Council,
ostensibly to protect children from being encouraged to smoke or use smokeless
tobacco. The codes have a number of similar provisions, such as prohibiting
models in ads who appear to be under the age of 25, not to associate smoking
with glamour, physical fitness, or wealth, and not to place brand-name tobacco
products in movies. As described in Chapter 7, cigar manufacturers’ advertising
and promotion of cigars have not adhered to those voluntary codes (Falit, 1997).
If the codes were strictly applied to cigar advertising, current cigar advertising
and promotion would be severely restricted. Famous actors and athletes, includ-
ing Demi Moore, Arnold Schwartzenegger, and Wayne Gretsky promote cigar use
(Chapter 7). Major themes presented in cigar advertisements include wealth,
athletic fitness, and sexual attractiveness. The tobacco industry stopped market-
ing of cigarettes on college campuses in the 1960’s. A recent story in Smoke
magazine describes emerging cigar social clubs on college campuses (Barry, 1997).
REGULATION OF An earlier chapter of this monograph reports on cigar smoking and
CIGAR SMOKING environmental tobacco smoke (ETS) generated by cigar use (Chapter 5).
IN PUBLIC PLACES
Early restrictions on cigarette smoking included bans on cigars and pipes. In
1971, the Civil Aeronautics Board (CAB) restricted cigarette smoking on airlines
to a limited number of seats, and at the same time banned cigar and pipe smok-
ing entirely.
States and local jurisdiction have extensively regulated cigar smoking as part
of ordinances that have restricted cigarette smoking. More completed reviews of
state and local ordinances are available in an earlier monograph in this series
(Monograph 3) and from the Centers for Disease Control and Prevention (State
Tobacco Highlights, 1996). In general, cigars are more strictly regulated than
cigarettes by these ordinances, probably because of the greater irritation and
annoyance produced by cigar smoke.
LITIGATION Cigarette and smokeless tobacco manufacturers have been sued by ,
individuals classes of persons, and the majority of states for the alleged harm
their products have caused to consumers and for the related health costs of
treating tobacco related diseases.
The Culbro Corporation, a major cigar manufacturer, has been named in
seven suits in Florida since 1995, although it was served in only four cases. In
each case, Culbro was voluntarily dismissed as a defendant. One of the suits in
which the company was named but not served as a defendant was a class action
suit claiming that the plaintiffs were addicted and harmed by cigar smoking.

Chapter 8
226
A principal defense made by tobacco manufacturers in the litigation is that
consumers have been adequately warned of the harm that cigarettes can cause
through health warning labels and are knowledgeable about the risks associated
with cigarette smoking. Cigarette manufacturers argue that consumers voluntar-
ily assume the risks and therefore they should not be held accountable. Cigarette
manufacturers have acknowledged that smoking is a risk factor for certain
diseases although they argue the association is not causal. Cigar manufacturers,
on the other hand, are not required to place health warnings on their products,
except in California. The failure of cigar manufacturers to place warnings on all
of their products, coupled with the marketing of their products, may place them
at risk of liability in the future.
RESTRICTIONS ON At the Federal level, the FDA adopted a regulation on August 23, 1996,
YOUTH ACCESS TO to prohibit the sale of cigarettes and smokeless tobacco products to
CIGARS persons under 18, as well as to restrict advertisements and
promotions directed toward youth. The FDA rule does not include cigars. The
Federal Alcohol, Drug Abuse and Mental Health Act was amended in 1992 to
include a requirement for states to establish 18 years of age as the minimum age
for the purchase of tobacco products. If a state did not establish such a require-
ment, the state would not receive full funding for Federal substance abuse block
grants. Cigars are included in this Act.
TAXATION In 1864, Congress passed a law placing an excise tax on tobacco
Federal Tax of Cigars products, and in the following year collected 11.4 million dollars in
revenue, with only .1 percent coming from cigarette taxation. By 1920, cigarettes
accounted for almost half of the 58 million dollars collected at the Federal level,
and in 1996, cigarettes represented 98 percent.
The current Federal tax on cigars (Table 3) is broken into two categories.
Small cigars are taxed at $1.125 per thousand or approximately one tenth of a
cent per small cigar. The small cigar is defined as having a weight no more than
3 pounds per 1,000 units, and resembling cigarettes in size and weight. The
Federal tax on a package of 20 cigarettes is 24 cents while the tax on 20 small
cigars is about one tenth that or 2.25 cents for 20 small cigars.
The tax on large cigars (cigars weighing more than 3 pounds per thousand) is
12.75 percent of the wholesale price, but not more than $30.00 per thousand. At
this rate, there is a maximum tax of 3 cents per cigar. Based on this weight
classification, cigarillos, manufactured, and premium cigars, would all be classi-
fied as large cigars.
The estimated average manufacturers price for a package of five cigarillos is
$0.60 per package or $120.00 per thousand. Based on that amount, the tax at
12.75 percent for 1,000 would be $16.20 or $1.62 per cigarillo. The estimated
wholesale price of the manufactured cigar is 36 cents per cigar, or $360.00 per
thousand. If the thousand were taxed at 12.75 percent, the resulting tax would
be $51.00 per thousand above the maximum taxable level of $30.00 per thou-
sand.

227
Smoking and Tobacco Control Monograph No. 9
The Federal tax on a typical manufactured or premium cigar would therefore
be limited to 3 cents per cigar. This tax scheme is particularly favorable to
manufacturers of premium cigars whose very costly cigars can only be taxed at a
maximum of 3 cents per unit. Thus as price increases due to inflation or de-
mand, Federal tax diminishes as a percent of price. Table 3 summarizes the
Federal taxes on different types of cigars and Table 4 compares the tax rate for
cigarettes and various types of cigars as a percent of the wholesale price.
Table 4
Wholesale price and federal tax per pound of various tobacco products
Wholesale Price per Federal Tax per Tax as a %
Products Pound of Tobacco Pound of Tobacco of Wholesale Price
Cigarettes $19.05 $3.432 28.6%
Small Cigar $15.87 $0.51 3.2%
Tiparillo $19.66 $1.95 12.75%
Manufactured Cigar $19.21 $1.59 8.3%
Premium Cigar $34.09 $0.68 2%
Table 3
Estimated weight, price, and federal tax per 1,000 pounds of tobacco products
Tobacco Product
(weight Est. Weight/Thousand Price/Thousand Fed Tax/Thousand %Tax
Wholesale Price) Units Units Units of Price
Small Cigars
(1 gram @$0.035 each) 2.205 lbs. $35.00 $1.125 3.2%
Tiparillos
(3 grams @$0.12 each) 6.614 lbs. $120.00 $15.30 12.57%
Manufactured Cigars
(8.5 grams @$0.36 each) 18.74 lbs. $360.00 $30.00 8.3%
Premium
(20 grams @$1.50 each) 44.100 lbs. $150.00 $30.00 2%
Cigarettes
(1 gram @$0.042 each) 2.205 LBS. $42.00 $12.00 28.6%

Chapter 8
228
State Taxation of Cigars As of January 1, 1996, the number of states taxing cigars was
41, with 36 placing a single average tax of 21. 7 percent on the manufacturers’ or
wholesalers’ price (Table 5). Five states have a tax system similar to that of the
Federal Government that have multiple rates according to the weight or price of
the cigar. Of the 36 states with the single rate, Washington has the highest tax of
74.9 percent of the wholesale price, and North Carolina the lowest, 2 percent.
Ten states had rates higher than 25 percent, and 26 lower. By comparison, 50
states tax cigarettes at an average tax of 31.7 cents per pack or 37 percent of the
wholesale price of $84.00 per thousand. Forty states tax smokeless tobacco at an
average rate of 25.3 percent of the wholesale price. According to the Tobacco
Institute, 337.2 million dollars in gross tax revenue was generated from state
taxation of tobacco products other than cigarettes in 1996. This represents 4.8
percent of the total tax revenue from all tobacco products.
In recent years, there has been an increasing trend at the state level to
impose taxes on tobacco products other than cigarettes. In 1970, 21 states taxed
cigars and the number remained virtually constant up until 1995 (22 states).
However, by 1990, the number of states rose to 33 and by 1996 was 41 states.
Not only did the number of states taxing cigars increase, but also the rate in-
creased by almost 30 percent from 1983 to 1996. In 1983, 14 states levied a flat
rate on the wholesale price of cigars of 21.3 percent. By 1996, the same states
increased the average rate 28.2 percent. Total state tax revenue for tobacco
products other than cigarettes increased from $32.6 million in 1975 to $62.3
million in 1985, and today is $337.2 million. In 1975, other tobacco products
made up 3.4 percent of all tobacco tax revenue at the state level, and by 1996
rose to 4.8 percent. Table 5 summarizes the taxation of cigars by individual
states.
All 50 states and the District of Columbia have enacted some form of legisla-
tion with respect to the sale of cigars to minors. According to NCI’s State Cancer
Legislative Database, through November 1997, 29 states and DC explicitly
prohibit the sale of cigars to minors. The remaining states prohibit the sale of
tobacco products to minors, implicitly covering cigars (Table 6).
In conclusion, the number of states taxing cigars has increased sharply over
the last 10 years, and the vast majority tax cigars as a percent of wholesale price.
Such a tax structure will result in an increase in revenue as cigar prices go up.
This is the opposite of the Federal system which sets a maximum rate of 3 cents
per large cigar. Thus as the price of large cigars increase, the proportion of tax on
the price decreases.

229
Smoking and Tobacco Control Monograph No. 9
Table 5
State tax rates on cigars
State Tax rates States with no tax rates
on cigars
Alabama Cigars, retailing for: District of Columbia
(a) 3 1/2 cents each or less, $1.50 per thousand; Florida
(b) More than 3 1/2 and not more than 5 cents each, $3.00 per thousand; Kentucky
(c) More than 5 and not more than 8 cents each, $4.50 per thousand; Maryland
(d) More than 8 and not more than 10 cents each, $7.50 per thousand; Pennsylvania
(e) More than 10 and not more than 20 cents each, $15 per thousand; Virginia
(f) More than 20 cents each, $20.25 per thousand. West Virginia
Little Cigars: 2 cents for each 10 or fraction thereof. Wyoming
Alaska 75% of wholesale price.
Arizona Cigars retailing for:
(a) 5 cents each or less, 6.4 cents for each 3 cigars;
(b) More than 5 cents, 6.4 cents each
Little cigars: 12.9 cents for each 20 or fraction thereof.
Arkansas 23% of manufacturers' invoice price.
California 29.37% of wholesale price effective 7/1/97-6/30/98.*
Colorado 20% of manufacturers' price.
Connecticut 20% of wholesale price – all OTP.
Delaware 15% of wholesale price.
Georgia Little cigars: weighing not more than 3 pounds per 1,000: 2 mills each.
All other cigars: 13% wholesale price.
Hawaii 40% of wholesale price.
Idaho 40% of wholesale sales price.
Illinois 18% of wholesale price.
Indiana 15% of wholesale price.
Iowa 22% effective 6/1/91 of wholesale sales price.
Kansas 15% of original invoice price from the manufacturer to the wholesaler.
Louisiana Cigars with a list price of $120 per thousand or less, tax is 8% of net invoice price;
Cigars with a list price of over $120 per thousand, tax is 20% of net invoice price.
Maine 16% of wholesale sales price.
Massachusetts 15% of wholesale price.
Michigan 16% of wholesale price.
Minnesota 35% of wholesale price.
Mississippi 15% of manufacturers' list price.
*CA reset at the beginning of each fiscal year.

Chapter 8
230
Table 5 (
Continued
)
State tax rates on cigars
State Tax rates States with no tax rates
on cigars
Missouri 10% of manufacturers' price.
Montana 12.5% of wholesale price.
Nebraska 15% of wholesale price.
Nevada 30% of wholesale price.
New Jersey 48% of wholesale price.
New Mexico 25% of product value.
New York 20% of wholesale price – all OTP.
North Carolina 2% of wholesale price.
North Dakota 28% of wholesale price.
Ohio 17% of wholesale price.
Oklahoma Cigars, cheroots, stogies, etc., weighing more than 3 pounds
per thousand, retailing for:
(a) 4 cents each or less, $10 per thousand;
(b) More than 4 cents each, $30 per thousand;
Little cigars: 2 cents for each 8 or fraction thereof.
South Dakota 10% of wholesale price.
Tennessee 6% of wholesale price.
Texas Tax on cigars is based on weight per 1,000 and retail selling price.
(a) Cigars weighing not more than 3 pounds per 1,000, 1 cent for each 10 cigars;
(b) Cigars weighing more than 3 pounds per 1,000 and retailing for not more
than 3.3 cents each, $7.50 per 1,000;
(c) Cigars of all descriptions weighing more than 3 pounds per 1,000 and
retailing for over 3.3 cents each, containing no substantial amount of
nontobacco ingredients, $11.00 per $1,000;
(d) Cigars of all description weighing more than 3 pounds per 1,000 and
retailing for over 3.3 cents each, containing a substantial amount of
nontobacco ingredients, $15.00 per $1,000.
Utah 35% of manufacturers' selling price exclusive of any trade discount,
special discount, or deal.
Vermont 41% of distributors' price.
Washington 74.9% of wholesale price.
Wisconsin 20% of wholesale price.
Source: Tobacco Institute, Washington, D.C.

231
Smoking and Tobacco Control Monograph No. 9
Table 6
States with laws prohibiting the sale of cigars to minors
(Through November 30, 1997)
State Type of Prohibition State Type of Prohibition
Alabama
2
* Montana *
Alaska * Nebraska x
Arizona * Nevada x
Arkansas x New Hampshire *
California x New Jersey x
Colorado * New Mexico x
Connecticut x New York *
Delaware * North Carolina x
District of Columbia * North Dakota *
Florida x Ohio x
Georgia x Oklahoma *
Hawaii x Oregon x
Idaho * Pennsylvania x
Illinois * Rhode Island *
Indiana * South Carolina x
Iowa x South Dakota *
Kansas * Tennessee x
Kentucky x Texas *
Louisiana * Utah *
Maine x Vermont *
Maryland * Virginia *
Massachusetts x Washington x
Michigan * West Virginia *
Minnesota * Wisconsin *
Mississippi * Wyoming *
Missouri *
Source: National Cancer Institute, State Cancer Legislative Database, Bethesda, MD: SCLD
Legend: * Denotes states that have enacted laws explicitly prohibiting the sale of cigars to minors
x Denotes states that have enacted laws prohibiting the sale of tobacco/tobacco products to minors
2
Alabama does not prohibit the sale of cigars or tobacco products to minors; instead the purchase of cigars by minors
is prohibited.

Chapter 8
232
CONCLUSIONS
1. There is less Federal and State regulation of cigars when compared to
cigarettes and smokeless tobacco. The Synar Amendment is the only Federal
statute, outside of the tax codes, that specifically includes cigars.
2. The voluntary codes restricting marketing practices established by the
tobacco trade associations are regularly violated by cigar advertising and
promotional activities.
3. Federal tax rates selectively favor premium cigars over other cigars and
tobacco products, by capping the tax rate at 3 cents per cigar.
4. With the exception of warnings mandated by California’s Proposition 65,
cigars do not carry warning labels.
REFERENCES
Barry, S.T. Collegiate smokes. Smoke 2(2): 138-150,
1997.
Cigar Association of America, Inc. Cigar Advertising
Standards. Washington, DC: Cigar Association of
America, Inc., 1986.
Falit, J.L. Cigar advertising targeting “baby-boomers”
and other adults. Tobacco Control, 6:240-242, 1997.
Federal Register, Vol. 61 No.168, 8/28/80, p. 44424.
International Committee, p. 4, 1974.
Minnesota Secretary of State Office. Minnesota General
Laws Chapter 227 H.F. No. 117. Minneapolis:
Minnesota Secretary of State Office, 1997.
Neuberger, M.D. Smoke Screen: Tobacco and the Public
Welfare. Englewood Cliffs, New Jersey: Prentice-Hall,
1963.
Phillips, F. Cigarette statute is upheld. Boston Globe,
February 8, 1997.
Pillsbury et al. Cigar Smoking Studies, p. 3, 1969.
Centers for Disease Control and Prevention. State Tobacco
Highlights. Washington, DC: Centers for Disease
Control and Prevention, 1996.
Vernon’s Texas Codes Annotated. Disclosure of Ingredients
in Cigarettes and Tobacco Products. Vol.1: Health and
Safety. St. Paul: West Group, pp.192-194, 1998.
Wilson, D.S. Cigars and pipe tobacco to get warning
labels. New York Times, October 19, 1988.
